
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 5
Severe encephalitis complicated by intracranial hypertension and incipient uncal herniation in a 41-year-old woman: A case report
Celeste Bonomi D’Imperio; Rafael Suárez Del Villar Carrero*
Emergency Department, HM Montepríncipe University Hospital, Boadilla del Monte, Madrid 28660, Spain.
*Corresponding Author : Del Villar Carrero RS
Emergency Department, HM Montepríncipe University Hospital, Boadilla del Monte, Madrid 28660, Spain.
Email: rsuarezdelvillar@hmhospitales.com
Received : Oct 14, 2024
Accepted : Nov 05, 2024
Published : Nov 12, 2024
Archived : www.jcimcr.org
Copyright : © Del Villar Carrero RS (2024).
Abstract
We present a case of a 41-year-old female who developed encephalitis complicated by increased intracranial pressure (HTIC) and incipient uncal herniation. The patient presented with fever, headache, and progressive loss of consciousness. Brain imaging revealed a right temporo-insular lesion with associated signs of HTIC. She underwent emergency decompressive craniectomy followed by intensive multidisciplinary care. While the clinical presentation and radiological findings were consistent with herpetic encephalitis, PCR confirmation through Cerebrospinal Fluid (CSF) analysis was not possible due to insufficient sample collection. This case highlights the importance of early diagnosis and aggressive management in cases of encephalitis complicated by HTIC, even when etiological confirmation is limited.
Keywords: Encephalitis; Intracranial hypertension; Uncal herniation; Decompressive craniectomy; Intensive care.
Citation: D’Imperio CB, Del Villar Carrero RS. Severe encephalitis complicated by intracranial hypertension and incipient uncal herniation in a 41-year-old woman: A case report. J Clin Images Med Case Rep. 2024; 5(11): 3338.
Case presentation
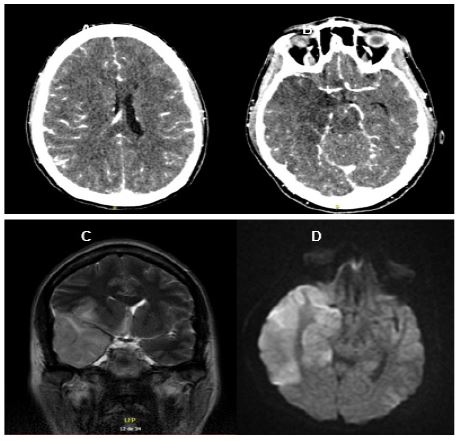
A 41-year-old woman with a medical history of hypothyroidism presented to the emergency department with a 2-day history of fever and progressive decrease in her level of consciousness. Upon arrival, the patient was disoriented, unable to follow simple motor commands, and without meningeal signs. A Computed Tomography (CT) scan of the brain revealed a right temporo-insular lesion with evidence of increased intracranial pressure (HTIC) and signs of incipient uncal herniation (Figure 1).
Given the clinical and radiological findings, the initial differential diagnosis included advanced herpetic encephalitis and a low-grade glioma. Empirical treatment with intravenous acyclovir was initiated, and the patient was admitted to the Intensive Care Unit (ICU) for close monitoring and management of HTIC. Cerebrospinal Fluid (CSF) PCR for Herpes Simplex Virus (HSV) could not be performed due to an insufficient sample, representing a limitation in confirming the diagnosis.
Several microbiological tests were requested to evaluate potential infectious etiologies:
CSF analysis: An attempt was made to perform PCR for HSV and other viral agents; however, the sample obtained was insufficient for processing.
Blood cultures: Negative for bacterial growth.
Serological tests: Evaluations for HIV, Epstein-Barr virus, cytomegalovirus, and other common viral pathogens were negative. However, as the initial clinical suspicion of herpetic encephalitis was high, empirical antiviral treatment with acyclovir was continued.
These microbiological results, along with imaging findings, supported the diagnosis of presumed herpetic encephalitis, although definitive viral confirmation could not be obtained.
Initial laboratory findings showed mild anemia (hemoglobin 11.0 g/dL, normal range: 12.3-15.3 g/dL) and leukocytosis with neutrophilia (leukocytes 14.35x103/μL, neutrophils 11.34x103/μL). Coagulation parameters, including prothrombin time and international normalized ratio (INR), were within normal ranges. However, a mild metabolic alkalosis was observed in arterial blood gases (pH 7.51, pCO2 30 mmHg).
Follow-up laboratory tests on day 5 revealed a decline in hemoglobin to 9.6 g/dL and persistent neutrophilia (9.38x103/μL). Coagulation studies indicated slight prolongation of prothrombin time (INR 1.21), but fibrinogen remained within the upper normal limit (437 mg/dL). Metabolic parameters such as sodium and potassium remained stable, with no significant electrolyte disturbances (sodium 132.5 mmol/L, potassium 4.84 mmol/L). Further arterial blood gas analysis continued to demonstrate metabolic alkalosis (pH 7.45, pCO2 35 mmHg).
Upon admission, the patient’s initial CT scan revealed a right temporo-insular lesion with significant midline shift and sulcal effacement, indicating severe brain edema and early signs of uncal herniation (Figures 1A,1B). Follow-up MRI demonstrated high-intensity signals on T2-weighted and FLAIR sequences, particularly in the temporal lobes, which are characteristic of herpes simplex encephalitis (Figure 1C). Additionally, DWI MRI highlighted regions of restricted diffusion, confirming cytotoxic edema and neuronal damage (Figure 1D).
The patient’s clinical course improved progressively, allowing her transfer from the ICU after 17 days. Upon discharge, she had regained functional independence for activities of daily living (communication, eating, and personal hygiene) but had residual bradypsychia, mild-to-moderate left hemiparesis, and left homonymous hemianopia.
Discussion
Herpes Simplex Encephalitis (HSE) remains the most frequent cause of sporadic necrotizing encephalitis, with a mortality rate of approximately 70% without treatment [1]. The introduction of acyclovir has dramatically improved survival, reducing the mortality rate to 15%. However, many survivors still experience significant long-term neurological disabilities [2]. Advances in Magnetic Resonance Imaging (MRI) have played a crucial role not only in diagnosing HSE but also in predicting outcomes. Recent studies have shown that abnormalities in more than three brain lobes and left thalamic lesions are associated with worse functional outcomes, particularly in patients over 60 years old [3].
The diagnosis of HSE relies heavily on the detection of herpes simplex virus DNA in cerebrospinal fluid via polymerase chain reaction, which has high sensitivity and specificity [4]. However, it is essential to initiate antiviral treatment as soon as possible, even before PCR confirmation. Studies indicate that starting acyclovir within the first four days of symptom onset significantly improves patient outcomes, reducing the likelihood of severe long-term sequelae [5].
Seizures at presentation have been identified as a major prognostic factor for poor outcomes in HSE patients, as they increase the risk of severe neurological impairment [6]. In cases of severe HSE requiring admission to intensive care units, multidisciplinary management, including decompressive craniectomy for patients with intracranial hypertension, has proven effective in improving survival and reducing permanent neurological damage [7].
In recent cohort studies, early MRI scans revealed that extensive brain damage, particularly in critical areas like the thalamus and frontal lobes, is a key predictor of poor outcomes at 90 days, confirming the role of neuroimaging in guiding treatment and prognosis [8]. Machine learning models have also been applied to enhance prediction accuracy, particularly for severe cases with bilateral diffusion abnormalities, which are strongly linked to poor functional outcomes [9].
Conclusion
This case highlights the critical importance of rapid diagnosis and intervention in severe encephalitis complicated by HTIC. Decompressive craniectomy, in combination with antiviral therapy and multidisciplinary care, proved to be an effective strategy for preventing irreversible neurological damage and improving patient outcomes. While microbiological confirmation of HSV was not possible in this case, empirical treatment based on clinical and imaging findings was crucial. Further studies are needed to explore the most effective management strategies in similar cases, particularly in those with severe complications such as uncal herniation.
References
- Practical Neurology. Viral infections of the central nervous system: An update on herpes simplex virus, varicella-zoster virus, and enterovirus D68. Practical Neurology. 2023.
- Assessment of Magnetic Resonance Imaging Changes and Functional Outcomes among Adults with Severe Herpes Simplex Encephalitis. JAMA Neurology. 2020.
- Herpes simplex encephalitis: High mortality and the role of neuroimaging. Journal of Neurology, Neurosurgery & Psychiatry. 2023.
- Management of Encephalitis: Clinical Practice Guidelines. Clinical Infectious Diseases. 2021.
- Clinical characteristics and outcomes of patients with Herpes Simplex Encephalitis in Vietnam: A retrospective study. BMC Infectious Diseases. 2021.
- Prognostic factors for severe outcome in herpes simplex encephalitis: analysis from a multicenter study. BMC Infectious Diseases. 2022.
- Neurological sequelae after herpes simplex encephalitis: A cohort study. Critical Care Medicine. 2020.
- Herpes simplex encephalitis MRI findings and patient outcomes in severe cases. JAMA Network Open. 2023.
- Advanced imaging techniques in HSE prognostication: Machine learning approaches. Critical Care Medicine. 2023.