
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Series - Open Access, Volume 5
Application of nafamostat mesylate anticoagulation in hemodialysis of uremia patients with active bleeding: Clinical experience and a literature review
Ting Wang1*; Xiao Liu2; Ziyan Tang2; Weihong Bi1; Yangling Zhang1; Xiaoqing Ye1; Ziyan Luo2
1Department of Nephrology, The Third Hospital of Mian Yang (Sichuan Mental Health Center), Mian Yang 621000, Si Chuan, China.
2Affiliated Hospital of North Sichuan Medical College, Nan chong 637000, Si Chuan, China.
*Corresponding Author : Ting Wang
Department of Nephrology, The Third Hospital of Mian Yang (Sichuan Mental Health Center), Mian Yang 621000, Si Chuan, China.
Email: 21917708@qq.com
Received : Oct 20, 2024
Accepted : Nov 06, 2024
Published : Nov 13, 2024
Archived : www.jcimcr.org
Copyright : © Wang T (2024).
Abstract
Anticoagulation is one of the most important techniques to ensure the progress of hemodialysis. Uremia patients are often prone to hemorrhagic diseases, making it very difficult to choose anticoagulant regimens used for maintenance hemodialysis. The commonly used anticoagulation methods for uremic patients with severe bleeding risk or active bleeding include citric local anticoagulation or no anticoagulant mode. Nafamostat mesylate with a short half-life and multi-target effect to prevent coagulation during extracorporeal circulation has demonstrated its unique advantages in hemodialysis. Here, we present two cases of uremic patients with active bleeding both experienced intolerable metabolic alkalosis when using citrate local anticoagulation. After adjusting the anticoagulant to nafamostat mesylate, the patients’ hemodialysis was finished, and their active bleeding did not worsen. So, we proved the safety and efficacy of nafamostat mesylate as an anticoagulant for hemodialysis. We also provided the experience in selecting anticoagulants when facing uremia patients with severe bleeding risk or active bleeding.
Keywords: Hemodialysis; Nafamostat mesylate; Anticoagulation; Uremia; Active bleeding.
Citation: Wang T, Liu X, Tang Z, Bi W, Zhang Y et. al. Application of nafamostat mesylate anticoagulation in hemodialysis of uremia patients with active bleeding: Clinical experience and a literature review. J Clin Images Med Case Rep. 2024; 5(11): 3339.
Case one
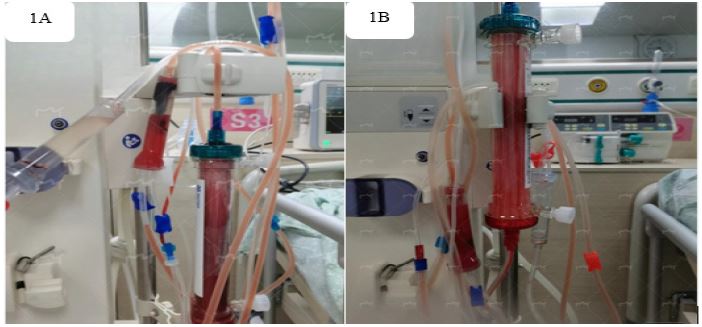
A 93-year-old Chinese woman presented with a 3-year history of maintenance hemodialysis, with dialysis vascular access of the right cervical tunneled cuffed catheter, frequency of 3 times per week, dry weight of 54.5 kg, low molecular weight heparin sodium 4500 IU anticoagulant, and single dialysis ultrafiltration of 1-2 L. The primary cause of renal failure is considered hypertension. 2 hours ago, the patient accidentally fell and felt dizzy complicated with nausea and vomiting two hours before she came to the hospital. A cranial computed tomography revealed a right frontal parietal lobe brain contusion and laceration with hematoma. Physical examination only showed severe hypertension (194/85 mmHg). The laboratory examination showed her hemoglobin, platelet, D-Dimer, prothrombin time, fibrinogen degradation products, blood nitrogen and creatinine were 97 g/L, 259×109/L, 4.21 mg/L, 14s, 9.7 mg/L, 21.49 mmol/L, 699 μmol/L. We adjusted the anticoagulant to replace low molecular weight heparin sodium with citric acid to avoid worsening of cerebral hemorrhage. At the end of treatment, the dialyzer showed grade II-III coagulation using 300 ml of citric acid per hour. The dialyzer still coagulated at II-III level (Figure 1A) and the patient exhibited symptoms of fatigue and numbness in the lips, while the dosage of citric acid was adjusted to 390 ml/h. Arterial blood gas analysis showed pH 7.57, HCO3- 32 mmol/L, pCO2 35 mmHg, pO2 78 mmHg and BE 9 mmol/L. We had to adjust the anticoagulant to nafamostat mesylate, with a dose of 20 mg pre charge and 40 mg/h maintenance. The dialyzer and extracorporeal circulation tubing showed almost no coagulation (Figure 1B). Cranial computed tomography revealed subdural hematoma and fluid accumulation in the right frontal, parietal, temporal, and occipital regions are less absorbed than before after one week later. The laboratory examination showed D-Dimer, prothrombin time, fibrinogen degradation products were 1.27 mg/L, 12.9s, 4.8 mg/L.
Case two
An 81-year-old Chinese woman presented with a 5-month history of maintenance hemodialysis, with dialysis vascular access of the right cervical tunneled cuffed catheter, frequency of 3 times per week, dry weight of 64.8 kg, low molecular weight heparin sodium 3500IU anticoagulant, and single dialysis ultrafiltration of 1-2 L. The primary cause of renal failure is considered type 2 diabetes. She has a 40-year history of hypertension through taking medication to control. She has had a 5-year history of coronary heart disease through taking Aspirin 100 mg and Atorvastatin Calcium 20 mg once a day orally. She suddenly felt nauseous and vomited 150 ml of blood containing blood clots one hour before being sent to the hospital by her son. Physical examination showed poor mental state, damp and cold limbs, anemic appearance and high heart rate (110 beats/minute). The laboratory examination showed her hemoglobin, platelet, D-Dimer, prothrombin time, fibrinogen degradation products, blood nitrogen and creatinine were 70 g/L, 266×109/L, 2.52 mg/L, 13.3s, 6.8 mg/L, 34.91 mmol/L, 776 μmol/L. Immediate treatment was given with pantoprazole, somatostatin for acid suppression and hemostasis, as well as infusion of fresh frozen plasma and removal of white blood cell suspension red blood cells. We adjusted the anticoagulant to 300 ml/h of citric acid. The patient experienced general numbness and discomfort during the treatment. The dialyzer and extracorporeal circulation tubing had no coagulation. Arterial blood gas analysis of the patient showed pH 7.68, HCO3- 25.7mmol/L, pCO2 17 mmHg, pO2 118 mmHg and BE 5 mmol/L. The patient’s symptoms did not improve while we reduced the amount of citric acid to 150 ml/h gradually, but the dialyzer showed grade II coagulation (Figure 2A). Arterial blood gas analysis of this time showed pH 7.65, HCO3-24.8 mmol/L, pCO2 18 mmHg, pO2 86 mmHg and BE 1.5 mmol/L. We had to adjust the anticoagulant to nafamostat mesylate, with a dose of 20 mg pre charge and 25 mg/h maintenance. The dialyzer and extracorporeal circulation tubing showed almost no coagulation (Figure 2B). The laboratory examination showed her hemoglobin, platelet, D-Dimer, prothrombin time, fibrinogen degradation products were 90 g/L, 177×109/L, 7.75 mg/L, 12.5s, 13.8 mg/L. The patient’s hemoglobin was stable without signs of active gastrointestinal bleeding.

Discussion
Chronic kidney disease has become a global public health problem with the aging of the population, the increasing incidence of diabetes, hypertension and other chronic diseases. Uremia is a poor prognosis for chronic kidney disease patients. Maintenance hemodialysis which relies on safe and effective anticoagulation is one of the most important treatments for uremic patients [1,2]. At present, heparins are the most common anticoagulation in hemodialysis, which have the economical and convenient characteristics but not suitable for uremia patients with active bleeding [3]. Bleeding events occur higher in uremic patients undergoing hemodialysis. Chinese expert consensus on the application of anticoagulant technology in renal replacement therapy for critical patients (2023) [4] recommends patients with severe bleeding risk or active bleeding use nafamostat mesylate or citric acid as anticoagulants, and the no anticoagulant mode is only used for patients who are not accessible by other anticoagulant techniques due to its poor effectiveness [5].
Citric acid local anticoagulation has been widely used for maintenance hemodialysis in patients with severe bleeding risk or active bleeding in China [6,7]. The citric acid local anticoagulation significantly improves the completion rate of hemodialysis, and reduces the coagulation events in extracorporeal circulation pipelines and dialyzers. Uremic patients’ ultrafiltration is limited because of using low concentration citric acid as anticoagulation. Citric acid anticoagulation also has complications such as hypocalcemia and metabolic alkalosis [8]. The incidence of adverse events is significantly increased when used in elderly, emaciated, and patients with underlying liver diseases.
The two cases describe the selection process of anticoagulants during hemodialysis in uremia patients with active bleeding. According to expert consensus [4], they have indications for using citric acid for anticoagulation. At the end of the treatment, the dialyzer of the patient in Case 1 showed significant coagulation. And there was no significant improvement in coagulation during the increase in citric acid dosage, while the patient developed symptoms of fatigue and numbness in the mouth and lips, and blood gas analysis indicated metabolic alkalosis which was considered the accumulation of citric acid. The patient in Case 2 developed discomfort symptoms such as general numbness while using a standard dose of citric acid. During the reduction of dose, there was no improvement in these symptoms, but coagulation had already occurred in the extracorporeal circulation tubing. When we adjusted the anticoagulant to nafamostat mesylate, the treatment process went smoothly without coagulation in the extracorporeal circulation pipeline and dialyzer. Follow up on some related indicators showed that patients did not experience any worsening of bleeding [9-12].
Nafamostat mesylate is a serine protease inhibitor that exerts anticoagulant effects by multiple pathways such as inhibiting thrombin, VIIa, Xa, and XIIa [13], inhibiting platelet aggregation [14], prolonging fibrinolysis time [15]. Its half-life is only 5-8 minutes [16], mainly cleared by the blood and liver. It has in vitro anticoagulant characteristic because of its quickly degrades through the liver and blood when a small amount enters the body. In 1988, nafamostat mesylate was used as an anticoagulant in blood purification in Japan [17]. Due to its excellent anticoagulant efficacy for extracorporeal circulation, nafamostat mesylate has become the most commonly anticoagulant for continuous renal replacement therapy in Japanese intensive care units for patients at high risk of bleeding [18]. During maintenance hemodialysis, the dose of nafamostat mesylate entering the body is less than 4% of being used [19], and it can be rapidly degraded in the body with little impact on coagulation function. The bleeding events is much lower than that of systemic anticoagulants [20,21]. And its advantages in anticoagulation are reflected in its simple operation, small impact on platelets and acid-base electrolyte balance. At present, there is limited experience [22-24] in using nafamostat mesylate in China which suggested the advantages of it in blood purification therapy for high-risk bleeding patients. By observing before and after symptoms, clinical manifestations, and related indicators in uremic bleeding patients using nafamostat mesylate as anticoagulant, we further confirmed the safety and efficacy of it. More and more nephrologists are paying attention to its advantages. The latest expert consensus [25] provided a detailed introduction to the pharmacokinetics, clinical indications, usage plans and monitoring, bleeding and coagulation risk assessment, and the application of different blood purification treatment modes of nafamostat mesylate, in order to better guidance for clinical practice and improve the safety and efficacy of its application in blood purification therapy for uremic bleeding patients.
References
- Chinese Society of Nephrology. Guidelines for the anticoagulant management of continuous renal replacement therapy[J]. Chin J Nephrol,2022, 38(11): 1016-1024.
- Sciascia S, Radin M, Schreiber K. et al. Chronic kidney disease and anticoagulation: from vitamin K antagonists and heparins to direct oral anticoagulant agents. Intern Emerg Med.2017,12(8):1101-1108.
- Villa G, Ricci Z, Ronco C. Renal replacement therapy[J]. Crit Care Clin,2015, 31(4):839-848.
- Expert Consensus Working Group. Chinese expert consensus on the application of anticoagulant technology in renal replacement therapy for critical patients (2023) [J]. Chin J Nephrol,2023,39(2): 155-164.
- Zhu Wen-fang, He Jian-qiang, Cao Jun. Clinical application research of citric acid, heparin free, and low-molecular-weight heparin anticoagulation in hemodialysis [J]. Clinical Medicine,2015, 35(5):39-41.
- Shui Guang-xing, Zou Feng, He Dan et al. Application of simplified citrate anticoagulation in patients with high-risk bleeding tendency during hemodialysis [J]. CJITWN, 2021, 22(3): 237-239.
- Ke Xiao-su, Li Yu-wei, Luo Li-xia. Clinical observations on anticoagulant efficacy of high-dose segmented citrate on high-flux hemodialysis [J]. J Clin Nephrol,2021, 21(8):6677-680.
- Tan J N, Haroon S W P, Mukhopadhyay A, et al. Hyperlactatemia predicts citrate intolerance with regional citrate anticoagulation during continuous renal replacement therapy. J Intensive Care Med. 2019; 34(5): 418-425. DOI: 10.1177/0885066617701068.
- Lee Y K, G K S, Oh J, et al. Low-dose nafamostat mesilate in hemodialysis patients at high bleeding risk. Kidney Res Clin Pract. 2011; 30(1): 61-66.
- Yang J W, Han B G, Kim B R, et al. Superior outcome of nafamostat mesilate as an 29/35 anticoagulant in patients undergoing maintenance hemodialysis with intracerebral hemorrhage. Ren Fail. 2009; 31(8): 668-675. DOI: 10.3109/08860220 903180616.
- Miyamoto S, Ogasawara K, Kuroda S, et al. Japan Stroke Society Guideline 2021 for the treatment of stroke [J]. Int J Stroke, 2022,17(9): 1039-1049. DOI: 10.1177/17474930221090347.
- Nobuya Kitamura, Zhang Ling. Nafamostat mesilate in anticoagulation of continuous renal replacement therapy[J]. West China Medical Journal, ,2018,33(07):801-805.
- Koshiyama Y, Ozeki M, Motoyoshi A, et al. Pharmacological studies of FUT-175, nafamstat mesilate. IV. Effects on coagulation, platelets and fibrinolysis [J]. Nihon Yakurigaku Zasshi, 1984, 84(5): 417-428.
- Miyata M, Shirakawa T, Acharya B, et al. Effects of nafamostat mesilate on ADPinduced platelet aggregation and disaggregation in hemodialysis patients [J]. ASAIO J, 2006, 52(3): 272-275. DOI: 10.1097/01.mat.0000209224.94089.bc.
- Matsuoka S, Futagami M, Ohno H, et al. Inhibitory effects of ONO-3307 on various proteases and tissue thromboplastin in vitro and on experimental thrombosis in vivo [J]. Jpn J Pharmacol, 1989, 51(4): 455-463. DOI: 10.1016/s0021-5198(19)40071-
- Okajima K, Uchiba M, Murakami K. Nafamostat mesilate mesilate [J]. Cardiovasc Drug Rev, 2007, 13(1): 51-65. DOI: 10.1111/j.1527-3466.1995.tb00213.x.
- Pak K, Shirasu A, Okino K, et al. Effectiveness of FUT-175, protease inhibitor, as an anticoagulant to hemodialysis [J].Hinyokika Kiyo. 1988,34(6):1077-81.
- Ariumra T, Abe M, Shiga H, etal. Clinical study of blood purification therapy in critical care in Japan: results from the survey research of the Japan Society for Blood Purification in Critical Care in 2013[J]. J Artif Organs,2017,20(3):244-251.
- Matsuo T, Wanaka K. Management of uremic patients with heparin-induced 24 / 35 thrombocytopenia requiring hemodialysis [J]. Clin Appl Thromb Hemost, 2008, 14(4): 459- 464. DOI: 10.1177/1076029607309184.
- Lin Y, Shao Y, Liu Y, et al. Efficacy and safety of nafamostat mesilate anticoagulation in blood purification treatment of critically ill patients: a systematic review and meta-analysis [J]. Ren Fail, 2022, 44(1): 1263-1279. DOI: 10.1080/0886022X.2022.2105233.
- Lazrak H H, Rene E, Elftouh N, et al. Safety of low-molecular-weight heparin compared to unfractionated heparin in hemodialysis: a systematic review and meta-analysis [J]. BMC Nephrol, 2017, 18(1): 187. DOI: 10.1186/s12882-017-0596-4.
- Zhuang Bing, Ye Hong, Cao Hong-di et al. A multicenter, randomized and controlled study of nafamostat mesylate for anticoagulation therapy in hemodialysis[J]. Chin J Blood Purif,2022,21(10):739-743.
- Wu Bu-yun, Liu Kang, Ge Yi-fei, et al. Anticoagulation of nafamostat mesylate for double filtration plasmapheresis: a report of four cases with a literature review [J]. J Clin Nephrol,2023, 23(6):522-525.
- Ao Guang-yu, Huang Lan, Chen Ting-yu et al. Observation on the anticoagulant efficacy and blood concentration of nafamostat mesylate in hemodialysis [J]. Chin J Blood Purif,2023,22(8):579-583.
- Hu Jia-chang, Xie Ye-qing, Shen Bo et al. Expert consensus on application of nafamostat mesilate in anticoagulation for blood purification [J]. Shanghai Medical Journal. https://link.cnki.net/urlid/31.1366.R.20240322.1522.002