
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 5
A rare case of right ovarian hemangioma masquerading as struma ovarii on frozen section analysis
Sai Karthik Bandi1; Arthi Priya Viswanathan2; Deepak Donthi3*
1Department of Pathology, PES Medical College, Kuppam, Andhra Pradesh 517425, India.
22337 SW Archer Rd, apt 2030, Gainesville, FL-32608, USA.
3Clinical Assistant Professor, Department of Pathology, University of Florida, USA.
*Corresponding Author : Deepak Donthi
Clinical Assistant Professor, Department of Pathology, University of Florida, USA.
Tel: +12523475122;
Email: Deepak.donthi@ufl.edu
Received : Oct 16, 2024
Accepted : Nov 06, 2024
Published : Nov 13, 2024
Archived : www.jcimcr.org
Copyright : © Donthi D (2024).
Abstract
Objective: Ovarian hemangiomas although rare (only 70 cases in published literature) can mimic struma ovarii radiologically and during Frozen Section (FS) analysis and they can be associated with other ovarian neoplasms.
Case report: A left ovarian cystic mass and a solid right Ovarian Mass (OM) was seen on ultrasound in a 55-year-old woman. On doppler ultrasound, the right solid OM showed internal septations with minimum vascular flow, and was diagnosed as benign solid lesion. On surgical resection, the FS of the right OM showed multiple micro and macrocystic spaces with pink homogenous material and diagnosed as benign, possible struma ovarii. On microscopy, the left ovarian cyst was a mucinous cystadenoma and right OM was a cavernous hemangioma. Immunohistochemistry confirmed the diagnosis with CD31 positivity in endothelial cells and D2-40 negative.
Conclusion: Although ovarian hemangiomas are rare entities, the radiological and morphological appearance can mimic SO whose surgical management is imperative, unlike benign ovarian hemangiomas.
Keywords: Hemangioma; Ovarian mass; Struma ovarii; Frozen section; Doppler ultrasound; Immunohistchemistry.
Citation: Bandi SK, Viswanathan AP, Donthi D. A rare case of right ovarian hemangioma masquerading as struma ovarii on frozen section analysis. J Clin Images Med Case Rep. 2024; 5(11): 3340.
Introduction
Hemangiomas are benign localized proliferation of small sized blood vessels that can occur at multiple sites of the body such as skin, liver, lungs, bones, retina, etc. Hemangiomas in an ovary is a rare radiological diagnosis in routine gynecologic practice due to their small size and cyclical changes that happen in an ovary of a reproductive woman [1]. There are about 60 or more cases of ovarian hemangioma which have been reported in literature [1]. The age range in which ovarian hemangiomas are diagnosed are from infants to as old as 81 years. Ovarian hemangiomas are incidentally diagnosed ante-mortem during evaluation for other causes for an OM like increased CA-125, adnexal torsion, Meig’s syndrome or post mortem during an autopsy [1]. They can sometimes present associated with hemangiomas of the other sites of the body [2]. Histologically if they appear as multiple thin walled dilated vessels then it is cavernous type. If there are capillary arteries aggregate then capillary type or some can have a combination of cavernous and capillary type called as mixed type [3]. Often the cavernous type is the most common type found in the ovary [2]. Most ovarian hemangiomas are seen in the ovarian hilar region. However, larger hemangiomas extend to the adjacent medulla [4].
Here we will discuss a 55-year-old patient, who presented with an acute abdominal pain and histopathological examination was diagnosed as ovarian hemangioma with contralateral ovarian mucinous cystadenoma. This case is interesting for many reasons such as it was radiologically and FS diagnosis as a possible SO in FSs which could be in the differential. The case report was prepared in accordance to CARE reporting guidelines.
Case presentation
A 55-year-old female presents with incidental mass in January 2024 showing a 7.2x6.4 cm left complex cystic OM identified on a CT scan. Tumor markers like CEA (1.3), CA19-9 (7), CA125 (11.8), inhibin B <7.0 are all within normal limits. The decision was made to conservatively watch and follow-up the patient.
Three months later she developed severe acute onset of left lower quadrant pain. Pelvic examination shows fullness in the left adnexa. CT scan performed in this visit shows bilateral cysts. Ultrasound performed shows a right ovarian solid OM measuring 4.9x3.2x2.4 cm which was isoechoic with minimal positive vascular flow on doppler ultrasound. The left ovary was 8.4x 7.3x4.9 cm cystic lesion with internal echoes and multiple internal septations which was favored to be a benign cyst with hemorrhage. There was minimal vascular flow in the septations. There was also some free fluid within the pelvis.
A robotic assisted laparoscopic bilateral salpingo-oophorectomy was performed and 10 cm left ovarian complex cyst with features of torsion was retrieved. On FS, it was diagnosed as mucinous neoplasm with no evidence of borderline tumor or malignancy. The right ovary grossly was a 5 cm complex solid cystic on cross sectioning which showed micro and macro cystic as shown in the images (Figure 1) and was diagnosed as benign, possible SO, but final diagnosis deferred to permanent sections.
Grossly left OM was 324.5 gram, 8.9x7.0x0.7 cm cystic OM which surface was surgically disrupted. No solid components or excrescences are identified in the outer surface. Sectioning reveals the multiloculated mass which contains mucinous fluid with no papillary excrescences or solid components on the inner surface. The cystic wall thickness ranges in size from 0.1 to 0.4 cm.
Grossly the right ovary shows a well-circumscribed, dark brown and adjacent to an outer rim of normal-appearing ovarian parenchyma and measures 2.5x2.1x2.0 cm. No papillary excrescences are identified on the outer ovarian wall or in the cystic foci. The fimbriated fallopian tube has purple-tan, smooth and glistening serosa and does not appear to be involved by the tumor.
The right ovarian tissue shows large dilated thin walled congested blood vessels with a well circumscribed mass. The blood vessels were lined by endothelium which are engorged with blood (Figure 2). The immunohistochemical markers show positivity for CD31 and negative for D2-40 (Figure 3). The lesional tissue was present with leydig cell clusters which were SF-1 positive but stromal cells were negative for SF-1. Microscopically the left ovary showed a cyst wall lined by single lined mucinous epithelium which was diagnosed as a mucinous cystadenoma (Figure 4).
Table 1: Table representing clinicopathological data of the patients reported with ovarian hemangioma and co-existing lesions in the peer reviewed published literature.
| Author(s),year, title | Age(years) | Symptom | Size (cm) | Type ofhemangioma | Clinical issues | Coexistinglesions | Luteinization |
|---|---|---|---|---|---|---|---|
| Lawhead et al.1985 | NA | NA | NA | NA | Abdominopelvic hemangiomatosis Thrombocytopenia | NA | NA |
| Yamawaki Tet al. 1996 | 62 | Pelvic mass | Cavernous | Ascites | NA | NA | |
| Mirilas P et al.1999 | 8 | Acute abdominal pain | NA | Cavernous | Ovarian torsion | NA | NA |
| Jurkovic I et al.1999 | 32 | Asymptomatic | NA | NA | NA | Mucinouscystadenoma | ER/PR –ve |
| Gehrig PA et al.2000 | 39 | NA | NA | Capillary type withanastomosing pattern | Massive ascites, ElevatedCA-125 | NA | NA |
| Kaneta Y et al.2003 | NA | NA | NA | NA | Pseudo-meigs syndrome (pleuraleffusion) with elevated CA-125 | NA | NA |
| Akbulut et al.2008 | 65 | Irregular vaginal bleeding, pelvic pain | 0.5 | Capillary | NA | Serous papillary carcinoma | ER/PR-ve |
| Comunoglu C et al. 2010 | 81 | Asymptomatic | 3.5 | Cavernous | Hypertension, hyponatremia | Mature cysticteratoma | NA |
| Haung RS et al.2013 | 77 | Left lowerabdominalfullness and pressure | Right side-2.1Left side-0.6 | Capillarytype withstromal luteinization | Hyperandrogenism | NA | NA |
| Mitra B et al.2013 | 22 | Lower abdominal pain | 4.5 | Capillary and cavernous | NA | A follicle cyst | NA |
| Kefelı M et al.2014 | 10 | NA | 9.8 | Cavernous | NA | Dysgerminoma | NA |
| Ekanayake CDet al.(14) 2020 | 43 | Heavymenstrual bleeding, Secondary dysmenorrhea | 6 | NA | NA | Mucinous cystadenoma, Maturecystic teratoma | NA |
| Shopov ST et al.2020 | 74 | NA | NA | Mixed type with stromal luteinization | NA | Serous cystadenoma | ER/PR – ve |
| Correia S et al.2022 | 61 | Hirsutism, hair loss,masculinization of voice, 3 kg weight gain | 3.7 | Anastomosing type withstromal luteinization | Clitoromegaly , Bilateral adrenal adenomas (1.3 cms), Increased levels of 17-OHP | NA | NA |
| Neshat S et al.2023 | 48 | Shortness of breath, chest pain, Heavy menstrual bleeding | 4 | Cavernous | Recurrent pleuraleffusion | NA | NA |
| Current case | 55 | Lower abdominal pain | 4.9 | Cavernous | NA | Mucinouscystadenoma | NA |
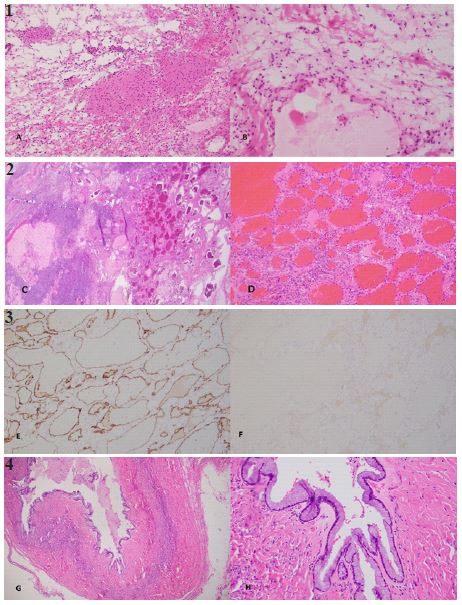
Figure 2(C,D): H&E (4x) and (20x) shows numerous dilated vascular spaces engorged with blood lined with thin endothelium, adjacent to normal ovarian tissue, no cellular atypia seen.
Figure 3(E,F): CD31 immunohistochemical stain under 10x shows positivity for vascular endothelial cells and D2-40 immunohistochemical stain under 10x shows negativity for vascular endothelial cells, respectively.
Figure 4(G,H): Microscopic study with H&E 4x and (20x) shows ovarian cyst wall lined by single layer of mucinous epithelium with basally placed nuclei, no cellular atypia or stratification seen, consistent with mucinous cystadenoma.
Discussion/conclusion
Ovarian hemangiomas are benign vascular tumors which mimic other benign ovarian lesions and ovarian cancers. The etiology of the ovarian hemangiomas is unknown similar to cutaneous hemangiomas [1]. Miliaras et al found that endothelial cells were ER, PR positive in their case [5]. Although, a few hypotheses which suggest hormonal effects and presence of hyperestrogenism leading to stimulatory growth factor in vessels as controversial causes [6]. Few propose that a pre-existing hemangioma like hamartomas or congenital malformations or neoplasms which becomes larger as ovarian hemangiomas induce stromal luteinization through mass effect resulting in androgen production with unopposed conversion to estrogen [7]. This estrogen is postulated to cause proliferation of an existing hemangioma.
The clinical presentation of ovarian hemangiomas is often nonspecific, with the majority of cases being asymptomatic. However, when symptomatic, unilateral abdominal pain is the most common presenting symptom, with bilateral presentation being rare. Initially, in our case similar to others, OM was detected incidentally. On a subsequent visit, our patient presented with unilateral acute abdominal pain requiring the necessity for further imaging studies. Other symptoms if associated with large hemangiomas may include abdominal distension, pelvic discomfort, menstrual irregularities and vomiting, etc. Due to their nonspecific symptoms and rarity, ovarian hemangiomas can mimic other more common ovarian pathologies, such as ovarian endometriomas or ovarian malignancies, posing diagnostic challenges [8].
Ultrasound is typically the initial imaging modality used for the evaluation of ovarian masses. On ultrasound, ovarian hemangiomas may appear as predominantly hyperechoic, predominantly solid, well defined mass with increased vascular flow on doppler imaging [9]. Some cases have shown hypoechoic to anechoic with few showing a complex cystic mass [10]. In our case the lesion was a solid well circumscribed, isoechoic mass with positive vascular flow. Low resistant vascular flow pattern on doppler might mimic a malignant lesion, requiring additional imaging for characterization of the lesion. Although CT scan with contrast can vaguely highlight septations in a mass with differentiation of a cystic versus solid lesion, it might not completely help in identification of a hemangioma [1,11]. Therefore, definitive diagnosis often requires histopathological examination of surgical specimens obtained through biopsy or excision.
Clinically and radiologically the differential diagnosis can include benign ovarian neoplasms like monodermal teratoma like struma ovari, endometrioma, ovarian torsion, peripheral arterior-venous malformation and malignant tumors like sex cord stromal tumors, angiosarcoma, epithelioid hemangioma [12,13]. It is hard to differentiate ovarian hemangiomas from ovarian malignancy with the ultrasound, elevated CA-125 and gross findings although there are very rare cases of mucinous cystadenoma associated with elevated CA-125 [14], these levels were normal in our case raising a diagnostic challenge. The stromal luetinization and the hyperandrogenism mimics the presentation of solid leydig cell tumors as well the increased levels of CA-125 reported in some cases according to the literature [7]. A variant of hemangiomas which had overlap of sinusoidal and hobnail hemangiomas of skin and soft tissue is anastomosing hemangioma which can overlap with well differentiated angiosarcomas.
Histologically, teratomas can be in the differential diagnosis due to the presence of prominent vasculature [15]. Lymphangiomas are close differential diagnosis in which the cells lining the lymphatic spaces are positive for D2-40. A true hemangioma from enlarged hilar blood vessels of the ovary, as the true hemangioma is usually a circumscribed mass of dilated vascular channels with minimal amount of stroma [13]. Similar to our case few studies have performed immunohistochemical markers like CD31 and CD34 highlighting endothelial cells lining the vascular channels.
Ovarian hemangiomas are often associated with other benign and malignant ovarian lesions on the contralateral ovary. Some ovarian hemangiomas are associated with clinical issues like thrombocytopenia, torsion and pseudo-meig’s syndrome, elevated CA-125 levels and a few with stromal luteinization, endometrial hyperplasia [3,5,11]. There are many studies that show co-existing lesions in the contralateral ovary as discussed in (Table 1). Our case also presented with torsion of the ovary.
In summary, ovarian hemangiomas are rare benign vascular tumors of the ovary that can present diagnostic challenges due to their nonspecific symptoms and rarity. Early recognition and accurate diagnosis are crucial for appropriate management and optimal patient outcomes. Further research is needed to better understand the etiology, pathogenesis, and optimal management strategies for these rare tumors.
Having around just over 60 cases reported in the literature, further research towards understanding the etio-pathogenesis, associations with other ovarian tumors and optimal management strategies for these rare tumors is imperative. The differential diagnosis for ovarian hemangiomas clinically, radiologically and histologically demonstrates a diagnostic challenge, additionally highlighting the importance of reporting such rare lesions.
Conflict of interest: The authors have no conflicts of interest to disclose
References
- Ramos H, Thummala N, Jacques SM, Gogoi R. A rare case of ovarian hemangioma in a 30-year-old nulligravid woman. Radiol Case Rep. 2023; 18(2): 613-9. doi: 10.1016/j.radcr.2022.10.100.
- Dahal M, Upadhyaya P, Adhikari P, Karki D, Regmi N. Ovarian Hemangioma: A rare entity. International Journal of Reproduction, Contraception, Obstetrics and Gynecology. 2018. doi: 10.18203/2320-1770.ijrcog20182023.
- Huang RS, Covinsky M, Zhang S. Bilateral ovarian capillary hemangioma with stromal luteinization and hyperandrogenism. Ann Clin Lab Sci. 2013; 43(4): 457-9.
- McHenry A, Buza N. Anastomosing Hemangioma of the Ovary with Leydig Cell Hyperplasia: A Clinicopathologic Study of 12 Cases. International Journal of Gynecological Pathology. 2023; 42(2): 167-75. doi: 10.1097/pgp.0000000000000887.
- Mirilas P, Georgiou G, Zevgolis G. Ovarian cavernous hemangioma in an 8-year-old girl. Eur J Pediatr Surg. 1999; 9(2): 116-8. doi: 10.1055/s-2008-1072225.
- Ziari K, Alizadeh K. Ovarian Hemangioma: a Rare Case Report and Review of the Literature. Iran J Pathol. 2016; 11(1): 61-5.
- Gehrig PA, Fowler WC Jr, Lininger RA. Ovarian capillary hemangioma presenting as an adnexal mass with massive ascites and elevated CA-125. Gynecol Oncol. 2000; 76(1): 130-2. doi: 10.1006/gyno.1999.5648.
- Hafsi M, Moussi M, Najar S, Dridi F, Maroua S, et al. Ovarian hemangioma: Differential diagnosis of ovarian cancer. Int J Surg Case Rep. 2024; 116: 109431. doi: 10.1016/j.ijscr.2024.109431.
- Qi Y, Zhuang L, Zhu T. Ultrasonography Findings in Ovarian Hemangiomas: Report of Three Cases and Review of the Literature. Reproductive Sciences. 2024. doi: 10.1007/s43032-024-01656-y.
- Gunduz M, Hurdogan O, Onder S, Yavuz E. Cystic Anastomosing Hemangioma of the Ovary: A Case Report With Immunohistochemical and Ultrastructural Analysis. Int J Surg Pathol. 2019; 27(4): 437-40. doi: 10.1177/1066896918817148.
- Correia S, Oliveira MJ, Wen X. Ovarian Hemangioma with Stromal Luteinization. Cureus. 2022; 14(9): e29438. doi: 10.7759/cureus.29438.
- Wang Z, Hu J. A case report of anastomosing hemangioma of the ovary. Medicine. 2023; 102(19): e33801. doi: 10.1097/md.0000000000033801.
- Mitra B, Sengupta S, Rai A, Mehta J, Quader AR, et al. Ovarian haemangioma: A rare case report. Int J Surg Case Rep. 2013; 4(11): 981-4. doi: 10.1016/j.ijscr.2013.07.029.
- Ekanayake CD, Munasinghe N, Kumarasinghe I, Rasnayake S. Elevated CA 125 level in a mucinous cystadenoma and a teratoma: A case report. J Med Case Rep. 2020; 14(1): 141. doi: 10.1186/s13256-020-02458-x.
- Akbulut M, Bir F, Çolakoğlu N, Soysal ME, Düzcan SE. Ovarian hemangioma occurring synchronously with serous papillary carcinoma of the ovary and benign endometrial polyp. Annals of Saudi Medicine. 2008; 28(2): 128-31. doi: doi:10.5144/0256-4947.2008.128.