
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 5
A patient with massive splenomegaly and its cause unfound
Elanaz Alizade*; Yasir Furkan Çağin; Ali Alizade
1Internal Medicine Assistant, Inonu University, Turkey.
2Gastroenterology, Inonu University, Turkey.
3Emergency Medicine, Battalgazi Hospital, Turkey.
*Corresponding Author : Elanaz Alizade
Internal Medicine, Inonu University, Turkey.
Email: pineapple31952@gmail.com
Received : Oct 20, 2024
Accepted : Nov 07, 2024
Published : Nov 14, 2024
Archived : www.jcimcr.org
Copyright : © Alizade E (2024).
Abstract
The most common causes of splenomegaly are liver disease, malignancy, and infection. 84% of cases with progressive splenic enlargement were associated with hematological diseases, especially malignancy. Acute infections, anemia, and splenic rupture are the most common complications of splenomegaly. Hereditary Spherocytosis (HS) is the most common red cell membrane disorder. Morphologically, spherocytes are round red cells that have lost the ability to change shape. Hereditary spherocytosis is a common inherited disease characterized by anemia, jaundice and splenomegaly. A 28-year-old male patient applied to the emergency service with complaints of abdominal pain and jaundice for 20 days. In the patient’s abdominal usg, the spleen was measured as 21 cm. Etiology investigation was done for the patient’s splenomegalism. Viral hepatitis was negative. His past infections were examined and no disease except toxoplasma igg was detected. EBV, CMV values were negative. No pathological findings were detected in the peripheral blood spread. It was thought that splenomegaly may be due to hereditary spherocytosis, but a definitive diagnosis could not be made.
Keywords: Splenomegaly; Cytopenias; Hereditary spherocytosis.
Citation: Alizade E, Çağin YF, Alizade A. A patient with massive splenomegaly and its cause unfound. J Clin Images Med Case Rep. 2024; 5(11): 3341.
Introduction
The spleen is the largest organ of the lymphatic system. The spleen’s functions include removing aging or abnormal blood cells, storing platelets and red blood cells, producing and distributing immune cells and antibodies. The spleen is a secondary lymphoid organ that can affect the progression of many diseases, especially liver cirrhosis. The spleen may fill with blood when there is increased pressure due to parenchymal liver disease (e.g., fibrosis, cirrhosis). The exact mechanism is unknown. Reduced blood flow caused by vascular obstruction (e.g., portal, hepatic, or splanchnic vein thrombosis) can cause the spleen to enlarge due to increased pressure.
The most common causes of splenomegaly are liver disease, malignancy, and infection. 84% of cases with progressive splenic enlargement were associated with hematological diseases, especially malignancy. Infectious diseases were associated with liver diseases with fever and abnormal liver function tests, hepatomegaly, and thrombocytopenia or leukopenia.
Patients with splenomegaly and lymphadenopathy mostly had hematological malignancies. Although not so specific that other diagnoses can be excluded, these features may still contribute to the clinician’s overall diagnostic impression. Acute infections, anemia, and splenic rupture are the most common complications of splenomegaly. There may be symptoms of cytopenias due to hypersplenism. General systemic symptoms such as fever, sweats, weight loss or lymphadenopathy suggest haematological, malignant, infectious or inflammatory disease. One-third of patients with splenomegaly have cirrhosis; abnormal liver parenchyma leading to congestive splenomegaly.
Hereditary spherocytosis
Hereditary Spherocytosis (HS) is the most common red cell membrane disorder. Morphologically, spherocytes are round red cells that have lost the ability to change shape.
Hereditary spherocytosis is a common inherited disease characterized by anemia, jaundice and splenomegaly. Compensated hemolytic anemia is observed in most patients. Some individuals are asymptomatic, while others have severe hemolytic anemia requiring red blood cell transfusion.
In hereditary spherocytosis, it is the loss of membrane surface area and leads to reduced deformability due to defects in the membrane proteins ankyrin, band 3, β spectrin, α spectrin, or protein 4.2. Splenectomy is curative but should be performed after careful evaluation of risks and benefits. Osmotic fragility tests have poor sensitivity because approximately 20% of cases of mild hereditary spherocytosis are missed.
Case presentation
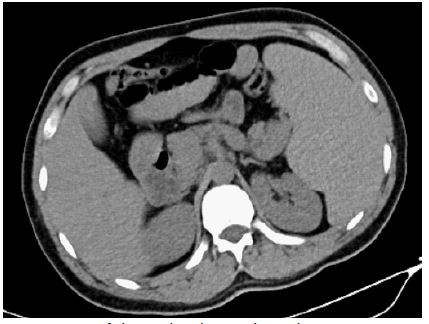
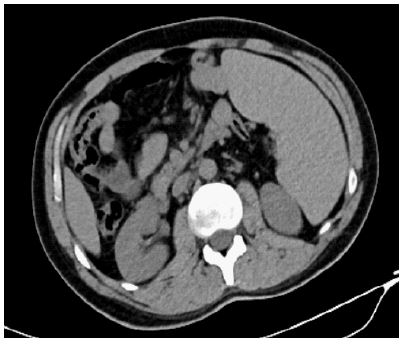
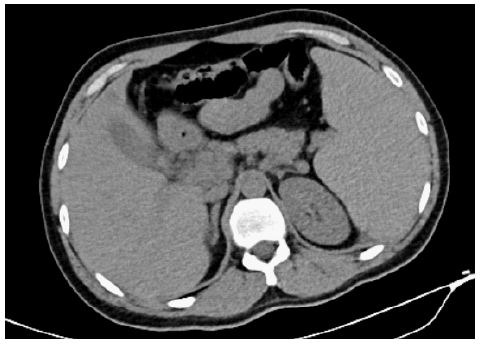
A 28-year-old male patient applied to the emergency service with complaints of abdominal pain and jaundice for 20 days. In the patient’s abdominal usg, the spleen was measured as 21 cm.
Lab test
Total bilirubin 28,49 mg/dl
Direct bilirubin 14,51 mg/dl
AST 205 U/L
ALT 273 U/L
ALP 216 U/L
GGT 517 IU/L
LDH 318 U/L
WBC 8.32x103/UL
Hemogram 11.40 g/dl
Platelet 165x103/ul
INR 1.1
The patient was admitted to the intensive care unit and plasmapheresis was performed. After plasmaphresis applied, the patient’s bilirubin values decreased. The patient was transferred from the intensive care unit to the service. Bilirubin values were monitored and the patient was consulted with the hematology department during this process. Peripheral blood spread and bone marrow aspiration was done to the patient by the hematologist. Etiology investigation was done for the patient’s splenomegalism. Viral hepatitis was negative. His past infections were examined and no disease except toxoplasma igg was detected. EBV, CMV values were negative. No pathological findings were detected in the peripheral blood spread. The patient continued to be hospitalized for approximately 15 days and birubin values remained stable at around 6 mg/dl. Osmotic fragility test was requested for the patient where hematology and gastroenterology cannot find the etiology of splenomegaly. The patient was in good condition and was discharged. The patient’s follow-ups are continued by the hematology. Birubin values are around around 6 mg/dl. Hereditary fragility test was high.
Patient’s latest lab test
Total bilirubin 5.95 mg/dl
Direct bilirubin 0.75 mg/dl
AST 20 U/L
ALT 16 U/L
ALP 75 U/L
GGT 58 IU/L
LDH 239 U/L
WBC 9.13x103/UL
Hemogram 13.40 g/dl
Platelet 218x103/ul
INR 1.12
The pathology result of the bone marrow aspiration test did not have any pathological findings. In the last abdomen usg result, spleen was reported as 19 cm. It was thought that splenomegaly may be due to hereditary spherocytosis, but a definitive diagnosis could not be made. The patient’s general condition is good and he continues his routine checks.
Discussion and conclusion
The most common causes of splenomegaly are liver disease, malignancy, and infection. 84% of cases with progressive splenic enlargement were associated with hematological diseases, especially malignancy. Hereditary spherocytosis is a common inherited disease characterized by anemia, jaundice and splenomegaly. Compensated hemolytic anemia is observed in most patients. Some individuals are asymptomatic. A 28-year-old male patient applied to the emergency service with complaints of abdominal pain and jaundice for 20 days. In the patient’s abdominal usg, the spleen was measured as 21 cm. Etiology investigation was done for the patient’s splenomegalism. Viral hepatitis was negative. His past infections were examined and no disease except toxoplasma igg was detected. EBV, CMV values were negative. No pathological findings were detected in the peripheral blood spread. It was thought that splenomegaly may be due to hereditary spherocytosis, but a definitive diagnosis could not be made.
Conflict of interest: The authors declare that there is no conflict of interest.
References
- Pozo AL, Godfrey EM, Bowles KM. Splenomegaly: Investigation, diagnosis and management. Blood Rev. 2009.
- Aldulaimi S, Mendez AM. Splenomegaly: Diagnosis and Management in Adults. Am Fam Physician. 2021.
- Cesta MF. Normal structure, function, and histology of the spleen. Toxicol Pathol. 2006.
- Li L, Duan M, Chen W, Jiang A, Li X, et al. The spleen in liver cirrhosis: revisiting an old enemy with novel targets. J Transl Med. 2017.
- Perrotta S, Gallagher PG, Mohandas N. Hereditary spherocytosis. Lancet. 2008.