
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 5
Spontaneous thoracic epidural hematoma presenting with delayed neurological deficits
Niragh Sikdar*; Subhranil Mal; Spandan Hansda
Kolkata Medical College & Hospital, Kolkata, India.
*Corresponding Author : Niragh Sikdar
Kolkata Medical College & Hospital, Kolkata, India.
Email: niraghsikdar@gmail.com
Received : Sep 25, 2024
Accepted : Nov 08, 2024
Published : Nov 15, 2024
Archived : www.jcimcr.org
Copyright : © Sikdar N (2024).
Abstract
Spontaneous Spinal Epidural Hematoma (SEH) is a rare cause of acute spinal cord compression, with an estimated incidence of 0.1 per 100,000 patients annually. This case report describes a 63-year-old male who presented with a 10-day history of severe lower back pain, right foot numbness, and right lower limb weakness, without any history of trauma or relevant comorbidities. MRI revealed a D8-D11 epidural lesion causing spinal cord compression, diagnosed as spontaneous Spinal Epidural Hematoma (SEH). The patient underwent emergency D9-D11 laminectomy and hematoma evacuation, with perioperative management complicated by antiplatelet medication use. Postoperatively, the patient showed significant neurological improvement. This case highlights the importance of considering SEH in patients with acute back pain and neurological deficits, even without typical risk factors. It emphasizes the crucial role of prompt MRI diagnosis and surgical intervention, while also illustrating the challenges in managing patients on antiplatelet therapy. The delayed presentation underscores the potential for missed diagnosis in such cases.
Citation: Sikdar N, Mal S, Hansda S. Spontaneous thoracic epidural hematoma presenting with delayed neurological deficits. J Clin Images Med Case Rep. 2024; 5(11): 3344.
Introduction
An accumulation of blood in the space between dura and bone is the called an epidural hematoma. There are two types of epidural hematomas: spinal and intracranial. Spinal Epidural Hematoma (SEH) is most common after trauma but it may also present spontaneously. Other associated factors include blood disorders, anticoagulation medicines, malignancy, and AVMs [1]. SEH usually presents with sudden onset of neck pain, radicular pain, back pain followed by symptoms and signs of rapidly evolving nerve root and spinal cord compression [2]. The rate of mortality was reported to be ranging anywhere from 5% to 50%. For patients with neurological deficits, immediate decompressive laminectomy and hematoma evacuation has been recommended [3]. The preoperative neurologic status may help predict the outcome of surgical treatment in a patient with spinal epidural hematoma [4]. Our case was a rare occurrence. The reason we are sharing this case report is to alert physicians towards the need for further investigation of the problem even if there are no risk factors or any potential explanation for lower limb weakness or back discomfort in affected individuals [5].
Case presentation
A 63-year-old male, presented to the emergency room with sudden onset of severe pain in his lower back, experiencing since ten days prior to admission. This pain was followed by numbness in his right foot and an inability to sense or move his right lower limb. Additionally, he had difficulty extending his knee and experienced two episodes of vomiting. Upon admission, he was diagnosed with a D9-D11 spinal extradural hematoma with cord compression.
During the initial evaluation, it was noted that patient had no history of diabetes, hypertension, coronary artery disease, or asthma. A general examination revealed decreased sensation below the umbilicus, 4/5 power in both lower limbs, and absent bladder control. His vital signs were stable, and a range of biochemistry tests, including serum albumin, alkaline phosphatase, and bilirubin levels, were within normal limits.
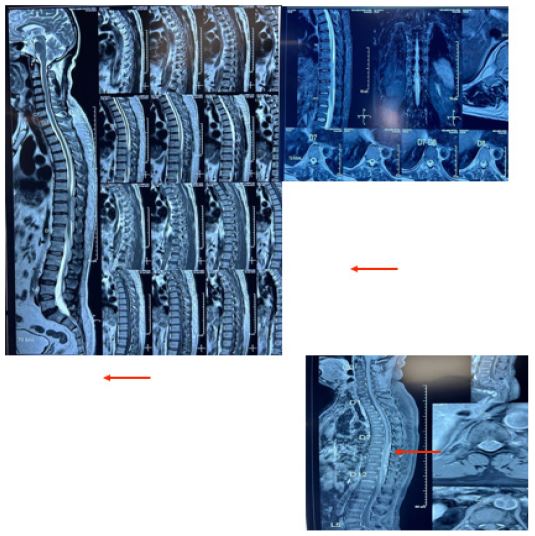
An MRI of the lumbar spine revealed a well-circumscribed epidural lesion at the D8-D11 vertebral level, causing compression and anterior displacement of the spinal cord. The lesion, indicative of an epidural hematoma, measured approximately 6.4 x 1 x 6.1 cm and displayed mixed signal intensity on MRI sequences. No invasion or erosion of adjacent vertebrae was observed, and other parts of the spine showed minor issues such as mild disc bulges and a loss of cervical and lumbar lordosis.
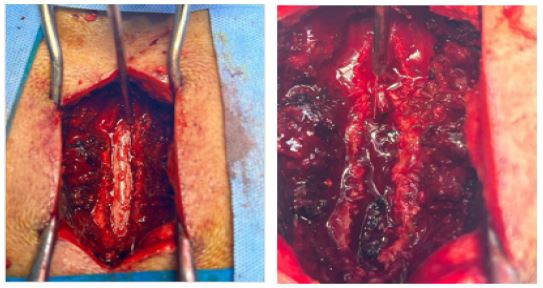
Given the severity of his condition, an emergency D9-D11 laminectomy and microsurgical evacuation of the hematoma were planned and performed. Prior to surgery, due to his intake of antiplatelet medication, patient underwent platelet transfusion. Informed consent and pre-anesthesia assessments were completed, and the surgery proceeded without complications. The procedure included a laminectomy, decompression of the spinal cord, and removal of the epidural clot, which was sent for histopathological examination. Hemostasis was achieved using Floseal and Surgicel, followed by the application of Gelfoam.
Post-operatively, patient was extubated on the operating table and transferred to the Neuro-ICU. He received antiplatelets as per cardiologist advice and was gradually stabilized. On the third post-operative day, his surgical drain was removed, and he was mobilized with the assistance of a physiotherapist. He tolerated oral intake well, regained normal bladder function, and showed overall symptomatic improvement.
Treatment included antibiotics, analgesics, neuroprotectives, antiplatelets, and supportive medications. After showing significant improvement and hemodynamic stability, he was discharged with advice to follow up for suture removal. His discharge prescription included medications such as Ecosprin, Brilinta, and Prolomet XL, with specific dosages and instructions for administration.
The discharge summary emphasized the need for continued follow-up with cardiologists and urologists, alongside maintaining a normal diet and adhering to the prescribed medication regimen. Patient was also advised to seek immediate medical attention if symptoms like fever, new or worsening pain, vomiting, breathing difficulty, altered consciousness, discharge from the wound, or any other significant concerns arose. Patient’s condition at discharge was stable, marking a successful recovery from the spinal hematoma and its associated complications
Discussion
This case report presents a rare occurrence of spontaneous spinal epidural hematoma in a 63-year-old male patient, highlighting the importance of prompt diagnosis and surgical intervention in managing this potentially life-threatening condition.
Spontaneous spinal epidural hematoma is an uncommon cause of acute spinal cord compression, with an estimated incidence of 0.1 per 100,000 patients per year [5]. While often associated with trauma, anticoagulation therapy, or underlying medical conditions, the patient’s case is notable for its apparently spontaneous onset in the absence of clear risk factors.
The patient’s presentation with sudden onset of severe lower back pain, followed by neurological deficits, is consistent with the typical clinical picture of spontaneous spinal epidural hematoma [6]. However, the ten-day interval between symptom onset and hospital admission underscores the potential for delayed diagnosis, which can significantly impact patient outcomes.
Magnetic Resonance Imaging played a crucial role in diagnosis, revealing a well-circumscribed epidural lesion causing spinal cord compression. This aligns with current literature emphasizing MRI as the gold standard for diagnosing spontaneous spinal epidural hematoma due to its superior soft tissue contrast and ability to delineate the extent of the hematoma [7].
The decision to perform emergency decompressive surgery was based on the patient’s neurological deficits and imaging findings. This approach is supported by current guidelines recommending immediate surgical intervention for patients with neurological compromise [8]. The favorable outcome in the case, with significant post-operative improvement, reinforces the efficacy of timely surgical management.
An interesting aspect of this case was the management of the patient’s antiplatelet medication. The pre-operative platelet transfusion and post-operative continuation of antiplatelets as per cardiologist advice highlight the delicate balance required in the perioperative management of patients with spontaneous spinal epidural hematoma an underlying medical conditions.
Conclusion
This case report highlights the importance of prompt diagnosis and surgical intervention in the management of spontaneous spinal epidural hematoma, a rare but potentially life-threatening condition. Clinicians should maintain a high index of suspicion for this diagnosis in patients presenting with sudden-onset severe back pain and neurological deficits, and should have a low threshold for obtaining MRI to confirm the diagnosis and guide appropriate treatment.
References
- David SL. Epidural Hematoma, Medscape. 2018. https://emedicine.medscape.com/article/1137065-overview.
- Lo CC, Chen JY, Lo YK, Lai PH, Lin YT. Spontaneous spinal epidural hematoma: A case report and review of the literatures. Acta Neurol Taiwan. 2012; 21(1): 31-34.
- Binder DK, Sonne DC, Lawton MT. Spinal epidural hematoma. Neurosurg Q. 2004; 14: 519. doi: 10.1097/00013414-200403000-00009.
- Foo D, Rossier AB. Preoperative neurological status in predicting surgical outcome of spinal epidural hematomas. Surg Neurol. 1981; 15(5): 389-401. doi: 10.1016/0090-3019(81)90178-6.
- Sheng OC, Wu RC, Chang IH. Spontaneous spinal epidural hematoma: a case report. Int J Emerg Med. 2021; 14(1): 60. doi:10.1186/s12245-021-00379-0.
- Baek B S, Hur J W, Kwon K Y, Lee H K. Spontaneous Spinal Epidural Hematoma. Korean Neurosurgical Society. 2008; 44(1): 40-40. https://doi.org/10.3340/jkns.2008.44.1.40.
- Shah J A, Patel N N, Michael K W. Spontaneous Spinal Epidural Hematoma: An Atypical Clinical Presentation and Discussion of Management. CIG Media Group. 2020; 14(2): 158-161. https://doi.org/10.14444/7030.
- Hussenbocus S M, Wilby M, Cain C M, Hall D J. Spontaneous Spinal Epidural Hematoma: A Case Report and Literature Review. Elsevier BV. 2012; 42(2): e31-e34. https://doi.org/10.1016/j.jemermed.2008.08.008.