
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 5
The association between quadricuspid aortic valve and ischemic stroke: A case report
Niragh Sikdar*; Subhranil Mal
Kolkata Medical College & Hospital, Kolkata, India.
*Corresponding Author : Niragh Sikdar
Kolkata Medical College & Hospital, Kolkata, India.
Email: niraghsikdar@gmail.com
Received : Sep 25, 2024
Accepted : Nov 11, 2024
Published : Nov 18, 2024
Archived : www.jcimcr.org
Copyright : © Sikdar N (2024).
Abstract
The Quadricuspid aortic valve is a rare congenital heart abnormality characterized by the development of four cusps instead of the normal three in the aortic valve. One of the common complications of this defect is progressive aortic regurgitation. It is extremely rare for a case of the quadricuspid aortic valve to present with ischemic stroke, and the association between them is still not well understood. We explore this association in the case of a 55-year-old man who presented with a 1-week history of left-sided visual loss and paresthesia. He was diagnosed with subacute right parietal occipital ischemic stroke, and subsequently, an electrocardiogram revealed a Quadricuspid aortic valve.
Keywords: Quadricuspid aortic valve; Occipital ischemic stroke; Case report.
Citation: Sikdar N, Mal S. The association between quadricuspid aortic valve and ischemic stroke: A case report. J Clin Images Med Case Rep. 2024; 5(11): 3345.
Introduction
This paper reports a case of Quadricuspid Aortic Valve (QAV), which has been reported in line with the SCARE criteria [1]. QAV is a rare congenital heart defect characterized by the presence of four cusps of varying sizes instead of the typical three symmetrical cusps found in the aortic valve. This anomaly typically arises during the embryological development of the aortic trunk in gestation, with a current reported incidence ranging from 0.013% to 0.043% [2]. Over time, the anatomic configuration of QAV can lead to progressive Aortic Regurgitation (AR). This progression may result in leaflet fibrosis and thickening, leading to issues such as leaflet malcoaptation and AR in affected individuals [3]. Long-standing AR can further manifest as hemodynamic changes, such as left ventricular chamber dilation or decreased left ventricular systolic function [3].
Here, we present a rare case of a Quadricuspid aortic valve defect that presented with a subacute right parietal occipital ischemic stroke. To our knowledge, only two other cases exist that report the occurrence of an ischemic stroke with a Quadricuspid aortic valve [4,5]. The link between the two conditions is not well understood, and further research should be invested in investigating their association.
Case presentation
A 60-year-old male with a history of major depressive disorder and Gastroesophageal Reflux Disease (GERD). There is no significant family history. In addition, the patient smokes, occasionally consumes alcohol about once a month, and has a history of substance abuse with cocaine. He had a history of Cerebrovascular Disease (CVD), which was managed well two years ago.
The patient presented to the clinic on August 1, 2022, complaining of a puzzling neurological condition, such as a 1-week history of visual loss on the left side, occasional headaches, and left-sided paresthesia. A Computerized Tomography (CT) scan of the head revealed an acute to subacute right parietal occipital ischemic stroke. Additionally, a Magnetic Resonance Imaging (MRI) scan of the brain found an acute right posterior cerebral artery stroke and a small left cerebellar infarct. Further investigation led to the discovery of a quadricuspid aortic valve, diagnosed 20 years ago through a transesophageal echocardiogram. The thickened leaflet tips on all four cusps and a probable 1.8 x 1.2 cm mass on one leaflet led to the diagnosis of Type E QAV. Additionally, the diagnosis confirmed moderate Aortic Regurgitation (AR).
On follow-up, his examination revealed that he is well-built and not in any acute discomfort. The echocardiogram revealed no intracardiac thrombus or other cardiac abnormalities, except hypertension, recorded at 140/77 mmHg, normal CV, and pulmonary exams. Based on these findings, we decided not to rule out infective endocarditis. We admitted him and prescribed Vancomycin 1.2 g 12 hourly and Rifampicin 300 mg 8 hourly intravenously for six weeks.
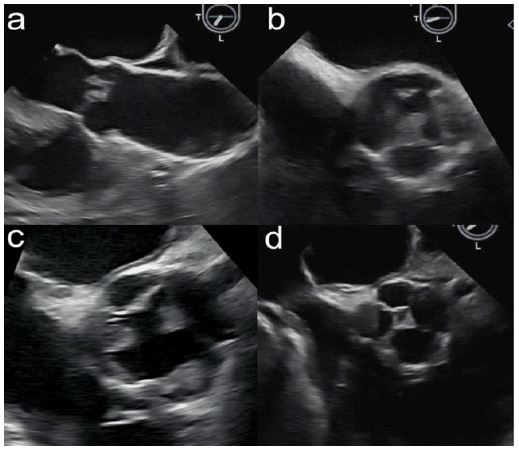
Plane (a) shows the parasternal long-axis view, from which you can observe the left ventricle, left atrium, and mitral valve. Plane (b) shows the parasternal short-axis view at the level of the aortic valve. This plane shows the four cusps that are thickened at the leaflet tips. Plane (c) shows an apical four-chamber view. Here, you can see a section of all four chambers of the heart Plane (d) is another parasternal short-axis view at the level of the aortic valve. This clear image shows thickened leaflet tips on all four cusps with a probable 1.8 x 1.2 cm mass on one leaflet that was not independently mobile. This is suggestive of a Type E quadricuspid aortic valve
Discussion
The congenital aortic Quadricuspid Aortic Valve (QAV) is the least common anomaly of the semilunar valves [6]. QAV is a rare congenital heart disease with an incidence ranging from 0.013% to 0.043% [7]. Tri-leaflet aortic valve is formed by the excavation of the mesenchymal ridge in three areas; however, when one of these three mesenchymal ridges divides to form an additional leaflet, a QAR develops [8]. Other mechanisms suggested include anomalous septation of the conotruncus excavation of one of the valve cushions or the septation of a normal valve cushion as a result of an inflammatory episode [9]. According to Hurwitz and Roberts [10], there are seven anatomical variations (type A-G) of Quadricuspid valves based on cusps size and symmetry. It is reported that QAV can be acquired by diseases such as infective endocarditis and rheumatic fever [11]. The absence of nodules of semilunar cusps can help differentiate between true genetic versus an acquired AQV.
In a case series, it was reported that patients with QAV are likely to develop moderate to severe AR in their late 40s or early 50s [12]. According to an echocardiography database performed on 788,733 patients from January 1, 1975, to March 14, 2014, by Tsang [13], 49 patients were diagnosed with QAV by transthoracic echocardiography. AR was common in 45(90%) patients, of whom 13(26%) had moderate or severe AR, and only 4(8%) patients had aortic stenosis, which was mild in all 4. AR can be caused by primary disease of the aortic valve cusps, abnormalities of the aortic root, and ascending aortic geometry.
Other causes include infective and rheumatic endocarditis, with the vast majority of infectious endocarditis cases with gram-positive streptococci, staphylococci, and enterococci infection. Together, these three groups account for 80% to 90% of all cases, with Staphylococcus aureus specifically responsible for around 30% of cases in the developed world [14,15]. It is also common for QAV to present with other congenital heart defects, such as atrial or ventricular septal defects. Congenital valve abnormalities, including bicuspid aortic valve disease, are considered an intermediate risk of IE. In patients at intermediate risk of IE, antibiotic prophylaxis is not routinely recommended but may be considered on an individual basis [16]. QAV patients may be asymptomatic until the sixth decade, with subsequent symptoms experienced correlating with the valve’s functional status and any associated abnormalities [7]. In a study of 12 cases using the Massachusetts General Hospital echocardiography database, we found that for patients diagnosed with QAV from January 2003 to January 2009, the predominant clinical findings and management issues relate to progressive AR with aging [17].
The novelty, in this case, is the history of cerebrovascular events that this patient has experienced, including aneurysmal subarachnoid hemorrhage, occipital ischemic stroke, an acute right posterior cerebral artery stroke, and a small left cerebellar infarct. To our knowledge, only two other cases report an association between QAV and ischemic strokes [4,5]. In the presented case, the patient has a history of hypertension and mild to moderate AR, and experimental models suggest a causal association between hypertension and AR [18]. However, his hypertension is relatively well controlled as his blood pressure usually remains under 140/80. Another theory suggests that the AR caused by the QAV progressively worsens with leaflet fibrosis and the failure of leaflet coaptation with aging [19]. Although calcified valve disease is considered a “low embolic risk” according to current guidelines, it still remains a significant risk factor to consider in all cerebrovascular events, including ischemic stroke [20].
Currently, the patient has gram-positive bacteremia requiring long-term antibiotics. Aside from the patient’s multiple comorbidities, including QAV, on physical examination, there were no focal neurological deficits, normal CV, and pulmonary exams. A follow-up cardiac MRI will be necessary to investigate the progression, if any, of the aortic valve abnormality and regurgitation to determine if surgical intervention is recommended after antibiotic treatment. Surgery is recommended in symptomatic patients, irrespective of the LVEF, as long as AR is severe [14]. Treatment options typically involve surgical interventions, including tricuspidization, aortic valve reconstruction, or aortic valve replacement with a synthetic valve [21].
Conclusion
This is a novel case of Quadricuspid aortic valve defect that presented with a history of cerebrovascular events, most importantly, occipital ischemic stroke. In this report, we explore the possibility of the association between QAV and cerebrovascular events. Furthermore, this case highlights the need for further research to better understand the mechanism of aortic regurgitation and calcified valve diseases and how they may lead to an increased risk of stroke.
References
- Sohrabi C, Mathew G, Maria N, et al. The SCARE guideline: Updating consensus Surgical Case Report (SCARE) guidelines. Int J Surg. 2023; 109(5): 1136-1140. doi:10.1097/JS9.0000000000000373
- Weerakkody Y, Murphy A, Hacking C, et al. Quadricuspid aortic valve. Reference article, Radiopaedia.org. 2012. https://doi.org/10.53347/rID- 17193.
- Douglas A, Patel A, Batsides G, Safi L. Quadricuspid Aortic Valve: A Rare Cause of Aortic Regurgitation. Case (Phila). 2020; 4(4): 244-247. doi:10.1016/j.case.2020.04.002.
- Krisper M, Köhncke C, Escher F, Morris DA, Tschöpe C, et al. A Patient with Quadricuspid Aortic Valve and Ischemic Stroke. J Heart Valve Dis. 2016; 25(4): 456-458.
- Spartalis M, Tzatzaki E, Spartalis E, et al. Ischemic Stroke in a Patient With Quadricuspid Aortic Valve and Patent Foramen Ovale. Cardiol Res. 2017; 8(4): 169-171. doi:10.14740/cr567w.
- Shadman S, Asadi MS, Nomigolzar S, Sarfarazi M. A Congenital Quadricuspid Aortic Valve Associated With Aortic and Mitral Regurgitation: Case Report and Literature Review. Cureus. 2021; 13(1): e12986. doi:10.7759/cureus.12986.
- Yuan S. Quadricuspid Aortic Valve: A Comprehensive Review. Braz J Cardiovasc Surg. 2016; 31(6): 454-460.
- Aslan E. Unicuspid and quadricuspid aortic valves: Two case reports and literature review. Cardiol Young. 2021; 31(9): 1538-1541. doi:10.1017/S1047951121001153.
- Timperley J, Milner R, Marshall AJ, Gilbert TJ. Quadricuspid aortic valves. Clin Cardiol. 2002; 25(12): 548-552. doi:10.1002/clc.4950251203.
- Hurwitz LE, Roberts WC. Quadricuspid semilunar valve. Am J Cardiol. 1973; 31(5): 623-626. doi:10.1016/0002-9149(73)90332-9.
- Khalid I, Ijaz HM, Choudhry P, et al. Case Series of Quadricuspid Aortic Valve. Cureus. 2022; 14(9): e28888. doi:10.7759/cureus.28888.
- Adeniyi A, Abadir S, Douglass P, Brown C. Late Complication of Quadricuspid Aortic Valve: Early Moderate to Severe Aortic Regurgitation. Cureus. 2022; 14(7): e27312. doi:10.7759/cureus.27312
- Tsang MY, Abudiab MM, Ammash NM, et al. Quadricuspid Aortic Valve: Characteristics, Associated Structural Cardiovascular Abnormalities, and Clinical Outcomes. Circulation. 2016; 133(3): 312-319. doi:10.1161/CIRCULATIONAHA.115.017743.
- Vahanian A, Beyersdorf F, Praz F, et al. 2021 ESC/EACTS Guidelines for the management of valvular heart disease. Eur Heart J. 2022; 43(7): 561-632. doi:10.1093/eurheartj/ehab395.
- Yallowitz AW, Decker LC. Infectious Endocarditis. In: StatPearls. Treasure Island (FL): StatPearls. 2023.
- Delgado V, Ajmone Marsan N, de Waha S, et al. 2023 ESC Guidelines for the management of endocarditis. Eur Heart J. 2023; 44(39): 3948-4042. doi:10.1093/eurheartj/ehad193.
- Jagannath AD, Johri AM, Liberthson R, et al. Quadricuspid aortic valve: a report of 12 cases and a review of the literature. Echocardiography. 2011; 28(9): 1035-1040. doi:10.1111/j.1540- 8175.2011.01477.x.
- Borer JS, Sharma A. Drug Therapy for Heart Valve Diseases. Circulation. 2015; 132(11): 1038-1045. doi:10.1161/CIRCULATIONAHA.115.016006.
- Hayakawa M, Asai T, Kinoshita T, Suzuki T. Quadricuspid aortic valve: A report on a 10-year case series and literature review. Ann Thorac Cardiovasc Surg. 2014; 20 Suppl: 941-944. doi:10.5761/atcs.cr.13-00125.
- Aboitiz-Rivera CM, Blachman-Braun R, Lanza MF, et al. Quadricuspid aortic valve: an unexpected echocardiographic finding. Med Ultrason. 2016; 18(2): 250-252. doi:10.11152/mu.2013.2066.182.4cv.
- Song MG, Yang HS, Lee DH, Shin JK, Chee HK, et al. Mid-term results in patients having tricuspidization of the quadricuspid aortic valve. J Cardiothorac Surg. 2014; 9: 29. doi:10.1186/1749-8090-9-29.