
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 5
Uncommon occurrence of secondary plasma cell leukemia in a Sudanese female with persistent episodes of multiple myeloma
*Corresponding Author : Bashir Abdrhman Bashir
Department of Hematology, Faculty of Medical Laboratory Sciences, Port Sudan Ahlia University, Sudan.
Email: bashirbashir17@hotmail.com
Received : Sep 29, 2024
Accepted : Nov 11, 2024
Published : Nov 18, 2024
Archived : www.jcimcr.org
Copyright : © Bashir BA (2024).
Abstract
Background: Plasma Cell Leukemia (PCL) is a very aggressive lymphoproliferative disease defined by an abundance of plasma cells in the peripheral smear. It can manifest as a new occurrence or develop from Multiple Myeloma (MM), leading to the diagnosis of primary or secondary PCL, respectively.
Case presentation: We have documented a case of secondary plasma cell leukemia in a 60-year-old female patient who was diagnosed at the Dr. Awaad clinical laboratory in Sudan. The patient underwent a two-year follow-up for the etiological assessment of MM. She underwent chemotherapy following the Velcade-Thalidomide-Dexamethasone protocol and showed positive progress after completing 4 cycles. After two years, the patient exhibited symptoms of anemia and experienced persistent cough and pain in the spinal region. The laboratory analysis revealed the presence of normocytic normochromic anemia with a hemoglobin level of 4.4 g/dl and hypercalcemia with a corrected calcium level of 15.1 mg/dL. The blood smear indicated that 26% of the circulating plasma cells were present, most of which were dystrophic. This finding suggests the likelihood of secondary plasma cell leukemia.
Conclusion: Our case report focuses on an uncommon instance of MM that progressed aggressively, resulting in the formation of a plasmacytoma in the lung, followed by secondary Plasma Cell Leukemia (PCL), and ultimately spreading to the Central Nervous System (CNS). Patients with a confirmed diagnosis of multiple myeloma who have received therapy and have a stable condition should have continuous monitoring. Therefore, performing blood film examinations in all multiple myeloma patients is essential.
Keywords: Multiple myeloma; Plasma cell leukemia; Blood film examination; Paraproteinemia.
Citation: Bashir BA. Uncommon occurrence of secondary plasma cell leukemia in a Sudanese female with persistent episodes of multiple myeloma. J Clin Images Med Case Rep. 2024; 5(11): 3346.
Introduction
Plasma Cell Leukemia (PCL) is distinguished by more than 2×109/L plasma cells in the bloodstream or by a plasmacytosis that exceeds 20% of the total white blood cells [1]. The prevalence of plasma cell neoplasm is approximately 2-4%, with primary PCL accounting for most cases (60-70%). Nevertheless, secondary PCL is rising due to the improved survival rates of individuals with myeloma [1,2]. Primary PCL typically manifests at an earlier age than secondary PCL. The primary PCL and secondary PCL are separate entities; however, both have a bleak prognosis. The median overall survival for secondary PCL that occurs in the context of relapsed or refractory myeloma is between 6 to 11 months, and it is associated with worse results. The gender distribution in primary PCL and secondary PCL is roughly 3 males to every 2 females [1]. Due to the infrequency of this illness, the standards for identifying and managing it are currently being researched. This study highlights the importance of using blood smears to diagnose secondary PCL. It also presents a case report of MM advancing to secondary PCL.
Case presentation
This case report focuses on a 60-year-old hypertensive woman who was diagnosed with MM at a different medical facility. The patient exhibited reduced consciousness [Glasgow Coma Scale score of 9] and had a 22 kg/m2 body mass index. Their blood pressure was 140/80 mmHg, they were dehydrated, and they had a fever [temperature: 37.3˚C], persistent cough, and spinal pain. There was no detectable swelling of lymph nodes in the peripheral areas, no liver or spleen enlargement, and the conjunctivae and mucous membranes seemed pale without any signs of jaundice. She has received a one-year course of treatment with bortezomib, thalidomide, and dexamethasone.
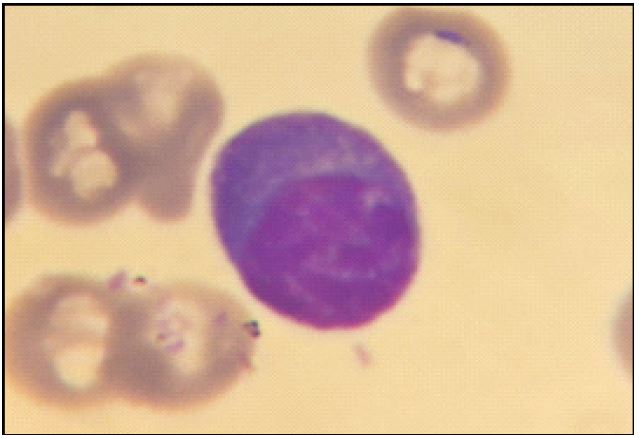
After being revived, the patient was taken to the emergency room. A biological assessment was then conducted, which involved a Complete Blood Count (CBC). The CBC displayed leukopenia [WBC:2.4x109/L], absolute lymphocytes [1.9x109/L]. Mostly plasma cells (Figure 1), absolute neutropenia [0.4x109/L], anemia [Hb:4.4 g/dL], normocytic [MCV: 100 fL], normochromic [MCHC:29.0%] blood cells, and marked thrombocytopenia [Platelet:4.0x109/L]. The biochemical evaluation revealed a corrected serum calcium level of 15.1 mg/dL, a creatinine level of 2.8 mg/dL, total proteins of 3.3 g/dL, an LDH level of 721 IU/l, and normal transaminases.
She underwent an iliac crest bone marrow at another institution due to ongoing anemia, finding an infiltration of an over 65% plasma cell predominantly dystrophic in nature. Erythropoiesis is reduced with normoblastic maturation. Granulopoiesis is also reduced across all stages of maturation, with abundant nucleated cells in the bone marrow being aberrant plasma cells. Thrombopoiesis is drastically decreased.
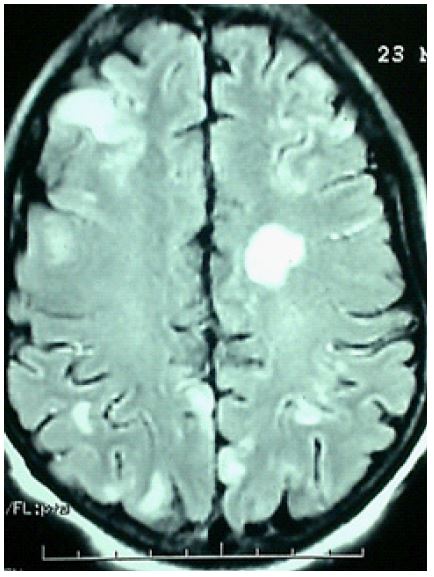
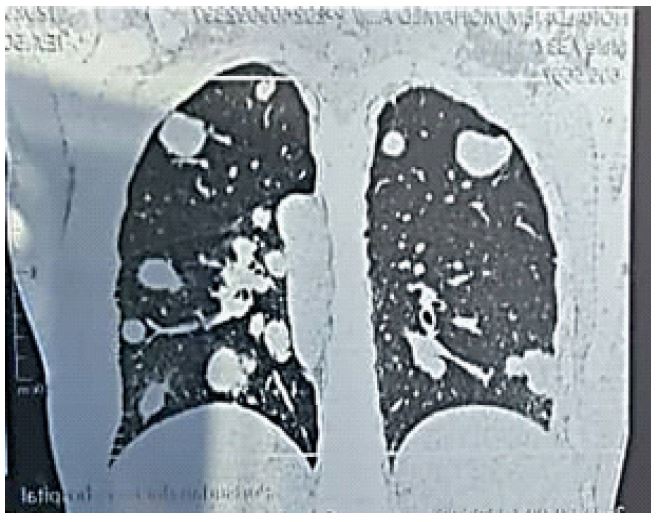
The electrophoresis of serum proteins indicated a monoclonal gammopathy. A crucial step in the diagnostic process was the detection of an IgG Kappa using Immunofixation (IF). Immunophenotyping of bone blood cells was carried out to identify the cause, which showed the following results: CD38/CD138: [73%], CD19+ [9%], CD20+ [1%], CD56+ [99%], Kappa+ [100%]. These findings suggest the presence of a Kappa CD19− plasma cell population expressing the abnormal marker CD56. The Computed tomography of the chest and brain revealed several metastatic lesions in the lung and CNS, respectively (Figures 2,3).
Discussion
The World Health Organization (WHO) defines Multiple Myeloma [MM] as having at least one or More Myeloma-Defining Events (MDEs), together with evidence of either 10% or more clonal plasma cells on bone marrow examination or a biopsy-proven plasmacytoma. MDE has consisted of well-defined criteria for CRAB characteristics, including hypercalcemia, renal failure, anemia, and bone lytic lesions, as well as additional biomarkers indicative of malignancy [3].
Plasma cell leukemia is a cancerous condition characterized by the abnormal growth of plasma cells originating from a single clone. It is considered a leukemic variant of multiple myeloma. In approximately 60% of cases, PCL is primary and secondary in the remaining 40%. The primary condition, which affects younger individuals more than MM has only been reported in older cases. Due to the infrequency of this illness, there have only been a limited number of reported cases [2]. The individual presented is a 60-year-old female, making this case of utmost importance.
While the traditional definition of PCL requires the presence of more than 2×109/L of circulatory plasma cells in peripheral blood or a relative plasmacytosis of over 20% of blood leukocytes, current research suggests that a lower threshold of circulatory plasma cells should be used to identify PCL [4-6]. Although our patient received multiple treatment cycles with the combination of bortezomib, thalidomide, daratumumab, pomalidomide, and dexamethasone for multiple myeloma, they did not successfully attain remission.
Our patient’s case is uncommon while exhibiting a tumor syndrome. The biological diagnosis relies on a comprehensive blood analysis, including a complete blood count and a blood smear stained with May Grunwald Giemsa (MGG). This staining technique enables the detection of blood plasmacytosis, indicated by a concentration of plasma cells exceeding 2 g/L or comprising more than 20% of the total leukocyte count [7]. Identifying plasma cells on blood smears can be challenging. Thus, it is crucial to apply immunophenotyping in cases where the cells are unclear to provide an accurate diagnosis. The patient’s case strongly aligns with leukopenia, characterized by a lower-than-average count of white blood cells [8].
The patient exhibited a rare combination of conditions, including leukopenia with a count of 2.4x109/L, non-regenerative normochromic normocytic anemia with a hemoglobin level below five g/dl, and deadly thrombocytopenia. These findings, while rare, are documented in medical literature, with only between 45% and 87.5% of patients exhibiting them [9]. The patient exhibited anemia characterized by a low hemoglobin level. The patient’s condition is further complicated by a hemoglobin level of 4.4 g/dL and thrombocytopenia with a count of 4.0x109/L. The myelogram or osteomedullary biopsy reveals a concerning finding of widespread infiltration of plasma cells, ranging from 65%.
The blood marrow flow cytometry analysis confirmed the existence of 65% CD138 dim-positive and kappa-restricted plasma cells, aligning with a diagnosis of secondary PCL. However, another study also revealed modest levels of CD138 expression, which can be challenging to interpret accurately [10]. During flow cytometry analysis, the CD138 molecule tends to rapidly disintegrate and vanish in the sample, potentially underestimating CD138 levels. Furthermore, the expression of CD138 can be diminished during the processing of the sample for flow cytometry. Therefore, the faint CD138 expression observed may not accurately reflect the actual biological expression of CD138 in our patient [11]. These challenges in interpreting CD138 expression highlight the complexities of the analysis and the need for further research.
Furthermore, most of these aberrant cells exhibited both cytoplasmic and surface kappa, with a subset showing positivity for CD56 and CD138 markers. This is a significant finding, as it challenges the traditional understanding of PCL and MM diagnosis. Typically, patients with these conditions have plasma cells that express a specific type of light chain clone in their cytoplasm. However, our analysis has found that plasma cells can also express this light chain clone on their surface, in addition to the cytoplasmic expression, as mentioned in previously published documents [8,11]. This discovery could have profound implications for future diagnosis and treatment strategies, underscoring the urgency and importance of our research.
These findings indicate that secondary plasma cell leukemia may have atypical morphology instead of the usual plasma cells. Therefore, it is essential to examine the peripheral smear when managing MM thoroughly. The swift advancement from Monoclonal Gammopathy of Undetermined Significance (MGUS) to plasmacytoma and, subsequently, secondary PCL, underscores the aggressive nature of MM. This necessitates a comprehensive approach to management and treatment, which takes into account the characteristics of the abnormal cells and their unique features.
Secondary PCL typically arises due to translocations involving the immunoglobulin heavy chain and other chromosomal partners (4p16, 6p21, 11q13, 16q23, and 20q11). These translocations may occur with or without concomitant mutations or deletions in chromosomes and other genes such as NRAS, KRAS, p53, MYC, and NF-kB [12]. Specifically, there is an increased occurrence of t(11; 14) (q13; q32) and other chromosomal abnormalities, including del (17p13), del (1p21), ampl (1p21), t(14; 12), and t(4:14), as documented in a previous study [13]. While the change of MM to secondary PCL is challenging to anticipate, several risk factors indicate a higher likelihood of progression. These include failure to react to initial treatment, elevated LDH levels, low serum albumin levels, hypercalcemia, advanced age, and increased plasma cells at the time of MM diagnosis [12]. Following the first diagnosis of MM, our patient underwent a comprehensive examination, revealing elevated LDH levels, abnormal serum protein analysis, and the presence of aberrant plasma cells following bone marrow biopsy.
PCL, characterized by t(11;14), exhibits an extremely unpredictable clinical course [14]. Research suggests a 50% decrease in circulating plasma cells following ten days of treatment and complete elimination of circulating plasma cells within four weeks of treatment. In addition, recent studies have demonstrated promising patient results, providing encouragement and motivation, by incorporating venetoclax, a BCL-2 inhibitor [15]. Stem cell therapy, both autologous and allogeneic, has been linked to longer periods without disease progression (progression-free survival) and longer overall survival in people with MM. However, complete remission has been observed in primary PCL patients treated with stem cell therapy, but their overall survival was lower compared to MM patients [16]. In elderly patients, particularly those with PCL, the outlook for PCL treated with traditional chemotherapy without the use of new medications is unfavorable. Therefore, it is crucial to inform and educate healthcare professionals about the importance of treating these patients with newer immunomodulatory therapies and proteasome inhibitors, which are advisable and offer the latest treatment options.
Bortezomib has an overall response rate of 69%, effectively and swiftly reduces the size of the tumor, and reverses issues related to PCL, such as renal failure and elevated blood calcium levels [17]. Lenalidomide and pomalidomide, in combination with dexamethasone and bortezomib, have been administered to treat relapse-refractory instances of MM. The treatment has shown an overall response rate of 59% [17]. In patients of advanced age who have secondary PCL and MM, induction, consolidation, and maintenance with a bortezomib-based regimen have improved the response rate and Overall Survival (OS) with or without comorbidities. While proteasome inhibitors, immunomodulatory drugs, and monoclonal antibodies have successfully improved the clinical outcome of MM, achieving complete clinical remission can still be difficult with current treatments [17]. The patient did not successfully establish remission and experienced a delay in receiving treatment with proteasome inhibitors and immunomodulatory drugs.
The patient experienced a fast advancement of MM to secondary PCL, followed by the spread of MM to the lungs and CNS. As far as we know, this particular case, an uncertain clinical course of MM, has not been documented. Due to being a 60-year-old female with other health issues, the patient did not receive a treatment plan that included proteasome inhibitors and immunomodulatory drugs. Additionally, they could not participate in clinical trials for treatment with anti-MM antibodies, Chimeric Antigen Receptor T Cell (CART) therapy, or stem cell transplantation. Our case report emphasizes the clinical setting in which the management of MM, due to its highly aggressive clinical course, poses a significant difficulty.
Conclusion
When dealing with patients who have recurring MM, particularly those who are older and have other medical conditions, it is essential to examine and manage secondary PCL carefully. The therapy protocol, combining innovative immunomodulatory drugs and monoclonal antibodies, enhanced the overall survival rate. Our case study highlights the difficulty in diagnosing, treating, and managing MM, particularly when it rapidly advances to secondary PCL.
References
- Swerdlow SH, Campo E, Harris NL, et al. World Health Organization Classification of Tumours of Haematopoietic and Lymphoid Tissues, 4th Edition. IARC Press, Lyon. 2017.
- Bougrine N, Djibrilla A, Khermach A, Mahhah M, Talmacani I, et al. De Novo Plasma-Cell Leucemia: About a Case. Saudi Journal of Pathology and Microbiology. 2017; 2: 115-117.
- Rajkumar SV. Multiple myeloma: Every year a new standard?. Hematol Oncol. 2019; 37: 62-65.10.1002/hon.2586.
- An G, Qin X, Acharya C, et al. Multiple myeloma patients with low proportion of circulating plasma cells had similar survival with primary plasma cell leukemia patients. Ann Hematol. 2015; 94: 257-264. 10.1007/s00277-014-2211-0.
- Granell M, Calvo X, Garcia-Guiñón A, et al. Prognostic impact of circulating plasma cells in patients with multiple myeloma: implications for plasma cell leukemia definition. Haematologica. 2017; 102: 1099-1104. 10.3324/haematol.2016.158303.
- Ravi P, Kumar SK, Roeker L, et al. Revised diagnostic criteria for plasma cell leukemia: Results of a Mayo Clinic study with comparison of outcomes to multiple myeloma. Blood Cancer J. 2018; 8: 116. 10.1038/s41408-018-0140-1.
- International Myeloma Working Group. Criteria for the Classification of Monoclonal Gammapathies, Multiple Myeloma and Related Disorders: A Report of the International Myeloma Working Group. British Journal of Haematology. 2003; 121: 749-757. https://doi.org/10.1046/j.1365-2141.2003.04355.x.
- Pasqualetti P, Festuccia V, Collacciani A, Acitelli P, Casale R. Plasma-Cell Leukemia. A Report on 11 Patients and Review of the Literature. Panminerva Medica. 1996; 38: 179-1.
- Guieze R, Moreau AS, Dupire S, Coiteux V, Facon T, et al. Leucemie a plasmocytes. Hematologie. 2005; 115: 217-225.
- Sanchez L, Wang Y, Siegel DS, Wang ML. Daratumumab: A first-in-class CD38 monoclonal antibody for the treatment of multiple myeloma. J Hematol Oncol. 2016; 9: 51. 10.1186/s13045-016-0283-0.
- Kumar S, Kimlinger T, Morice W. Immunophenotyping in multiple myeloma and related plasma cell disorders. Best Pract Res Clin Haematol. 2010; 23: 433-451. 10.1016/j.beha.2010.09.002.
- Van de Donk NW, Lokhorst HM, Anderson KC, Richardson PG. How I treat plasma cell leukemia. Blood. 2012; 120: 2376-2389. 10.1182/blood-2012-05-408682.
- Gundesen MT, Lund T, Moeller HEH, Abildgaard N. Plasma cell leukemia: definition, presentation, and treatment. Curr Oncol Rep. 2019; 21: 8. 10.1007/s11912-019-0754-x.
- An G, Xu Y, Shi L, et al. t(11;14) multiple myeloma: A subtype associated with distinct immunological features, immunophenotypic characteristics but divergent outcome. Leuk Res. 2013; 37: 1251-1257.10.1016/j.leukres.2013.06.020.
- Durie BG, Goldschmidt H, Mateos MV, et al. Outcomes of patients with t(11;14) multiple myeloma: an International Myeloma Working Group (IMWG) multicenter study. J Clin Oncol. 2019; 37: 8015-8015.
- Drake MB, Iacobelli S, Van Biezen A, et al. Primary plasma cell leukemia and autologous stem cell transplantation. Haematologica. 2010; 95: 804-809. 10.3324/haematol.2009.013334.
- Katodritou E, Terpos E, Kelaidi C, et al. Treatment with bortezomib-based regimens improves overall response and predicts for survival in patients with primary or secondary plasma cell leukemia: Analysis of the Greek myeloma study group. Am J Hematol. 2014; 89: 145-150. 10.1002/ajh.23600.