
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Clinical Image - Open Access, Volume 5
Cavernous sinus syndrome secondary to pituitary apoplexy
Kyle Wong1*; Daniel Brungs2
1Medical Oncology Registrar, Wollongong Hospital, New South Wales, Australia.
2Medical Oncologist, Wollongong Hospital, New South Wales, Australia. Graduate School of Medicine, University of Wollongong, Australia.
*Corresponding Author : Kyle Wong
Medical Oncology Registrar, Wollongong Hospital, New South Wales, Australia.
Email: kyle_wong@live.com
Received : Oct 24, 2024
Accepted : Nov 12, 2024
Published : Nov 19, 2024
Archived : www.jcimcr.org
Copyright : © Wong K (2024).
Citation: Wong K, Brungs D. Cavernous sinus syndrome secondary to pituitary apoplexy. J Clin Images Med Case Rep. 2024; 5(11): 3348.
Description
A 64-year old woman with metastatic gastric adenocarcinoma and recurrent pituitary macroadenoma presented with a one day history of headache and vomiting. She was diagnosed with small pulmonary emboli one week prior and was treated with therapeutic enoxaparin at 1 mg/kg BD.
On exam she had a left sided ptosis of the eyelid, inability to move her left eye in all four directions and reduced sensation overlying her left forehead. She had diplopia on horizontal and vertical gaze testing. This was consistent with an oculomotor (III), trochlear (IV), ophthalmic branch of the trigeminal (V1) and abducens (VI) nerve palsy.
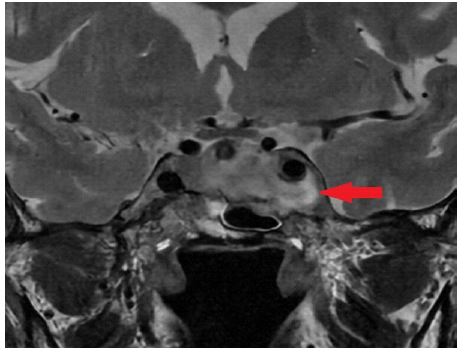
Magnetic resonance imaging scan of the head demonstrated a large sellar and parasellar mass lesion with signal intensity consistent with subacute haemorrhage peripherally and acute haemorrhage centrally (red arrow). A diagnosis of cavernous sinus syndrome secondary to pituitary apoplexy was made.
Cavernous sinus syndrome is characterised by ophthalmoplegia, Horner’s syndrome and sensory loss of the trigeminal nerve [1]. There are numerous aetiologies including infectious, inflammatory, vascular and neoplastic [1,2]. Pituitary apoplexy describes pituitary cellular destruction secondary to haemorrhage or ischemia occurring within the normal pituitary gland or into a pituitary adenoma [3]. It can present with a range of symptoms including headache, visual dysfunction and acute adrenal insufficiency with hypotension and shock [3]. Management of pituitary apoplexy includes stress dosing of hydrocortisone, management of pituitary hormone excess or deficiency and in some cases, resection of the pituitary gland [4].
Given our patient’s advanced cancer she was managed conservatively without neurosurgical intervention. She was commenced on thyroxine and stress steroids for her hypopituitarism. Balancing the risks of her pituitary haemorrhage and treatment of her pulmonary emboli, her enoxaparin dose was reduced to 40 mg daily.

References
- Lee JH, Lee HK, Park JK, Choi CG, Suh DC. Cavernous sinus syndrome: Clinical features and differential diagnosis with MR imaging. AJR Am J Roentgenol. 2003; 181(2): 583-590. doi:10.2214/ajr.181.2.1810583.
- Nassrallah G, Sun V, Guiot MC, Mikhail M, Arthurs B. Cavernous sinus syndrome associated with metastatic colorectal cancer and perineural spread along the trigeminal nerve. Am J Ophthalmol Case Rep. 2017; 6: 67-70. doi:10.1016/j.ajoc.2016.11.011.
- Jamal Y, Camacho Y, Hanft S, Chiarolanzio P, Goldberg MD, et al. A Case of Pituitary Apoplexy and Cavernous Sinus Syndrome during Hemodialysis. Case Rep Endocrinol. 2023; 2023: 3183088. Published 2023 Apr 25. doi:10.1155/2023/3183088.
- Barkhoudarian G, Kelly DF. Pituitary Apoplexy. Neurosurg Clin N Am. 2019; 30(4): 457-463. doi:10.1016/j.nec.2019.06.001.