
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 5
Acute liver injury and pulmonary embolism secondary to nitrous oxide inhalation: A case report
Prayag Jariwala; Harshit Gupta; Mahyar Toofantabrizi*
Department of Internal Medicine, MedStar Franklin Square Medical Center, 9000 Franklin Square Drive, Baltimore, MD, USA.
*Corresponding Author : Mahyar Toofantabrizi
Department of Internal Medicine, MedStar Franklin Square Medical Center, 9000 Franklin Square Drive, Baltimore, MD, USA.
Email: mahyar.toofantabrizi@medstar.net
Received : Oct 27, 2024
Accepted : Nov 13, 2024
Published : Nov 20, 2024
Archived : www.jcimcr.org
Copyright : © Toofantabrizi M (2024).
Abstract
Nitrous oxide is an inhalational anesthetic with a high abuse potential. Its increased abuse in recent times has been associated with adverse effects of myeloneuropathy, venous thrombosis, myocardial infarction, and pneumothorax. We report a case of a 36-year-old male who presented with acute onset chest pain following inhalation of nitrous oxide. Upon admission, the patient had sinus tachycardia and icterus on physical examination. Labs revealed findings suggestive of acute liver injury, and diagnostic imaging revealed bilateral segmental lower lobe pulmonary emboli and pneumomediastinum. A final diagnosis of acute liver injury and pulmonary embolism secondary to nitrous oxide abuse was made after ruling out other possible causes, including ischemic, viral, and other hepatic toxins. The patient was started on intravenous heparin, fluids, and empirical N-acetyl cysteine with a remarkable improvement. This case highlights the risk for acute liver injury associated with nitrous oxide abuse.
Keywords: Nitrous oxide; Venous thrombosis; Acute liver injury; Pulmonary emboli; Pneumomediastinum.
Citation: Jariwala P, Gupta H, Toofantabrizi M. Acute liver injury and pulmonary embolism secondary to nitrous oxide inhalation: A case report. J Clin Images Med Case Rep. 2024; 5(11): 3350.
Introduction
Nitrous oxide is a colorless, odorless anesthetic that can produce a euphoric state [1]. It is a low-potency anesthetic with no significant effect on hemodynamics or respiration. In recent years, nitrous oxide has become a recreational drug among young adults [2]. Its euphoric and psychedelic effects, along with its easy availability in the form of cartridges, have increased its potential for abuse [3,4]. Severe adverse effects associated with long-term abuse include megaloblastic anemia, myeloneuropathy, and venous thrombosis, which can be detrimental [5]. Additionally, literature reports suggest a predisposition for pneumothorax, pneumopericardium, pneumomediastinum, and seizure associated with nitrous oxide abuse [4]. This case study presents acute liver injury and pulmonary embolism secondary to nitrous oxide abuse.
Case history/examination
A 36-year-old male presented to the emergency department with acute onset chest pain following inhalation of nitrous oxide. The chest pain was just associated with palpitations and worsened with deep breaths. The patient had a history of marijuana abuse but denied long-term alcohol use, though he reported consuming more than a fifth of a pint of alcohol per day over the past few days due to work-related stress. He also did not report any recent travel, surgery or history of cancer. Upon admission, his vitals were within normal range except for sinus tachycardia. Physical examination was unremarkable except for icterus.
Differential diagnosis and investigation
Complete blood count revealed a slightly elevated white blood cell count of 12.63 k/uL and severe thrombocytopenia of 40 k/uL with a high immature platelet fraction of 12.4%, suggesting possible peripheral platelet destruction or bone marrow recovery. The basic metabolic profile demonstrated highly elevated levels of Aspartate Aminotransferase (AST) and Alanine Aminotransferase (ALT), as well as a high total bilirubin of 5.3 mg/dL and direct bilirubin of 3.35 mg/dL (Table 1). Further testing confirmed acute liver failure, with an International Normalized Ratio (INR) of 3.5 and Prothrombin Time (PT) of 34.5 seconds. Urinalysis was positive for bilirubin, and urine toxicology for cannabinoids. Lactic acid was mildly elevated at 3 mmol/L. Serial troponin levels were negative.
Imaging studies were conducted to investigate the patient’s presentation. The chest X-ray showed mildly prominent interstitial markings. Due to the ongoing chest pain and laboratory findings indicating acute liver failure, a Computed Tomography (CT) scan of the chest, abdomen, and pelvis was performed. This revealed acute bilateral segmental lower lobe pulmonary emboli and pneumomediastinum, but no significant intra-abdominal pathology. The patient was found to be functional and mobile, with no recent history of travel, surgery, or cancer. However, the underlying cause of the pulmonary findings remained unclear and may be related to the risk of thromboembolism caused by nitrous oxide abuse.
Echocardiography showed mild concentric left ventricular hypertrophy without evidence of right heart strain. Further evaluation with duplex ultrasound of the liver excluded portal or hepatic vein thrombosis. Additional testing was conducted to determine the etiology of the patient’s acute liver failure. The viral hepatitis panel was negative, and alcohol and acetaminophen levels were undetectable. Titers for autoimmune pathology and catastrophic antiphospholipid antibody syndrome testing were also negative. The workup for genetic causes, such as hemochromatosis or Wilson’s disease, was unremarkable.
Treatment
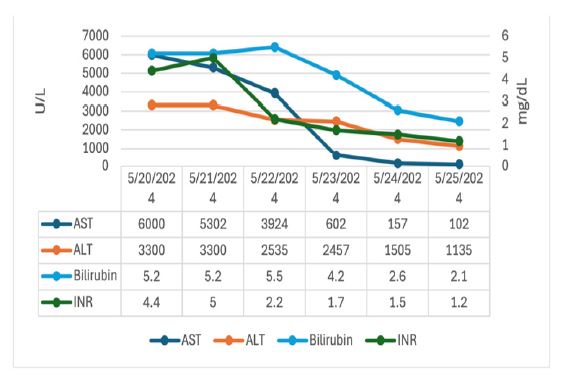
The patient was started on intravenous heparin, fluids, and empirical N-acetyl cysteine. By the second day of admission, the patient reported improved chest pain and yellowish skin discoloration. Lab results revealed a downtrend in bilirubin, lactate, AST, and ALT levels (Figure 1). The patient was successfully discharged with a transition to oral anticoagulants and was counseled to avoid nitrous oxide and alcohol abuse to prevent further liver injury.
Upon follow-up, the patient reported continued improvement in chest pain and jaundice. Laboratory tests revealed liver function levels nearing baseline. A final diagnosis of acute liver injury and pulmonary embolism secondary to nitrous oxide abuse was made after ruling out other possible causes, including ischemic, viral, and other hepatic toxins.
Table 1: Results of complete blood count, liver function test, and renal function test.
| Investigations | Reference range,adults(this hospital) | At admission | At discharge |
|---|---|---|---|
| Hemoglobin (g/dL) | 12.5-16.5 | 14.4 | 11.5 |
| Whitecellcount(per uL) | 4,000-10,800 | 12,630 | 6,880 |
| Differential count (per uL) | |||
| Neutrophils (%) | 43.0-75.0 | 91.5 | 43.4 |
| Lymphocytes (%) | 15.0-45.0 | 5.2 | 36.2 |
| Monocytes (%) | 3.0-12.0 | 2.5 | 13.1 |
| Platelets(peruL) | 145000-400000 | 40,000 | 102 |
| Immatureplatelet (%) | 1.1-6.7 | 12.4 | 8.3 |
| Liverfunction test | |||
| Aspartate aminotransferase(U/L) | 0-33 | >6000 | 102 |
| Alanine aminotransferase(U/L) | 10-49 | >3300 | 1135 |
| Total bilirubin(mg/dL) | 0.3-1.2 | 5.2 | 2.1 |
| Directbilirubin (mg/dL) | 0.0-0.3 | 3.35 | |
| Alkalinephosphatase (U/L) | 46-116 | 161 | 189 |
| Prothrombintime (sec) | 12.2-14.8 | 34.5 | 15.9 |
| International normalized ratio,INR | 0.8-1.2 | 3.5 | 1.2 |
| Albumin | 3.2-4.8 | 4.0 | 3.0 |
| Renal function test | |||
| Sodium(mmol/L) | 137-145 | 132 | 141 |
| Potassium (mmol/L) | 3.5-5.1 | 4.1 | 3.8 |
| Bloodurea (mg/dL) | 9-20 | 23 | 6 |
| Creatinine (mg/dL) | 0.66-1.50 | 0.60 | 0.38 |
Discussion
Nitrous oxide, also known as laughing gas, has anesthetic properties along with analgesic and anxiolytic effects [2]. Studies have also reported its therapeutic effect in treatment-resistant depression, with a prompt onset of action in decompensated patients [6]. However, these potential therapeutic effects are associated with a risk of drug abuse and long-term side effects, such as myeloneuropathy and venous thrombosis [5]. Previous studies have indicated risks for bowel distension, arrhythmia, myocardial infarction, seizure, pneumothorax, and pneumomediastinum with nitrous oxide use [7-10]. A case report has also documented acute liver injury secondary to nitrous oxide use [11].
In this study, the patient presented with acute onset chest pain associated with tachycardia following the inhalation of high-dose nitrous oxide. Investigations revealed acute bilateral segmental lower lobe pulmonary emboli along with acute liver injury. The patient was started on anticoagulants for pulmonary embolism and managed with fluids and N-acetylcysteine for acute liver injury. A diagnosis of exclusion of acute liver injury and pulmonary embolism secondary to inhalation of high-dose nitrous oxide was made after ruling out other causes.
Nitrous oxide has been shown to inhibit methionine synthase, leading to increased homocysteine levels [9]. Elevated homocysteine can cause endothelial dysfunction, dysfibrinogenemia, increased platelet and coagulation activation, thereby increasing the risk of thrombosis seen with nitrous oxide use. Acute liver injury could be due to hypoxia associated with the acute inhalation of high-dose nitrous oxide.
Conclusion
In conclusion, Nitrous oxide offers anesthetic, analgesic, anxiolytic, and antidepressant properties. However, its potential for abuse, along with side effects such as myeloneuropathy, venous thrombosis, myocardial infarction, pneumothorax, and acute liver injury, could be detrimental. This case highlights that the easy availability and increased abuse of nitrous oxide may lead to more emergency visits and in-hospital morbidity due to the acute adverse events associated with its use.
References
- Knuf K, Maani CV. Nitrous Oxide. In: StatPearls. StatPearls Publishing. 2024.http://www.ncbi.nlm.nih.gov/books/NBK532922/.
- Xiang Y, Li L, Ma X, et al. Recreational Nitrous Oxide Abuse: Prevalence, Neurotoxicity, and Treatment. Neurotox Res. 2021; 39(3): 975-985. doi:10.1007/s12640-021-00352-y.
- Ziegenfuß T, Zander R. Nitrous oxide as a party drug. Anaesthesiol. 2024; 25. doi:10.1007/s00101-024-01427-z
- Davidson LT. Recreational use of nitrous oxide causes seizure, pneumothorax, pneumomediastinum, and pneumopericardium: nitrous oxide and its harm, a case report. Ups J Med Sci. 2023; 128. doi:10.48101/ujms.v128.10281.
- Kronenberg G, Schoretsanitis G, Seifritz E, Olbrich S. The boon and bane of nitrous oxide. Eur Arch Psychiatry Clin Neurosci. 2024; 13. doi:10.1007/s00406-024-01801-3.
- Rech P, Custodio RM, Rodrigues Uggioni ML, et al. Use of nitrous oxide in the treatment of major depressive disorder and treatment-resistant major depressive disorder: A systematic review and meta-analysis nitrous oxide in depressive disorders. Prog Neuropsychopharmacol Biol Psychiatry. 2024; 129: 110869. doi:10.1016/j.pnpbp.2023.110869.
- Myles PS, Leslie K, Silbert B, Paech MJ, Peyton P. A Review of the Risks and Benefits of Nitrous Oxide in Current Anaesthetic Practice. Anaesth Intensive Care. 2004; 32(2): 165-172. doi:10.1177/0310057X0403200202.
- AkÇa O, Lenhardt R, Fleischmann E, et al. Nitrous oxide increases the incidence of bowel distension in patients undergoing elective colon resection. Acta Anaesthesiol Scand. 2004; 48(7): 894-898. doi:10.1111/j.0001-5172.2004.00427.x.
- Oomens T, Riezebos RK, Amoroso G, Kuipers RS. Case report of an acute myocardial infarction after high-dose recreational nitrous oxide use: a consequence of hyperhomocysteinaemia? Eur Heart J - Case Rep. 2021; 5(2): ytaa557. doi:10.1093/ehjcr/ytaa557.
- McDermott R, Tsang K, Hamilton N, Belton M. Recreational nitrous oxide inhalation as a rare cause of spontaneous pneumomediastinum. BMJ Case Rep. 2015; 2015: bcr2015209750. doi:10.1136/bcr-2015-209750.
- Gullestrup A, Jensen RB, Bøgevig S, Nilsson PM. Acute neuropathy and liver injury following the abuse of nitrous oxide. Ugeskr Laeger. 2019; 181(20): V12180890.