
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Clinical Image - Open Access, Volume 5
Rapid evolution of delayed pericardial tamponade following cardiac surgery: Clinical image
Ryan Lee1*; Mohamed Tiouririne2
1Departments of Anesthesiology and Emergency Medicine, Division of Anesthesia Critical Care, University of Virginia Health, Charlottesville, Virginia, 22903, USA.
2Departments of Anesthesiology and Obstetrics & Gynecology, Division of Anesthesia Critical Care, University of Virginia Health, Charlottesville, Virginia, 22903, USA.
*Corresponding Author : Ryan Lee
Departments of Anesthesiology & Emergency Medicine, Division of Anesthesia Critical Care, University of Virginia Health, Charlottesville, VA 22903, USA.
Email: ryan.lee@uvahealth.org
Received : Oct 28, 2024
Accepted : Nov 14, 2024
Published : Nov 21, 2024
Archived : www.jcimcr.org
Copyright : © Lee R (2024).
Abstract
Delayed pericardial tamponade represents a rare but life-threatening complication following cardiac surgery. We present a case of a 67-year-old male who developed delayed pericardial tamponade on postoperative day 8 following a Bio-Bentall procedure with diagnosis confirmed via bedside transthoracic echo facilitating expeditious operative intervention and safe hospital discharge.
Keywords: Pericardial effusion; Pericardial tamponade; Cardiac surgery; Transthoracic echocardiography.
Citation: Lee R, Tiouririne M. Rapid evolution of delayed pericardial tamponade following cardiac surgery: Clinical image. J Clin Images Med Case Rep. 2024; 5(11): 3352.
Description
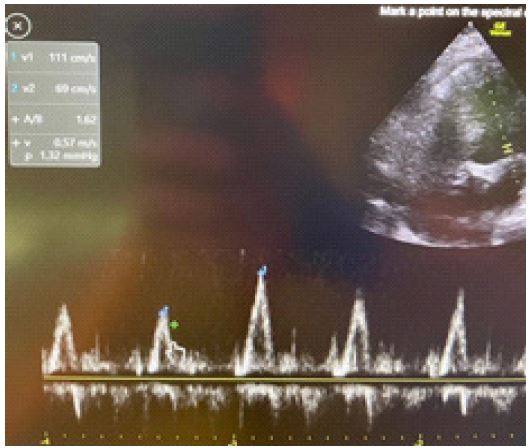
After an initially routine postoperative course, a 67-year-old male developed progressive tachypnea, tachycardia, and hypotension with a narrow pulse pressure on POD 8 following a Bio-Bentall procedure. Initial bedside Transthoracic Echocardiography (TTE) revealed a moderate sized pericardial effusion (Figure 1) which on repeat examination 5 hours later had progressed to tamponade physiology (Figures 2,3). The patient was taken for urgent surgical evacuation with fluid analysis consistent with an inflammatory but non-infectious pericarditis. Following drainage, the patient was treated with colchicine and ultimately discharged to acute rehabilitation on hospital day 24.
While usually small, asymptomatic, and clinically insignificant, Postoperative Pericardial Effusions (PPE) are common following cardiac surgery. Delayed effusions occurring after postoperative day 7 resulting in Pericardial Tamponade (PT) are an uncommon and life-threatening complication. A recent retrospective study reported an overall incidence of late postoperative PT of 6.2% with the highest rate following aortic surgery (9.3%; inclusive of concomitant coronary and/or valve procedures as in the presented case), followed by single valve procedures (6.6%), with isolated CABG having the lowest incidence (1.3%) [1]. This complication can result in both increased morbidity and mortality, as well as hospital and ICU length of stay, particularly when there is a delay to diagnosis. PT should be clinically suspected when a patient develops tachypnea, dyspnea, tachycardia and/or hypotension, particularly when associated with a narrow pulse pressure. Bedside echocardiography, a tool readily available to intensive care and emergency physicians, has been proven to expedite the diagnosis and time-to-treatment of this life-threatening complication [1]. Diagnostic features include right atrial systolic collapse, right ventricular diastolic collapse (Figure 2), IVC collapsibility < 50% upon inspiration, and respiratory flow variation across the mitral valve (Figure 3) of >25%. Therapeutic options include both interventional and surgical drainage, with subsequent medical management consisting of colchicine, high dose aspirin, NSAIDs, and corticosteroids for recurrent cases [2].


References
- Alerhand S, Carter J M. What echocardiographic findings suggest a pericardial effusion is causing tamponade?. The American journal of emergency medicine. 2019; 37(2): 321-326. https://doi.org/10.1016/j.ajem.2018.11.004.