
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 5
Irvan syndrome: A case report and literature review
Alassane BA*1; Aïssatou AW1; Sy El Hadji Malick1; Diallo Hawo Madina1; Ka Aly Mbara1; Mbaye Soda1; Diagne Jean Pierre1; Senghor Ousmane Ndiaga1; Gaye Serigne Souhaibou1; Ndiaye Mouhamed1; Ndiaye Lamine1; Ndoye Paule Aida2; Ndiaye Papa Amadou1
1Abass NDAO Hospital, Dakar, Senegal.
2Aristide Le Dantec Hospital, Dakar, Senegal.
*Corresponding Author : Alassane BA
Abass NDAO Hospital, Dakar, Senegal.
Email: assaneba2008@live.fr
Received : Nov 01, 2024
Accepted : Nov 18, 2024
Published : Nov 25, 2024
Archived : www.jcimcr.org
Copyright : © Alassane BA (2024).
Abstract
Purpose: Idiopathic Retinal Vasculitis, Aneurysms, and Neuroretinitis syndrome (IRVAN) is a rare disorder of unknown etiology. It is most commonly characterized by bilateral involvement with arterial bifurcation aneurysms, arterial vasculitis, exudative maculopathy, neuroretinitis, and peripheral retinal ischemia. The aim of this case report and a review of the literature is to highlight the clinical and therapeutic features of this syndrome.
Case report: We report the case of a 28-year-old patient with IRVAN syndrome. Clinical and angiofluographic semiology were characteristic. She was treated by retinal photocoagulation in peripheral non perfusion areas and subsequent intravitreal injections of bevacizumab.
Conclusion: syndrome is a rare but important condition to be aware of. Retinal photocoagulation is the first-line treatment.
Keywords: Irvan; Fluorescence angiography; Optical coherence tomography; Retinal photocoagulation; Bevacizumab.
Abbreviations: IRVAN: Idiopathic Retinal Vasculitis Aneurysms and Neuroretinitis; VEGF: Vascular Endothelial Growth Factor; OCT: Optical Coherence Tomography; IVT: Intravitreal Injection; NVG: Neovascular glaucoma.
Citation: Alassane BA, Aïssatou AW, Malick SEH, Madina DH, Mbara KA, et al. Irvan syndrome: A case report and literature review. J Clin Images Med Case Rep. 2024; 5(11): 3355.
Introduction
Idiopathic, Retinal Vasculitis, Aneurysms, and Neuroretinitis syndrome (IRVAN) is a rare disorder first described in 1995. It is a vasculitis that most often affects young women [1]. Involvement is often bilateral but unilateral case have been reported [2]. The diagnosis is based on major and minor criteria [3]. Prognosis may be severe with rapid vision loss due to retinal ischemia or macular exudation. Retinal photocoagulation is the first-line treatment which can be combined with anti-VEGF injection or adjuvanted corticosteroids [3]. We report a case of IRVAN syndrome treated with retinal photocoagulation and anti-VEGF intravitreal injections.
Case report
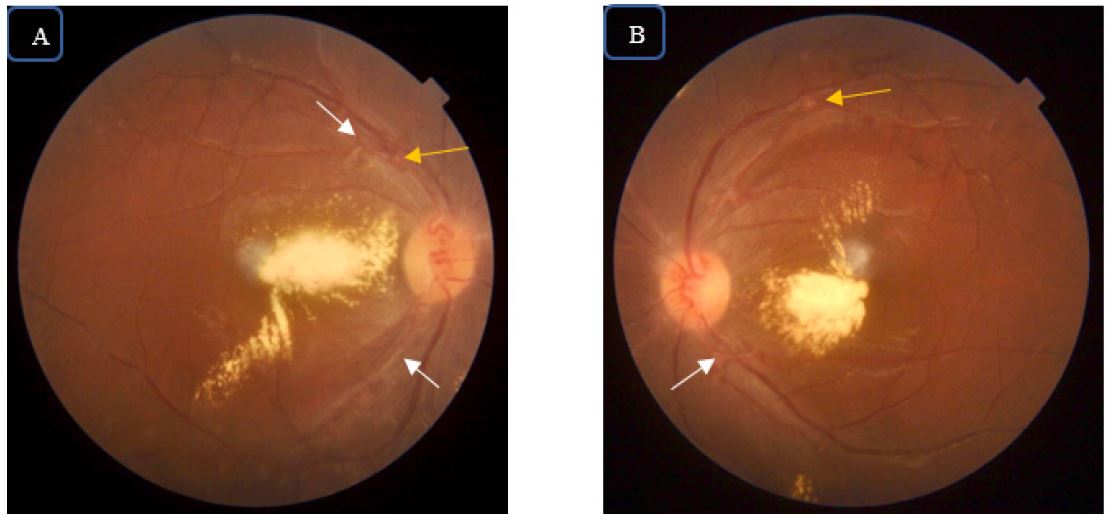
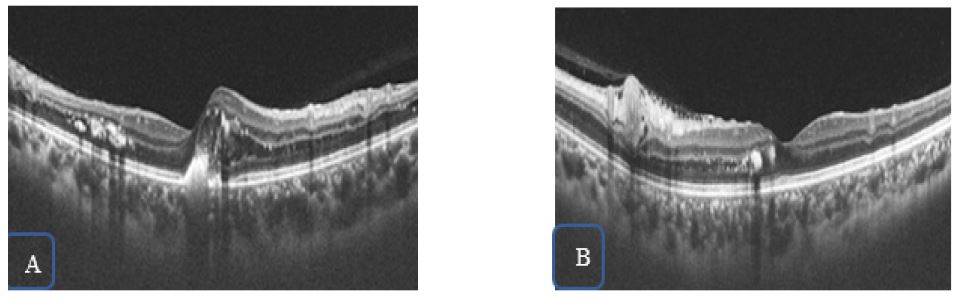
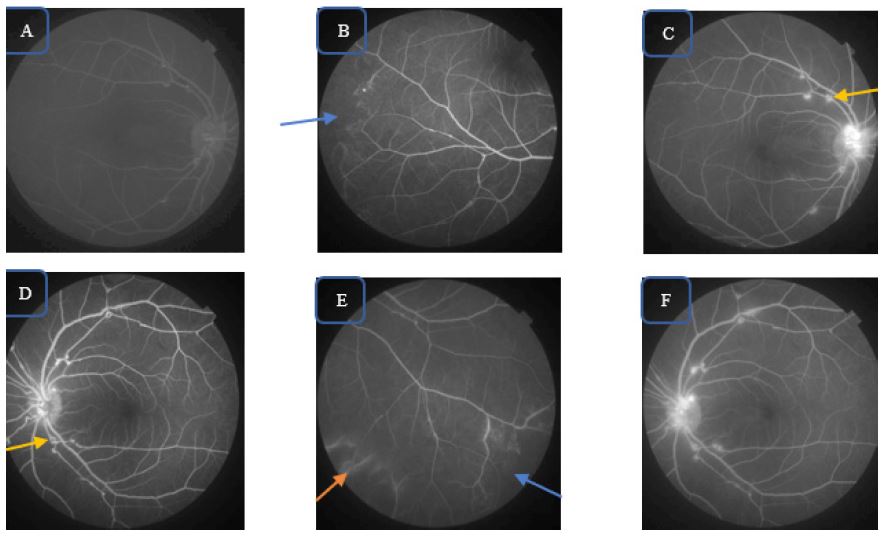
A 28-year-old melanoderm women, complained about vision loss with myodesopsias in the right eye over the past year. Her visual acuity was 20/40 in the right eye and 20/20 in the left eye. The anterior segment was normal and the intraocular pressure was 13 mmHg in both eyes. The fundus examination showed in both eyes: tortuosity of the peripapillary vessels, vasculitis with narrowed and sheathed arteries, aneurysms at the arterial bifurcations with nasal and peripapillary and macular exudation (Figure 1). In the right eye, Optical Coherence Tomography (OCT) showed retro-foveolar thickening with hyper-reflective dots in the retinal inner layers and epiretinal membrane. In the left eye, para-foveolar thickening, epiretinal membrane with juxta-foveolar hyper-reflective dots was noted (Figure 2). Fluo rescence angiography showed multiple macroaneurysms at ar terial bifurcation sites, capillary non-perfusion areas and subtle papillary and para-macular diffusion at the late stage (Figure 3).
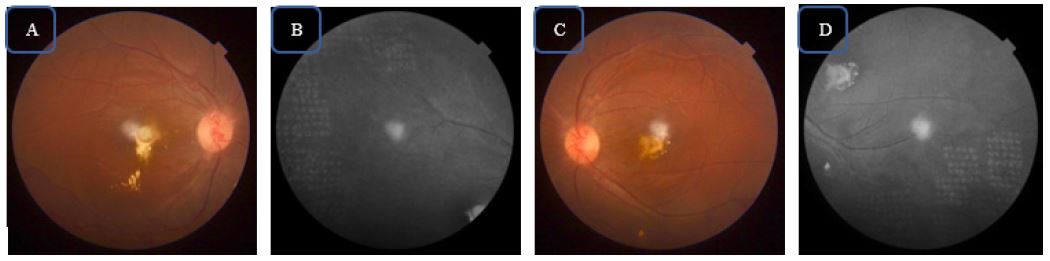
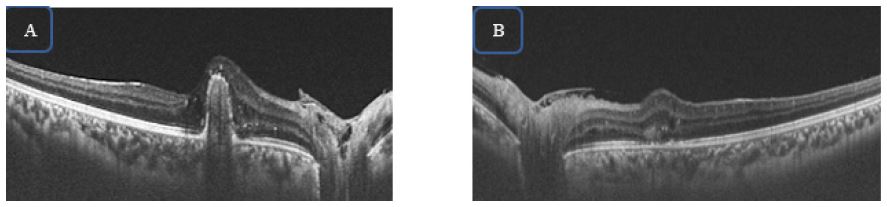
The cardiovascular evaluation was normal. IRVAN syndrome was the most likely diagnosis in this case. A photocoagulation of the ischemia areas was performed on both eyes, and she had three Intravitreal injections (IVT) of bevacizumab for the macula exudation. After one year of follow-up, the visual acuity was 20/40 in the right eye and 20/32 in the left eye. The fun dus showed in both eyes a persistence of arterial aneurysms, a regression of retinal exudation and a juxta-foveal scar fibrosis (Figure 4). OCT control showed a juxta-foveal dome uplift of the Pigment Epithelium (PE) more visible on the right eye with a preservation of the systematization of the outer retinal layers (Figure 5).
Discussion
IRVAN syndrome is a condition of the young adult and female predominance has been reported in the majority of series [1,3]. Involvment is most often bilateral [3-5], but unilateral case has been described by Mossavi [2]. The diagnosis is based on crite ria including three major (aneurysmal dilations in arterial bifur cations, retinal vasculitis and neuroretinitis) and three minors (retinal ischemia, exudative maculopathy and retinal neovascu larization) [1]. In our patient, the clinical and angiofluographic presentation was typical and included all major criteria and 2 minor criteria. Aneurysms located in the arterial branches of the head of the optic nerve or first-order arteries, are the most characteristic signs of this syndrome. However, exudative mac ulopathy and peripheral retinal ischemia are most described [1,6]. Retinal vasculitis and neuroretinitis were described in all patients in the Chang series [1].
Samuel proposed a prognostic and therapeutic classifica tion in 5 stages [3]. Our patient was classified stage 2. Exuda tive maculopathy and retinal ischemia, responsible of visual loss, are poor factors prognosis [3]. IRVAN syndrome is an id iopathic pathology, however an inflammatory component has been described in its pathophysiology [7]. An association with p-ANCA vasculitis and anti-phospholipid antibody syndrome was described [8-10]. It is important to differentiate this con dition with other pathologies such as macroaneurysms of high blood pressure, Coats’ disease and Eales’ disease [7]. In adult Coats’ disease, saccular dilations are both arterial and venous. Eales’ disease, which primarily affects the peripheral retina, is not associated with arterial aneurysms or vascular tortuosity [7]. Photocoagulation of ischemic areas performed in our pa tient, is the first line treatment admitted in the literature allow ing prevention of neovascularization [3]. Contrary to our case, photocoagulation allowed macular edema regression in Man sour’s IRVAN syndrome case reported [6]. Anti-VEGF is a thera peutic alternative and is thus indicated in case of neovascular complications [11,12]. Our patient had 3 injections of bevaci zumab with a regression of macular edema. Using systemic or intravitreal of corticosteroids is discussed. Saatci [4] reported a case successfully treated with a dexamethasone implant but ac cording to Lemaitre [13] their efficiency would be short.
After 12 months follow-up, our patient presented a bilateral macular scar fibrosis with near-acuity conservation, justified by the integrity of the outer retinal layers. Indeed, this compli cation was also reported by Nabil in 16.7% [5]. The prognosis for our patient is unpredictable, but according to Samuel early treatment with photocoagulation helps maintain good vision and prevent neovascularization [3].
Conclusion
RVAN syndrome is a rare idiopathic entity, mainly affecting young women. The search for an associated systemic disease is appropriate. Visual prognosis depends on ischemic involvement and exudative maculopathy. Photocoagulation is the reference treatment, supplemented by anti-VEGF.
References
- Chang TS, Aylward GW, Davis JL, et al. Idiopathic Retinal Vas culitis, Aneurysms, and Neuro-retinitis. Ophthalmology. 1995; 102(7): 1089-1097.
- Moosavi M, Hosseini SM, Shoeibi N, et al. Unilateral idiopathic retinal vasculitis, aneurysms, and neuroretinitis syndrome (IR VAN) in a young female. J Curr Ophthalmol. 2015; 27(1): 63-66.
- Samuel MA, Equi RA, Chang TS, et al. Idiopathic Retinitis, Vascu litis, Aneurysms, and Neuroretinitis (IRVAN): New Observations and a Proposed Staging System. Ophthalmology. 2007; 114(8): 1526-152 9.e1.
- Saatci AO, Ayhan Z, Takeş Ö, et al. Single Bilateral Dexametha sone Implant in Addition to Panretinal Photocoagulation and Oral Azathioprine Treatment in IRVAN Syndrome. Case Rep Oph thalmol. 2015; 6(1): 56-62.
- Nabi W, Khochtali S, Ben Amor H, et al. IRVAN syndrome: A ret rospective review of 9 cases from Tunisia. J Fr Ophtalmol. 2022; 45 :1012-1020.
- Mansour M, Al-Ghotani B, Abo-Shdeed B, et al. IRVAN syndrome: A case report and a literature review. Ann Med Surg. 2022; 77: 103725.
- Bajgai P, Katoch D, Dogra MR, et al. Idiopathic retinal vasculitis, aneurysms, and neuroretinitis (IRVAN) syndrome: clinical per spectives. Clin Ophtalmol. 2017; 11: 1805-1817.
- Nourinia R, Montahai T, Amoohashemi N, et al. Idiopathic Reti nal Vasculitis, Aneurysms and Neuroretinitis Syndrome Associ ated with Positive Perinuclear Antineutrophil Cytoplasmic Anti body. J Ophthalmic Vis Res. 2011; 6(4): 330-333.
- Alaerts N, Fortunati M. Syndrome d’IRVAN: à propos d’un cas. J Fr Ophtalmol. 2021; 44(4): e223-226.
- Kurz DE, Wang RC, Kurz PA. Idiopathic Retinal Vasculitis, Aneu rysms, and Neuroretinitis in a Patient with Antiphospholipid Syndrome. Arch Ophthalmol. 2012; 130(2): 257-258.
- Akesbi J, Brousseaud FX, Adam R, et al. Intravitreal bevacizumab (Avastin®) in idiopathic retinitis, vasculitis, aneurysms and neu roretinitis. Acta Ophthalmol (Copenh). 2010; 88(2): e40-41.
- Dupas B. Occlusive vasculitis not to be ignored: IRVAN syn drome. Images en Ophtalmologie. 2018; 12(2): 58-61.
- Lemaitre C, Ducos de Lahitte G, et al. Imaging study and popula tion predisposition in IRVAN syndrome: about 4 cases. J Fr Oph talmol. 2007; 30: 2S228.