
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Series - Open Access, Volume 5
Salmonella meningitis: Five cases
Kaouani D*; Elfakiri K; Rada R; Draiss G; Bouskraoui M
Pediatrics Department A, Pneumopaediatric Unit, Mohammed VI University Hospital, Cadi Ayyad University, Morocco.
*Corresponding Author : Douaa Kaouani
Pediatrics Department A, Pneumopaediatric Unit, Mohammed VI University Hospital, Cadi Ayyad University, Morocco.
Email: douaakaouani92@gmail.com
Received : Oct 29, 2024
Accepted : Nov 20, 2024
Published : Nov 27, 2024
Archived : www.jcimcr.org
Copyright : © Kaouani D (2024).
Abstract
Introduction: Although salmonellosis is very common in Morocco, its involvement in purulent meningitis remains possible, although very rare.
Method: The aim of this work is to study the clinical and paraclinical epidemiological profile as well as the evolution of purulent salmonella meningitis in our department from January 2012 to December 2023 at the Mohammed VI University Hospital in the pediatrics department A in Marrakech.
Results: We report five cases in infants aged 3 to 8 months. We included in our study all meningitis cases whose culture was positive for the Salmonella genus without distinction of species, and this without taking into account the results of blood cultures or possible stool cultures which were negative in all our patients. Our patients were treated with ceftriaxone for an average duration of three weeks with short- and long-term neurological sequelae.
Conclusion: Salmonella meningitis remains rare despite the frequency of enterocolic salmonella infections; however, prevention of salmonella meningitis requires first prevention and adequate treatment of salmonellosis in general.
Keywords: Meningitis; Salmonella; Infant; Lumbar puncture; Ceftriaxone.
Citation: Kaouani D, Elfakiri K, Rada N, Draiss G, Bouskraoui M. Salmonella meningitis: Five cases. J Clin Images Med Case Rep. 2024; 5(11): 3359.
Introduction
Although salmonellosis is very common in Morocco, its involvement in purulent meningitis remains possible, although very rare. Salmonella meningitis, caused by a Gram-negative bacillus of the Enterobacteriaceae family, is a complication that can lead to high mortality rates, significant neurological damage, and a high relapse rate and has become one of the leading causes of Gram-negative bacterial meningitis in developing countries. We report five cases after obtaining patients’ consent.
Methods
We conducted a retrospective study of five cases from January 2012 to October 2024 at the Mohammed VI University Hospital in the pediatric department A in Marrakech. We included in our study all meningitis cases whose culture was positive for the Salmonella genus without distinction of species.
Results
First observation: A male patient, 4 months old, eutrophic, was hospitalized for febrile convulsions with refusal to breastfeed. On clinical examination: Febrile, hypotonic with bulging fontanelle. The cerebrospinal fluid was cloudy with 7000 white blood cells, predominantly polymorphonuclear neutrophils; culture isolated salmonella without distinction of multi-susceptible species; not found in the blood. Coproculture was negative. CRP is 174 mg/l. A CT scan showed hydrocephalus and a dandy walker malformation. The patient was treated with Ceftriaxone 100 mg/kg/day for 19 days. The evolution was favorable under treatment.
Second observation: A male patient aged 4 months, with a history of 7 months of prematurity, a hypotrophic patient, initially hospitalized for febrile convulsions with refusal to breastfeed. On clinical examination: Febrile, hypotonic with bulging fontanelle. The cerebrospinal fluid was cloudy with 12,000 white blood cells, predominantly polymorphonuclear neutrophils. Culture isolated Salmonella sensitive to ceftriaxone and resistant to quinolone; not identified in blood culture or stool culture. CRP is 557 mg/l. Transfontanellar ultrasound showed hydrocephalus. The patient was treated with Ceftriaxone 100 mg/kg/day for 23 days. The evolution was marked by the occurrence of neurological sequelae such as cerebral palsy.
Third observation: A male patient aged 8 months, eutrophic, was hospitalized for febrile convulsive status epilepticus with refusal to suckle and moaning. On clinical examination: Febrile, obtunded, hypotonic with bulging fontanelle. The cerebrospinal fluid was cloudy with 5021 white blood cells with a predominance of polymorphonuclear neutrophils; culture isolated salmonella; not identified in blood culture or stool culture. CRP is 323 mg/l. A CT scan showed the appearance in favor of meningoencephalitis. Patient treated with Ceftriaxone 100 mg/kg/day for 19 days, associated with Ciprofloxacin 20 mg/kg/day for 16 days. The evolution was marked by the occurrence of epilepsy confirmed by electroencephalogram.
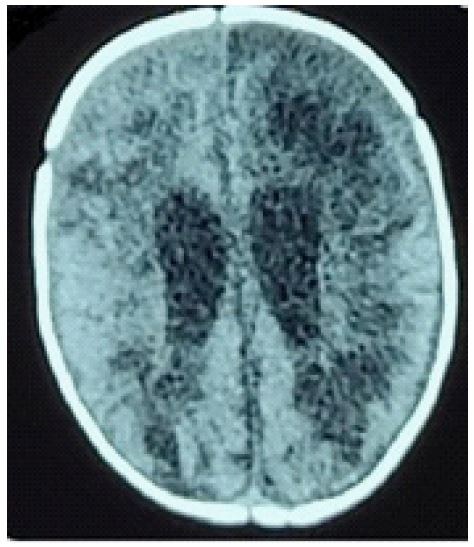
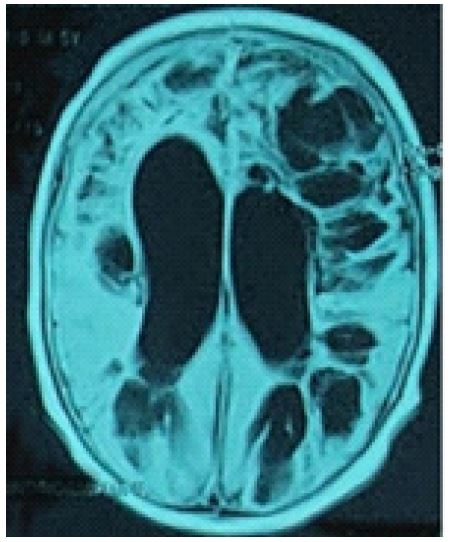
Fourth observation: A male patient aged 3 months with a history of prematurity at 33 weeks of amenorrhea, eutrophic, was hospitalized for generalized febrile convulsions with refusal to breastfeed. On clinical examination: Febrile, hypotonic with bulging fontanelle. The cerebrospinal fluid was cloudy with 1200 white blood cells with a predominance of polymorphonuclear neutrophils; culture isolated salmonella. Distinctions of multisensitive species; not found in the blood. Stool culture was negative. CRP is at 545 mg/l. CT scan showed images in favor of meningoencephalitis (Figure 1), which was subsequently complicated by brain abscess (Figure 2). The patient was treated with Ceftriaxone 100 mg/kg/day for 40 days and Ciprofloxacin 20 mg/kg/day for 7 weeks. The evolution was marked by the occurrence of disseminated intravenous coagulation, which required hospitalization in intensive care. The recovery was marked by the presence of several sequelae: Facial paralysis, triventricular hydrocephalus, and leukomalacia (Figure 3).
Fifth observation: A male patient aged 7 months with a history of prematurity at 30 weeks of amenorrhea, eutrophic, was hospitalized for generalized febrile convulsions with refusal to suckle and moaning. On clinical examination, the patient was febrile and hypotonic with a bulging fontanelle; the cerebrospinal fluid was cloudy with 640 white blood cells with a predominance of polymorphonuclear neutrophils; the culture isolated salmonella; the germ could be identified in the blood culture or in the stool culture. not found in the blood. Stool culture was negative. The CRP is at 320 mg/l. The CT scan showed no abnormalities. The patient was treated with Ceftriaxone 100 mg/kg/day and ciprofloxacin 20 mg/kg/day for 3 weeks. The evolution was favorable under treatment.

Discussion
Salmonella agender of Bacillus Gram Negative (BGN) of the family Enterobacteria. It is a Gram-negative, non-spore-forming, rod-shaped, anaerobic bacterium. Salmonella cells move by means of a peritrile flagellum. The three main diseases caused by Salmonella in humans are non-invasive non-typhoidal salmonellosis, invasive non-typhoidal salmonellosis, and typhoid fever.
Salmonella is transmitted by the fecal-oral route; recognition by the immune system is initiated upon invasion of intestinal epithelial cells, which may initiate an inflammatory response through recruitment of various phagocytic cell lineages that help slow the spread of bacteria to systemic tissues. After invading the abdominal barrier, Salmonella can enter the bloodstream and rarely present with meningitis [1].
Most cases of Salmonella meningitis involve children under one year, mainly under 3 months; this is the case for three patients in our series [2]. In our series, all cases were male. Three of the patients in our series had prematurity as a neurological risk factor, a risk factor that we have not found in the literature. The possibility of Salmonella meningitis should be kept in mind whenever Gram-negative bacteria are observed in the cerebrospinal fluid [3]. Salmonella infection is almost always caused by the fecal-oral route [3]. The source of infection could not be traced in our patients. There was no history of enteric fever and diarrhea in parents or other family members. The signs and symptoms presented by the infants did not differ from other bacteria responsible for meningitis; they were dominated by high fever, irritability, lack of sucking, convulsions, impaired consciousness, and malnutrition [4]. The analysis of the literature and our results support the use of fluoroquinolones in the treatment of salmonella meningitis in infants. The recommended dosage is 20 mg/kg/24 hours in 2 IV injections. The association with a C3G is necessary due to the emergence of resistance to fluoroquinolones for a minimum period of 3 weeks from the date of sterilization of the CSF. These authors specified that the treatment should be much longer in the event of cerebral complications [5]. The literature review shows that the prognosis is generally poor. Fatal complications are reported: thrombophlebitis, brain abscess, subdural hematoma. Neurosensory sequelae, hydrocephalus, vesiculitis, and empyema are also observed, as was the case in most of our patients. Hence the interest in treating digestive salmonellosis with antibiotic therapy in infants exposed to bacteremia and secondary localizations, especially since their immune system is not very mature [5].
Conclusion
Salmonella meningitis remains rare despite the frequency of salmonella enterocolic infections; however, it is clear that prevention of salmonella meningitis begins with prevention and adequate treatment of salmonellosis in general [6].
Conflicts of interest: None.
References
- Kurtz JR, Goggins JA, McLachlan JB. Salmonella infection: Interplay between the bacteria and host immune system. Immunol Lett. 2017; 190: 42-50. doi: 10.1016/j.imlet.2017.07.006.
- Cooke FJ, Ginwalla S, Hampton MD, Wain J, Ross-Russell R, et al. Report of neonatal meningitis due to Salmonella enterica serotype Agona and review of breast milk-associated neonatal Salmonella infections. J Clin Microbiol. 2009; 47(9): 3045-9. doi:10.1128/JCM.01064-09. Epub 2009 Jul 15.
- Adhikary R, Joshi S, Ramakrishnan M. Salmonella typhimurium meningitis in infancy. Indian J Crit Care Med. 2013; 17(6): 392-3. doi:10.4103/0972-5229.123464.
- Wessalowski R, Thomas L, Kivit J, Voit T. Multiple brain abscesses caused by Salmonella enteritidis in a neonate: Successful treatment with ciprofloxacin. Pediatr Infect Dis J. 1993; 12(8): 683-8. doi:10.1097/00006454-199308000-00010.
- Guillaumat C, Dang-Duy TL, Levy C, Cohen R, Leblanc A. Group of pediatricians and microbiologists of the National Observatory of Meningitis. Salmonella meningitis in newborns and infants. The importance of fluoroquinolones. Arch Pediatr. 2008; 15 (3): 161-6. doi: 10.1016/S0929-693X(08)75501-5.
- M Bouskraoui, Z Jouhadi, A Zineddine, J Najib, A Abid. Salmonella meningitis. About 4 cases. Medicine and Infectious Diseases. 1997; 27: 8-9.