
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 5
Recurrent type II second branchial cleft cyst: A case report
B Ramakrishna Reddy1*; Angshuman Dutta2; Anvita Bhansali3
1Resident, Department of ENT-HNS, Command Hospital Airforce, Bangalore, India.
2Consultant & Head, Department of ENT-HNS, Command Hospital Airforce, Bangalore, India.
3Assistant Professor, Department of ENT-HNS, Command Hospital Airforce, Bangalore, India.
*Corresponding Author : B Ramakrishna Reddy
Government Science College, Nrupathunga Road, Bangalore 560001, India.
Email: rakhi.104@gmail.com
Received : Nov 04, 2024
Accepted : Nov 22, 2024
Published : Nov 29, 2024
Archived : www.jcimcr.org
Copyright : © Ramakrishna Reddy B (2024).
Abstract
We present a compelling case of a 29-year-old gentleman who developed a progressively enlarging, painless lump on the left side of his neck. MRI imaging was instrumental in confirming the size and location of the mass. Surgical excision remains the mainstay of treatment in such cases.
Keywords: Branchial cysts; Embryonic anomalies; Surgical excision; Second branchial cleft cyst; Case report.
Citation: Ramakrishna Reddy B, Dutta A, Bhansali A. Recurrent type II second branchial cleft cyst: A case report. J Clin Images Med Case Rep. 2024; 5(11): 3363.
Introduction and importance
Branchial fistulas and cysts are uncommon yet captivating congenital anomalies that result from incomplete or improper development of the branchial apparatus during embryogenesis. These structures arise from the six paired branchial arches, which play a critical role in forming essential head and neck structures such as cartilage, muscles, bones, and blood vessels. In pediatric patients presenting with cervical swellings, branchial anomalies account for approximately 17% of cases, with cysts being the most prevalent, followed by fistulas and sinuses.
Case report
A 29-year-old gentleman from Uttarakhand, employed as a sailor, initially presented to the Indian Naval Hospital in Port Blair in July 2024 with a progressively enlarging, painless lump on the left side of his neck. Over the preceding three months, the lump had grown noticeably larger, and in the week prior to presentation, it became associated with mild discomfort. Importantly, there were no systemic symptoms such as fever, anorexia, or unintentional weight loss. The patient could not identify any specific factors contributing to the onset or progression of the lump.
On July 5, 2024, the patient underwent ultrasound-guided aspiration, followed by treatment with intravenous antibiotics and anti-inflammatory medication, which led to a significant reduction in the swelling. The patient reported symptomatic relief and remained asymptomatic for nearly two months.
However, on September 3, 2024, the patient presented again with a recurrence of the painless neck lump. He was subsequently referred to Command Hospital, Air Force, Bangalore, a tertiary care center, for further evaluation and management.
Upon thorough physical examination, a smooth, non-tender, fluctuant cyst measuring approximately 2×2 cm was palpated on the left side of the neck, anterior to the sternocleidomastoid muscle. The cyst was well-defined and mobile, with no movement upon tongue protrusion or swallowing, and exhibited no signs of inflammation. No lymphadenopathy was detected, and the remainder of the physical examination was unremarkable.
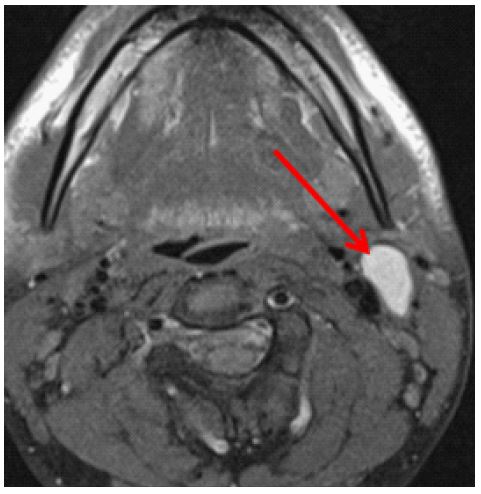
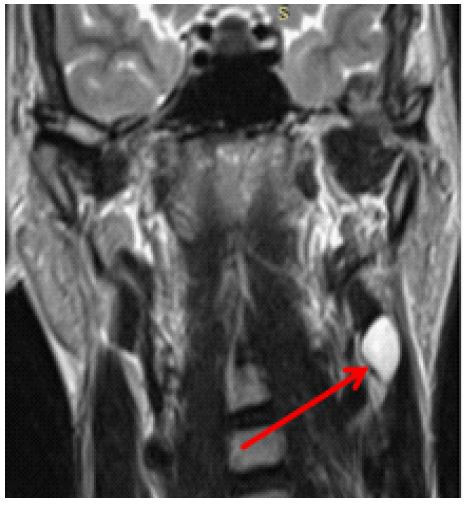
Aspirated fluid from the cyst contained numerous nucleated and anucleated squamous cells. MRI of the neck revealed a well-circumscribed, thin-walled lesion on the left side of the neck measuring 1.2×2.1×2.8 cm, located deep to the sternocleidomastoid and anterolateral to the carotid space. No tract was observed, and the lesion appeared hyperintense on both T1- and T2-weighted images (Figures 1 & 2).
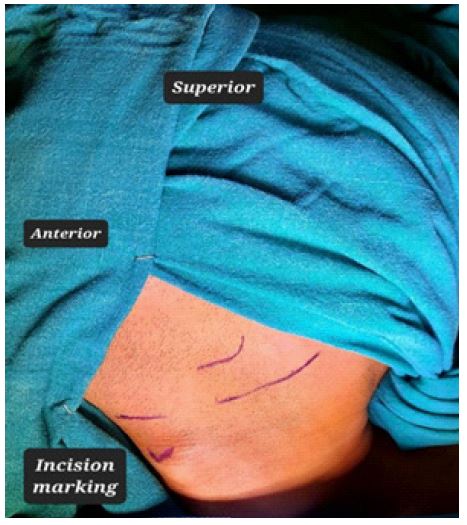
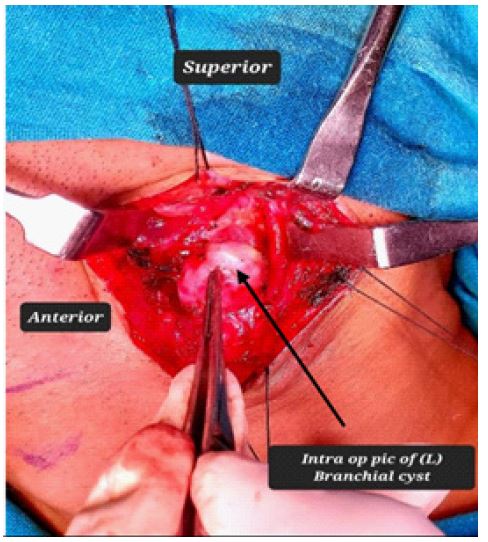
The patient underwent surgical excision of the cyst under general anesthesia to ensure maximum safety and comfort. An elliptical incision was made over the cyst site for optimal access (Figure 3). Upon dissecting around the left sternocleidomastoid muscle, the cystic swelling was visualized lateral to the internal jugular vein (Figure 4). The cyst, measuring 2.5×1.5 cm, was meticulously excised and sent for histopathological evaluation (Figure 5). Special care was taken to preserve the delicate anatomical relationships with the external and internal carotid arteries, ensuring no injury to vital structures. No associated tract was identified during surgery.
Discussion
Branchial fistulas and cysts are rare and fascinating congenital anomalies arising from the incomplete or abnormal development of the branchial apparatus during embryogenesis [1]. These anomalies affect the soft tissues of the neck and can present significant diagnostic and therapeutic challenges. The second Branchial Cleft Cyst (BCC) is the most common type of branchial anomaly, and its classification is best understood through the Bailey-Proctor system, which divides these cysts into four distinct types [3]. Types I and II are the most frequently encountered, while Type IV, located deep within the pharyngeal space, is exceedingly rare and presents a greater diagnostic challenge due to its deep location.
According to the Bailey-Proctor classification, second branchial cleft cysts are categorized as follows [2]:
• Type I: Situated along the anterior border of the sternocleidomastoid muscle, beneath the superficial fascia and platysma.
• Type II: The most common variant, found laterally to the great vessels under the cervical fascia.
• Type III: Positioned between the internal and external carotid arteries, which can complicate surgical excision due to proximity to vital vascular structures.
• Type IV: Rare and located deep in the pharyngeal mucosal space, posing significant diagnostic challenges because of its unusual presentation.
Typically, these cysts present as painless, asymptomatic neck masses, which can lead to delayed diagnosis. The absence of alarming symptoms, such as pain, fever, or weight loss, often results in patients seeking medical attention only after the cyst has grown substantially. Advanced imaging techniques, such as ultrasound, CT, and MRI, are instrumental in diagnosing these anomalies. These modalities not only help confirm the presence of a branchial cleft cyst but also delineate its anatomical relationships with surrounding structures, which is crucial for preoperative planning.
Surgical excision remains the definitive treatment for branchial cleft cysts, aiming to prevent recurrence and minimize the risk of infection or abscess formation [4]. Complete removal is essential to avoid recurrence, which is a known complication if residual cyst tissue remains. The location of the cyst, particularly in Type III and IV, where it lies in close proximity to critical structures like the carotid arteries, underscores the need for meticulous surgical technique [5].
Emerging literature has also highlighted a rare but significant consideration: the potential for malignant transformation [6] in branchial cleft cysts, although this risk remains low. This underscores the importance of early diagnosis and intervention to mitigate any potential long-term risks.
In recent years, there has been a growing interest in minimally invasive surgical techniques, which offer advantages such as reduced operative time, smaller incisions, and faster recovery. These advances in surgical approaches are particularly promising for younger patients and those with high cosmetic concerns, as they reduce complications associated with traditional open surgeries while still achieving excellent outcomes.
Conclusion
Branchial anomalies, including cysts and fistulas, often remain asymptomatic, leading to delayed diagnosis and intervention. A high clinical suspicion, aided by advanced imaging, is crucial for accurate identification. Surgical excision is the definitive treatment, reducing recurrence and complications like infection. Although the risk of malignancy is low, early detection and timely surgery are essential for optimal outcomes. Increased awareness, improved diagnostics, and evolving surgical techniques are key to enhancing patient care and long-term prognosis.
Declarations
Funding: Nil.
Conflict of interest: None.
Informed consent: Taken from patient.
Ethical statement: Permission taken from institutional ethical committee for doing this study.
References
- Hande V, Jain S, Singh CV, Parveen S, Murali M. Type III Second Branchial Cleft Cyst: A Rare Presentation. Cureus. 2022; 14(8): e28568. doi: 10.7759/cureus.28568. PMID: 36185944; PMCID: PMC9520520.
- Berrerhdoche Z, Lachkar A, Benfadil D, Elayoubi F. Second Branchial Cleft Cyst: A Case Report. Cureus. 2022; 14(11): e31815. doi: 10.7759/cureus.31815. PMID: 36579278; PMCID: PMC9783344.
- Safaa Hadi Abdulsattar Alshihmani. A second branchial cleft cyst, a case report. International Journal of Surgery Case Reports. 2023; 108. ISSN 2210-2612. https://doi.org/10.1016/j.ijscr.2023.108429.
- Boringi Mamatha, Bontha Sharath Chandra, Kaur Milanjeet, Shireen Arshia. Branchial cleft cyst - A case report with review of literature. Journal of Orofacial Sciences. 2014; 6(2): 125-128. | DOI: 10.4103/0975-8844.143058
- Patigaroo SA, Hamid W, Ahmed S. et al. Complete Second Branchial Cleft Fistulas: A Clinicosurgical Experience. Indian J Otolaryngol Head Neck Surg. 2023; 75: 1517-1524. https://doi.org/10.1007/s12070-023-03565-z
- Chen Wei, Zhou Yilong, Xu Mengrou, Xu Rong, Wang Qingyu, Xu Hongming, et al. Congenital second branchial cleft anomalies in children: A report of 52 surgical cases, with emphasis on characteristic CT findings, journal-Frontiers in Pediatrics. 2023; 11. DOI:10.3389/fped.2023.1088234,ISSN=2296-2360