
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Clinical Image - Open Access, Volume 5
Parotid gland plasmacytoma: A rare presentation of clinical progression of multiple myeloma
Anncy V Abraham1*; Prasanth L1; Roohie Singh2; Michael John3; Marlapudi Sudheer Kumar4; S Hari Kumar5
1Resident, Department of ENT & HNS, Command Hospital (Eastern Command), Kolkata, India.
2Professor, Department of ENT & HNS, Command Hospital (Eastern Command), Kolkata, India.
3Assistant Professor, Department of Pathology, Command Hospital (Eastern Command), Kolkata, India.
4Resident, Department of ENT & HNS, Command Hospital (Air Force), Bangalore, India.
5HOD, Department of ENT & HNS, Command Hospital (Eastern Command), Kolkata, India.
*Corresponding Author : Anncy V Abraham
Resident, Department of ENT & HNS, Command
Hospital (Eastern Command), Kolkata, India.
Email: anncymol1997@gmail.com
Received : Nov 05, 2024
Accepted : Nov 26, 2024
Published : Dec 03, 2024
Archived : www.jcimcr.org
Copyright : © Abraham AV (2024).
Citation: Abraham AV, Prasanth L, Singh R, John M, Sudheer Kumar M, et al. Parotid gland plasmacytoma: A rare presentation of clinical progression of multiple myeloma. J Clin Images Med Case Rep. 2024; 5(12): 3369.
Description
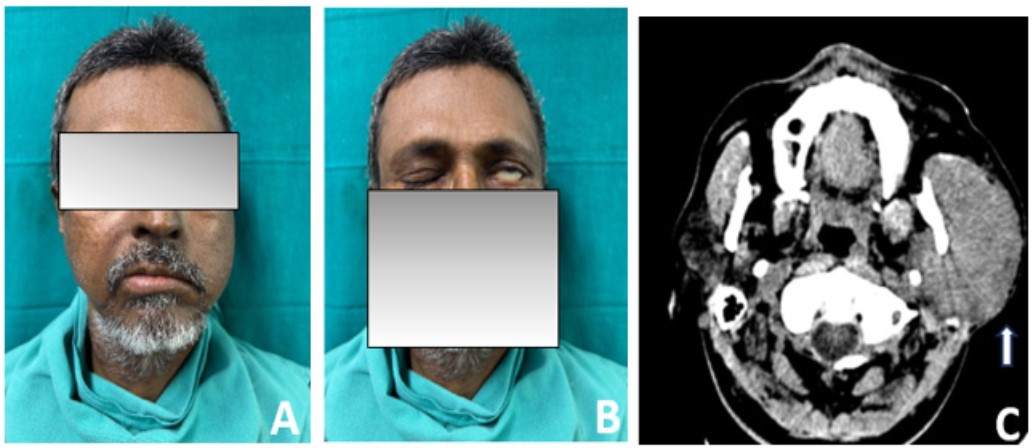
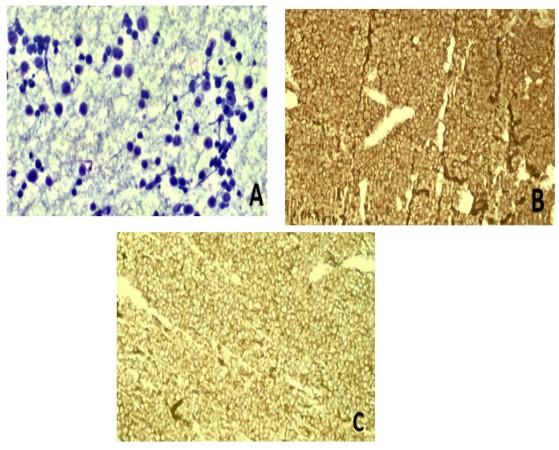
57 years, male, businessman by profession diagnosed with IgA kappa Multiple Myeloma 1 year back, on treatment under haematologist [VRD regimen {Bortezomib (Velcade), Lenalidomide (Revlimid) and Dexamethasone}] presented with complaints of painful (L) preauricular mass from past 12 days associated with deviation of angle of mouth to (R) side (Figure 1A) and inability to close the (L) eye (Figure 1B). On examination, the mass was of size 7 cm x 7cm (approximately) on the (L) side of face, bosselated, firm in consistency with smooth margin, non-tender with no local rise of temperature. It appeared to be originating from (L) parotid. He had (L) lower motor neuron facial nerve palsy (House Brackmann Grade IV). Rest ENT examination was unremarkable. MRI of neck and face revealed a parotid lesion measuring 6.3 x 5.3 x 4.5 cm with significant T2 & STIR hyperintense and T1 hypointense with restricted diffusion involving left parotid gland. A Contrast Enhanced CT (CECT) of face and neck was performed which showed a heterogeneously enhancing lesion involving superficial and deep lobes of left parotid gland (Figure 1C). This was followed by USG (ultrasonography) guided Fine Needle Aspiration Cytology (FNAC) of the mass which showed fibroconnective tissue with sheets of numerous plasma cells. A flow cytometry panel was conducted which was suggestive of Plasmacytoma (Figure 2). Hematologist review was done and patient underwent bone marrow aspiration which showed no increase in plasma cells. The multiple myeloma FISH panel was negative for Del 13q (RB1), Del 17p (TP53), Monosomy1/Gain 1q and IGH gene rearrangement. Skeletal survey showed generalised osteopenia, endosteal scalloping and wedge deformities in multiple vertebrae, ribs, clavicle and sternum.
Hence, a diagnosis of Extramedullary Plasmacytoma was confirmed. In view of this, the therapy was upgraded to Daratumumab, Bortezomib, Cyclophosphamide and Dexamethasone. At present, the patient is under follow-up. The parotid swelling has reduced in size and facial nerve palsy has improved to grade III.
Discussion
Plasmacytoma is a tumor of plasma cells within soft tissue which is traditionally divided into medullary and extramedullary types which could either be solitary or multiple. The most common form is generalized medullary also known as Multiple Myeloma [1]. Extramedullary plasmacytoma is an uncommon tumor mostly involving the mucous or submucous tissues of the upper respiratory tract and alimentary canal, the most frequent sites being the nasal cavity and the nasopharynx [2]. Its occurrence in salivary gland is singularly rare [2,3]. The histopathologic analysis alone is not sufficient. Location and extent, bone involvement and recurrence after treatment are considerably valuable to prognosticate the disease [4]. Parotid gland plasmacytoma is rarely described entity in latent/ initial phase of multiple myeloma. Even rare is clinical progression of multiple myeloma as parotid gland plasmacytoma as seen in this case [5]. A thorough workup and targeted therapy are needed for timely diagnosis and treatment of a patient with multiple myeloma with parotid gland plasmacytoma to get good clinical outcome.
Declarations
Acknowledgement: The authors would like to thank Dr Ashok Meshram (Dept of Hematology). Dr Roma Rai (Dept of Radiology), Dr K J Singh (Dept of Pathology) and the team members (ENT Team) for their contribution in taking care of the patient.
Conflicts of interest: Nil.
Research involving human participants/ or animals: Nil.
Informed consent: Informed consent was taken from the patient for this publication.
Funding: No funding was received to assist with the preparation of this manuscript. The authors have no relevant financial or non-financial interests to disclose.
References
- Kanthan R, Torkian B. Solitary Plasmacytoma of the Parotid Gland with Crystalline Inclusions: A Case Report. World J Surg Oncol. 2003; 1(1): 12. doi: 10.1186/1477-7819-1-12.
- Vainio-Mattila J. Plasmacytoma of the parotid gland. Arch Otolaryngol. 1965; 82(6): 635-7. doi: 10.1001/archotol.1965.00760010637016.
- Rothfield RE, Johnson JT, Stavrides A. Extramedullary plasmacytoma of the parotid. Head Neck. 1990; 12(4): 352-4. doi: 10.1002/hed.2880120414.
- Batsakis JG, Fries GT, Goldman RT, Karlsberg RC. Upper Respiratory Tract Plasmacytoma. Arch Otolaryngol. 1964; 79: 613-8. doi: 10.1001/archotol.1964.00750030626010.
- Goyal H, Sawhney H, Abdu A. Clinical progression of multiple myeloma presenting as parotid gland plasmacytoma. Int J Hematol. 2013; 97(2): 297-8. doi: 10.1007/s12185-013-1274-3.