
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 5
A rare case of IgG4 related disease with hepato-biliary, pancreatic and renal involvement successfully treated with rituximab: A case report
Irene Spinelli1*; Adriano De Santis2; Marcella Visentini3; Massimo Fiorilli3; Mariana Forlino2; Bruna Cerbelli4; Martina Leopizzi4; Giulia d’Amati5
1CEMAD (Centro Malattie Apparato Digerente), University Hospital Foundation A. Gemelli IRCCS, Largo A. Gemelli, 8, 00168, Rome, Italy.
2Department of Translational and Precision Medicine, Sapienza University of Rome, Foundation University Polyclinic A 37, 00185, Rome, Italy.
3Department of Internal Medicine and Clinical Immunology, Sapienza University of Rome, University Avenue 37, 00185, Rome, Italy.
4Department of Medical-Surgical Sciences and Biotechnologies, Sapienza University of Rome, Policlinic Umberto I, Viale Regina Elena 324, 00161, Rome, Italy.
5Department of Radiological, Oncological and Pathological Sciences, Sapienza University of Rome, Policlinic Umberto I, Viale Regina Elena 324, 00161, Rome, Italy.
*Corresponding Author : Irene Spinelli
Department of Internal Medicine and
Gastroenterology, University Hospital Foundation
A. Gemelli IRCCS, Largo A. Gemelli, 8, 00168, Rome,
Italy.
Email: irenespinelli1@gmail.com
Received : Nov 04, 2024
Accepted : Nov 26, 2024
Published : Dec 03, 2024
Archived : www.jcimcr.org
Copyright : © Spinelli I (2024).
Abstract
IgG4-related disease is a systemic immune-mediated disease characterized by chronic fibrotic inflammation and IgG4-positive plasma cell tissue infiltration that can involve different organ systems. We report the case of a patient who presented with obstructive jaundice as well as cholecystitis and biliary tree dilatation on imaging. The patient underwent radical cholecystectomy, but diagnosis of IgG4-related cholecystitis, cholangitis and pancreatitis was made later. A steroid therapy was started obtaining initially a good response. Over time, he developed a progressive increase in serum creatinine, and a renal biopsy showed kidney involvement of disease compatible with IgG4 nephritis. Subsequently, due to a patient’s glucocorticoid intolerance, he was treated with Rituximab, obtaining stabilization of renal disease with absence of relapses after two years.
Keywords: IgG4; Pancreatitis; Cholangitis; Nephritis; Rituximab.
Citation: Spinelli I, Santis AD, Visentini M, Fiorilli M, Forlino M, et al. A rare case of IgG4 related disease with hepato-biliary, pancreatic and renal involvement successfully treated with rituximab: A case report. J Clin Images Med Case Rep. 2024; 5(12): 3370.
Introduction
IgG4-related disease is a recently described disease affecting multiple organs including pancreas, liver, bile ducts, gallbladder, kidneys, salivary glands, thyroid, retroperitoneum, oesophagus, and other tissues. Involved organs can exhibit swelling, enlargement, or mass-forming lesions. Histopathological features include IgG4-positive lymphoplas-macytic infiltration, storiform fibrosis, obliterative venulitis and modest tissue eosino-philia. Laboratory findings usually, but not always, consist of high serum IgG4 and IgE levels and eosinophilia. Due to lack of evidence, the optimal treatment is still on debate, but actually glucocorticoid therapy is the first line because it induces prompt response and disease remission. Nevertheless, patients may become steroid intolerant or resistant, or develop relapse of disease. In these cases, immunomodulatory agents are a good al-ternative to maintain remission, in particular Rituximab, a depleting monoclonal anti-body against the CD20 antigen on B cells.
Here, we present the case of a patient with IgG4-related disease with unusual altogether biliary, pancreatic, and renal involvement and initial optimal response to steroid therapy. Since the worsening of renal function and his progressive glucocorticoid intolerance, four cycles of Rituximab were administered, leading to safe discontinuation of steroid therapy, persistent quiescent activity of disease and improvement of kidney condition.
Case report
A 68-year-old man was admitted to his regional hospital because of painless jaundice, dark urine and acholic stools. Past medical history was remarkable for arterial hypertension, myocardial infarction treated with Percutaneous Coronary Intervention (PCI) and eosinophilia of unknown origin for two years. Physical examination showed jaundice and hepatomegaly. No laboratory test available on admission. Patient underwent ultrasound scan that revealed intrahepatic bile ducts and common bile duct dilatation with a hypoechoic mass lesion in the head of pancreas. A contrast-enhanced Computed Tomography (CT) scan confirmed those findings but showing also pancreatic duct dilatation. Suspecting a periampullary disease, two Endoscopic Retrograde Cholangi-opancreatography (ERCP) with stenting and brushing were performed. Cytologic examination was compatible with hyperplas-tic-reactive biliary epithelium. Subsequent CT scan and endoscopic Ultrasound (EUS) described thickening of gallbladder and common bile duct walls with gallbladder stones. The patient underwent cholecystectomy that revealed a subacute cholecystitis with high tissue eosinophilia.
Few months following surgery, the patient was admitted to our hospital because of ingravescent pruritus, asthenia, and weight loss (10 kg). Laboratory investigations are showed in (Table 1).
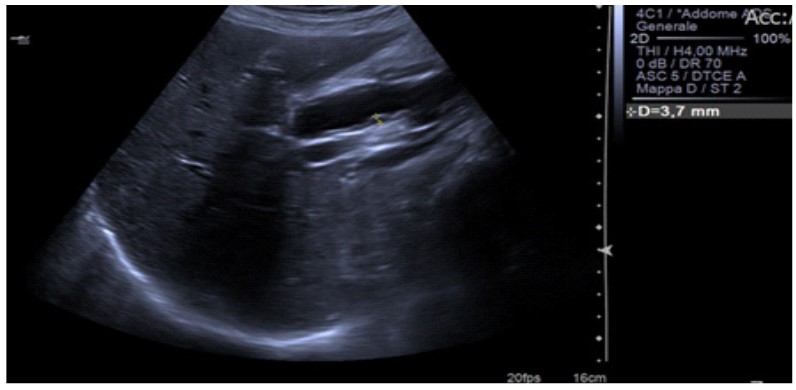
Patient underwent abdominal ultrasound examination, that revealed intrahepatic bile ducts and common bile duct dilatation with thickened wall (Figure 1) and upper limit head of pancreas diameter (Table 2) with heterogeneous parenchyma, and MR cholan-giopancreatography (MRCP), that showed dilatation of common bile duct with distal stricture suspected of malignancy.
(Figure 2A-2D) Renal biopsy showed a mixed interstitial inflammatory cell infiltrate composed by many plasma cells (Figure 2A; hematoxylin and eosin, 10X) stained for CD138 (Figure 2B; 40X). Plasma cells were positive for IgG4 immunostaining (Figure 2C; 40X) and negative for IgG (Figure 2D; 40X).
(Figure 2E-2H) Hematoxylin and eosin (Figure 2E; 20X) stain showed a dense plasma cell infiltration stained for CD138 (Figure 2F; 20X) in all gallbladder layers composed by a large prevalence of IgG4 plasma cells (Figure 2G; 20X) with the IgG4/IgG positive cell ratio exceeded 40% (Figure 2H; 20X). Promptly after the diagnosis, the patient was started with glucocorticoid therapy (deflazacort 12 mg). After six months, he presented body weight regain, normalization of cholestatic and pancreatic enzymes. A follow-up ultrasound scan of the abdomen was repeated, and it showed normal intrahe-patic bile ducts, reduction of common bile duct diameter and wall thickness (Figure 3), normal head of pancreas diameter with heterogeneous parenchyma. In consideration of ameliorated conditions, glucocorticoid therapy was tapered to half dosage per day.
At the same time, we noticed a progressive increase of serum creatinine value that passed from 1.1 mg/dl, at the beginning of clinical history, to 2.8 mg/dl, in about one year and half. Urine analysis was normal, with lower limits of C3 and C4 values. Renal ultrasound revealed absent corticomedullary differentiation and normal renal resistive index of both renal arteries, without lesions or masses. To examine renal status, a kidney biopsy was performed, reporting final diagnosis of IgG4-related tubulointerstitial nephritis (IgG4-TIN) (Figure 2). Unfortunately, over time patient developed a progressive heart failure, and further increase of se-rum creatinine (3.2 mg/dl after two other months) (Figure 4).
In consideration of his several cardiological comorbidities and rapid deterioration of renal function despite therapy, we evaluated him as steroid dependent and intolerant and decided to switch to a different therapy. He was treated with Rituximab (4 weekly intravenous doses of 500 mg each) without side effects, and he promptly responded to this intervention with improvements of clinical symptoms and successful tapering of glucocorticoids to discontinuation. Patient was evaluated monthly for the first three months after infusions and then every three months. Despite previous rapid kidney deterioration, serum creatinine level didn’t continue to rise up, but showed a minimal improvement and stabilization (2.7 mg/dl after nine months’ follow-up). Accordingly to medical literature [1,2], IgG4 concentrations declined following this treatment, passing from 15.3 g/L (value before Rituximab) to 4.22 g/L (value nine months after Rituximab). The other immunoglobulin class that showed a reduction was IgE, with a concentration of 355 KU/L nine months after infusions. Eosinophil counts changed significantly after glucocorticoid therapy, but not following rituximab treatment. Patient underwent a follow-up abdominal ultrasound examination that confirmed disease remis-sion (Figure 5).
Nine months after Rituximab therapy he remained free of disease progression and relapses, in both gastrointestinal and urinary tracts, and it was confirmed two years later as well.
Table 1: Laboratory tests.
| Laboratory results | Admission to our hospital | 6 months after steroid therapy | 9 months after rituximab therapy | 2 years after rituximab therapy |
|---|---|---|---|---|
| Hb (g/dl) | 11.8 | 13.4 | 13.4 | 13.8 |
| WBC (x10³/µL) | 7.95 | 13.97 | 10.46 | 11.41 |
| Eosinophils (x10³/µL) | 1.2 | 1.3 | 0.6 | 0.6 |
| PLTS (x10³/µL) | 162 | 232 | 222 | 223 |
| AST (UI/L) UNV 45 | 26 | 15 | 17 | 23 |
| ALT (UI/L) UNV 40 | 26 | 9 | 28 | 33 |
| Alkaline phosphatase (UI/L) UNV 129 | 138 | 61 | 88 | 94 |
| GGT (UI/L) UNV 61 | 150 | 13 | 52 | 40 |
| Bilirubin (mg/dl) UNV 1.2 | 0.6 | 0.3 | 0.5 | 0.6 |
| Amilase (UI/L) UNV 100 | 29 | 38 | 32 | 41 |
| Lipase (UI/L) UNV 60 | 18 | 29 | 14 | 29 |
| IgE (UI/ml) UNV 100 | 1079 | 500 | 355 | 207 |
| IgG4 (mg/dl) UNV 86 | 4310 | 1530 | 422 | 459 |
| Creatinine (mg/dl) | 1.8 | 2.8 | 2.7 | 2.8 |
UNV: Upper Normal Value.
Table 2: Abdominal ultrasound examination parameters.
| Abdominal organ | Admission to our hospital | 6 months after steroid therapy | 9 months after rituximab therapy | 2 years after rituximab therapy |
|---|---|---|---|---|
| Intrahepatic bile ducts | Dilatation | Normal | Normal | Normal |
| Common bile duct diameter (mm) | 16 | 10.8 | 7.7 | 8.4 |
| Common bile duct wall (mm) | 3.7 | 1.9 | 0.9 | 0.9 |
| Head of pancreas (mm) | 2.7 | 2.2 | 2.3 | 1.8 |




Discussion
IgG4-RD is a recently recognized multi-organs disorder whose medical literature mostly consists of case reports and small case series, but the awareness of this disease is increased world-wide [3-8]. Diagnostic process is commonly challenging and is based on close cooperation between different specialists like gastroenterologist, radiologist, pathologist, and surgeon. IgG4 disease clinically presents with multifocal tumour-like masses which create an obvious confusion with malignancy. The main difference between these two entities is that IgG4 disease tends to respond dramatically to steroids as opposed to malignancy, which would need surgical intervention. The difficulty to recognize this benign entity can result in incorrect management and unnecessary surgical procedures. On the contrary, prompt identification of the disease can help in prevention of the sequelae. Due to the complexity of our case, diagnosis was subjected to a delay of about one year from onset of symptoms and patient underwent avoidable chole-cystectomy.
The peculiarity of this case also emerges in multiorgan involvement of the disease. The pancreas, bile ducts and gallbladders are frequently affected [9], but multiple organs have rarely been documented [10]. The picture reported above is extremely rare and describes IgG4-RD with manifestations of pancreatitis, cholangitis, cholecystitis, and interstitial nephritis. A prospective study of 28 patients showed four sites involvement in only 18 % of patients and nobody reported the same affected organs of the patient [11]. According to results of a large cohort study of 125 patients with IgG4-RD, the frequencies of pancreas, kidney and biliary tract involvement were respectively 19%, 12% and 10% [12]. The optimal treatment for IgG4 disease is actually unknown, but the mainstay is represented by glucocorticoids, which are the first-line agent for induction of remission. Despite their efficacy, two major issues are related to this treatment. First, their systemic chronic side effects, as osteoporosis and complications of glucose intolerance. Second, many patients relapse over time and a large percentage present other organs involvement [13]. Therefore, immunosuppressive agents have been employed in patients with refractory or recurrent IgG4-RD but data regarding their efficacy are still few and based primarily on retrospective case series and case reports. Rituximab, a monoclonal antibody directed against CD20 antigen on B cells, has been described to have a role in treatment of patients with incomplete response or major contrain-dication to glucocorticoid therapy, in the absence of major side effects [1,2,14]. We described a case of IgG4 related disease pa-tient, with pancreatitis, cholangitis, cholecystitis, and interstitial nephritis manifestations, a rare multiorgan involvement, success-fully treated with Rituximab. The therapy was well tolerated during infusions and follow-up, and we assisted, according to the lit-erature, to a decline in serum IgG4 and IgE concentrations, in addition to a maintenance of serum creatinine values despite its previous increase, meaning a stop in kidney deterioration and a preservation of renal function. After two years from rituximab therapy, the patient was still free of disease. In conclusion, IgG4-related disease with multiorgan involvement is a rare entity and rituximab is a therapeutic alternative for all the difficult-to-treat and relapsing cases.
Declarations
Author contributions: Conceptualization IS and ADS; Methodology IS; Software IS and ADS; Validation ADS, BC, ML; For- mal analysis IS and ADS; Investigation IS, ADS, MF, MV, BC, ML, GDA; Resources IS, ADS; Mariana Forlino MV, BC, ML, GDA; Data curation IS, and A.S; writing-original draft preparation IS; writing-review and editing IS, ADS, BC, ML; visualization ADS; Massimo Fiorilli GDA; Supervision AD; Massimo Fiorilli GDA; project administration IS, and ADS. All authors have read and agreed to the published version of the manuscript.
Funding: This research received no external funding.
Institutional review board statement: Not applicable.
Data availability statement: The datasets presented in this article are not readily available due to privacy.
Conflicts of interest: The authors declare no conflicts of interest.
References
- Khosroshahi A et al. Rituximab for the treatment of IgG4-related disease: lessons from 10 consecutive patients. Medi-cine (Balti- more). 2012; 91(1): 57-66. doi: 10.1097/MD.0b013e3182431ef6. PMID: 22210556.
- Khosroshahi A, Bloch DB, Deshpande V, Stone JH. Rituximab therapy leads to rapid decline of serum IgG4 levels and prompt clinical improvement in IgG4-related systemic disease. Arthritis Rheum. 2010; 62: 1755-1762.
- Matsubayashi H, Sawai H, Kimura H, Yamaguchi Y, Tanaka M, et al. Characteristics of autoimmune pancreatitis based on serum IgG4 level. Dig Liver Dis. 2011; 43: 731-5.
- Ohta N, Kurakami K, Ishida A, Furukawa T, Saito F, et al. Clinical and pathological characteristics of IgG4-related scle-rosing sialadenitis. Laryngoscope. 2012; 122: 572-7.
- Kuruma S, Kamisawa T, Tabata T, Hara S, Fujiwara T, et al. Clinical characteristics of patients with autoimmune pan-creatitis with or without Mikulicz’s disease and Mikulicz’s disease alone. Gut Liver 2013; 7: 96-9.
- Saeki T, Nishi S, Imai N, Ito T, Yamazaki H, et al. Clinicopathological characteristics of patients with IgG4-related tu-bulointerstitial nephritis. Kidney Int. 2010; 78: 1016-23.
- Patel H, Khalili K, Kyoung KT, Yazdi L, Lee E, et al. IgG4 related disease-a retrospective descriptive study highlighting Canadian experiences in diagnosis and management. BMC Gastroenterol. 2013; 13: 168.
- Löhr J-M, Beuers U, Vujasinovic M, et al. European Guideline on IgG4-related digestive disease – UEG and SGF evi-dence-based recommendations. United European Gastroenterol J. 2020; 8: 637-66.
- Nakazawa T, Naitoh I, Hayashi K, et al. Diagnostic criteria for IgG4-related sclerosing cholangitis based on cholangio-graphic classification. J Gastroenterol. 2012; 47(1): 79-87. http://dx.doi. org/10.1007/s00535-011-0465-z.
- Vasaitis L. IgG4-related disease: A relatively new concept for clinicians. Eur J Intern Med. 2016; 27: 1-9. doi: 10.1016/j. ejim.2015.09.022. Epub 2015 Oct 16.
- Chen H, Lin W, Wang Q et al. IgG4-related disease in a Chinese cohort: a prospective study. Scand J Rheumatol. 2014; 43: 70- 74.
- Wallace ZS, Deshpande V, Mattoo H, et al. IgG4-related disease: clinical and laboratory features in 125 patients. Arthri-tis Rheumatol. 2015. http://dx.doi.org/10.1002/ art.39205.
- Khosroshahi A, Stone JH. Treatment approaches to IgG4-related systemic disease. Curr Opin Rheumatol. 2011; 23(1): 67-71. doi: 10.1097/BOR.0b013e328341a240.
- Carruthers MN, Topazian MD, Khosroshahi A, Witzig TE, Wallace ZS, et al. Rituximab for IgG4-related disease: A pro-spective, open-label trial. Ann Rheum Dis. 2015; 74(6): 1171-7. doi: 10.1136/annrheumdis-2014-206605.