
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 5
Interventional treatment of a rare case of pulmonary arteriovenous fistula causing cerebral embolism
Yue Zhao; Xingwu Xie; Guangbin Chen*
Department of Radiology, Shiyan People’s Hospital, Shiyan, Hubei, China.
*Corresponding Author : Guangbin Chen
Department of Radiology, Shiyan People’s Hospital,
Shiyan, Hubei, China.
Tel: 13635713448; Email: 13635713448@163.com
Received : Nov 10, 2024
Accepted : Nov 28, 2024
Published : Dec 05, 2024
Archived : www.jcimcr.org
Copyright : © Chen G (2024).
Abstract
Pulmonary Arteriovenous Fistula (PAVF) is a rare vascular malformation that directly connects the pulmonary and systemic circulations. This case reports the case of a middle-aged female who was admitted for ureteral stones and experienced sudden onset of consciousness disturbance, respiratory distress, and cardiac arrest during hospitalization. Ultrasound examination revealed deep vein thrombosis in the lower limbs, and brain MRI indicated cerebral infarction. Emergency thrombolysis and thrombectomy were performed by the neurology team. Subsequent pulmonary artery CTA and CTV confirmed the presence of a pulmonary arteriovenous fistula. The interventional radiology department placed a lower limb filter and performed pulmonary artery embolization. With close multidisciplinary collaboration, the patient’s condition improved.
Keywords: Pulmonary arteriovenous fistula; Cerebral infarction; Interventional therapy.
Citation: Zhao Y, Xie X, Chen G. Interventional treatment of a rare case of pulmonary arteriovenous fistula causing cerebral embolism. J Clin Images Med Case Rep. 2024; 5(12): 3373.
Clinical data
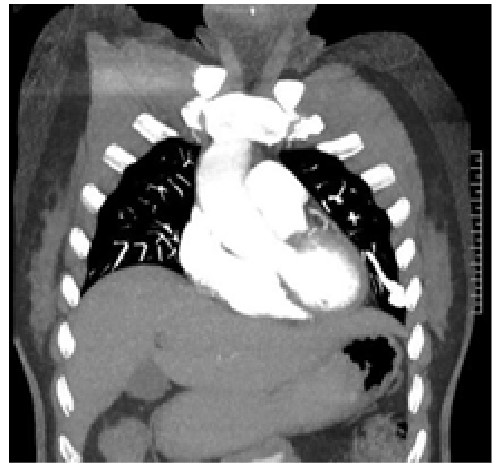
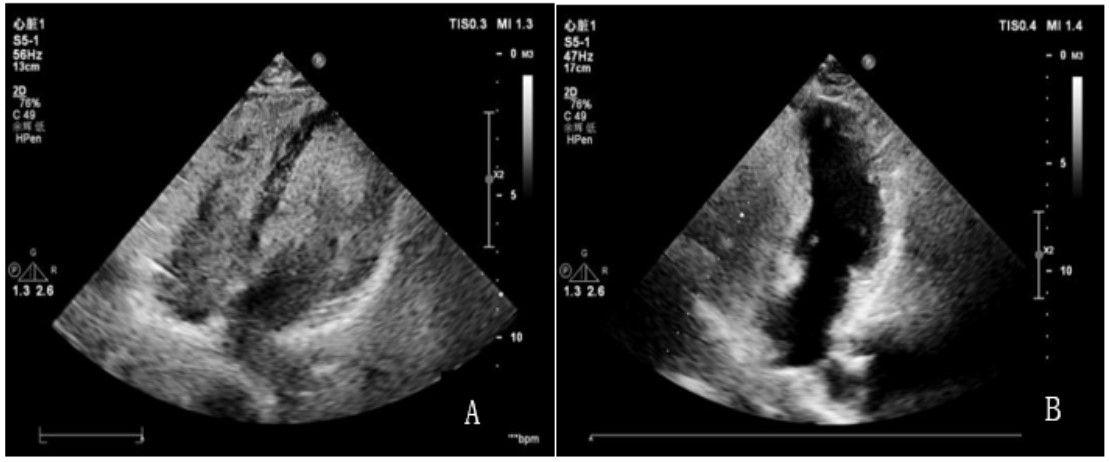
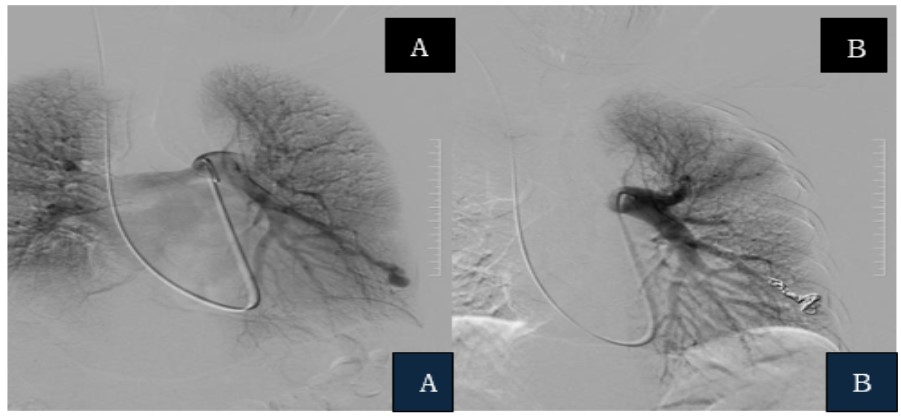
The patient, a female in her fifties, was admitted on July 2, 2024, due to “10 hours of right flank pain.” After undergoing an emergency CT scan at Shiyan People’s Hospital, a right ureteral stone was suspected. On July 3, the patient underwent transurethral ureteroscopy and renal pelvis laser lithotripsy with stone extraction, returning to the ward in stable condition post-operatively. However, on July 4 at 7:57 am, the patient suddenly collapsed while walking at her bedside, experiencing abrupt loss of consciousness, unresponsiveness to verbal stimulation, weak carotid pulse, cyanosis of the lips, and cardiac arrest. Immediate and continuous Cardiopulmonary Resuscitation (CPR) was administered, including sustained chest compressions, bag-mask ventilation, and intravenous access establishment. An emergency ICU consultation was promptly called, and at 8:02 am, endotracheal intubation was performed for mechanical ventilation. The patient was then transferred to the ICU for further resuscitation efforts. During her ICU stay, a Doppler ultrasound revealed thrombosis in the right calf, and arterial ultrasound of both lower limbs showed segmental atherosclerosis. Head MRI revealed multiple patchy lesions in the bilateral frontal and parietal lobes with isointense T1 and slightly hyperintense T2 signals. DWI demonstrated a patchy, slightly high signal in the mid- brain (approximately 8 mm), with low signal on ADC, suggesting a possible midbrain infarction. MRA of the head showed severe atherosclerosis with significant stenosis and potential partial occlusion of the left posterior cerebral artery segments P1-P3, vertebral artery, and basilar artery. A subsequent cerebral angiography performed by the neurology department confirmed an acute basilar artery occlusion, followed by a successful percutaneous intracranial thrombectomy and intra-arterial thrombolysis, which achieved complete visualization of the basilar artery on post-procedural angiography. Postoperatively, the patient’s condition improved. Follow-up CT of the head and lungs revealed a patchy low-density area in the right occipital lobe, with no abnormal density observed in the remaining brain paren- chyma; a vascular abnormality was suspected in the left lingual segment of the upper lung. Further CT angiography showed pulmonary embolism in both lungs, tortuous vascular shadow in the left lung lingual lobe, suggestive of a pulmonary arteriovenous fistula (PAVF; Figure 1). An enhanced ultrasound study was performed, where 8 ml of saline mixed with 1 ml of blood and 1 ml of air was injected into a superficial vein of the right forearm, revealing dense echogenic bubbles in the right atrium. Upon performing the Valsalva maneuver, dense bubbles filled the left atrium, indicating a positive pulmonary arteriovenous fistula (Figure 2A). A multidisciplinary team concluded that the brain embolism was likely caused by a lower extremity thrombus that had passed through the pulmonary venous fistula. On October 9, the interventional radiology department performed placement of a vena cava filter, pulmonary artery embolization, inferior vena cava angiography, and pulmonary artery angiography. A Pig catheter was guided into a branch of the pulmonary artery, where an aneurysmal expansion distal to a left pulmonary vein branch was identified, with early visualization of the adjacent pulmonary vein suggesting an arteriovenous fistula. The Pig catheter was replaced with a single-curve catheter and an Sp catheter, through which four fibered platinum coils were deployed. Post-embolization angiography showed resolution of the arteriovenous fistula. Two weeks postoperatively, a follow- up transthoracic echocardiogram indicated a negative bubble test (Figure 2B), and during the three-month follow-up period, the patient experienced no further cerebrovascular events.
Discussion
Pulmonary arteriovenous fistula is a rare vascular anomaly that directly connects the pulmonary and systemic circulations [1]. Its clinical manifestations are varied; patients may experience varying degrees of dyspnea, cyanosis, clubbing, or chest pain. However, most PAVF cases are asymptomatic, complicating the diagnostic process. Cerebral embolism is a rare complication, with PAVF accounting for only 0.02% of clinically observed cerebral embolisms. Once cerebral embolism occurs as a complication, it poses a life-threatening risk to the patient. The patient in this case was initially admitted for a ureteral stone but later experienced sudden collapse, loss of consciousness, respiratory distress, and cardiac arrest, making it challenging to associate these events with the rare condition of an arteriovenous fistula. Studies have confirmed that pulmonary arteriovenous fistula is an independent risk factor for ischemic stroke and transient ischemic attacks, with multiple pulmonary arteriovenous fistulas carrying a higher incidence of ischemic stroke compared to solitary lesions [2]. This case highlights the importance for clinicians to consider abnormalities in the pulmonary vascular system when dealing with unexplained strokes. A comprehensive evaluation using multimodal imaging, such as chest CTA and CTV, MRI, and ultrasound, should be conducted to enhance the early diagnostic rate of PAVF [3]. In addition to thorough diagnostic evaluations, multidisciplinary collaboration is crucial for the management of complex cases like this [4]. This case involved collaboration across multiple departments, including respiratory medicine, radiology, ICU, neurology, and interventional radiology, encompassing resuscitation, imaging diagnosis, and interventional treatment. This coordinated approach led to successful treatment of the patient, underscoring the importance of multidisciplinary teamwork in the management of PAVF. In recent years, numerous case reports have highlighted the role of multidisciplinary teams in managing complex vascular diseases. For conditions like PAVF, which may affect multiple organ systems, such collaboration can significantly improve diagnostic and treatment efficiency, save lives, and reduce delays in the diagnostic and therapeutic process. Interventional embolization is considered one of the most effective treatments for PAVF [5,6]. Recent studies show that embolizing abnormal arteriovenous channels, through interventional procedures can significantly reduce the incidence of complications such as cerebral embolism and hypoxemia [7,8]. In this case, after the patient underwent pulmonary artery embolization, imaging studies showed complete resolution of the arteriovenous fistula, and the patient’s symptoms rapidly improved. Interventional embolization not only effectively controls the condition in the acute phase but also has a highly positive impact on long-term prognosis. Additionally, individualized treatment plans are increasingly becoming an important trend in the management of PAVF [9]. Precise preoperative multimodal imaging assessments and real-time intraoperative interventional angiography guidance have greatly improved the accuracy and success rates of pulmonary artery embolization [10].
Conclusion
The incidence of PAVF is low and lacks specific symptoms, making it easily overlooked in clinical practice. However, its complications can be life-threatening. Therefore, for cases of unexplained cerebral embolism, comprehensive imaging examinations should be conducted. Multidisciplinary collaboration is essential for accurate diagnosis and treatment. Clinicians should increase awareness of PAVF and its potential complications to reduce the likelihood of missed or misdiagnosis. Timely intervention, such as interventional treatment, can effectively save lives and improve patient prognosis.
Declarations
Author contribution statement: The contributions of each author to this research are as follows.
Zhao Yue: Responsible for writing the initial draft and conducting data collection and analysis.
Xie Xingwu: Provided significant revisions, enhancing the quality and depth of the paper.
Chen Guangbin: Offered guidance on the research framework, helping to clarify the research direction.
All authors have agreed to the final version submitted and share responsibility for the integrity and results of the research.
Acknowledgements: I would like to express my gratitude to all those who helped me during the writing of this article.
Conflicts of interest: The authors declare that there is no conflict of interest.
Funding: This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Data availability statement: All data generated or analysed during this study are included within this published article.
References
- Joshi A, Saini V, Bheemavarapu B, et al. Bilateral Pulmonary Arteriovenous Malformations: Challenges in a Rare and Complex Case[J]. Cureus, 2024; 16(9): 70231.
- Topiwala KK, Patel SD, Pervez M, et al. Ischemic Stroke in Patients with Pulmonary Arteriovenous Fistulas [J]. 2021; 52(7): 311-315.
- Wozniak L, Skapska S, Marszalek K. Ursolic Acid-A Pentacyclic Triterpenoid with a Wide Spectrum of Pharmacological Activities [J]. 2015; 20(11): 20614-20641.
- Takao S, Masuda T, Yamada T, et al. Pulmonary arteriovenous malformation exhibiting recanalization >10 years after coil embolization: Two case reports [J]. Medicine (Baltimore). 2020; 99(2): 18694.
- Perez-Oliver T, Vela-Martinez E, Martin-Zamora S. Pulmonary embolism after embolization of vein of Galen [J]. An Pediatr (Engl Ed). 2023; 98(3): 236.
- Iwata S, Iwashita T, Senju A, et al. Successful Surgical Resection of Pancreatic Arteriovenous Malformation Complicated by Acute Pancreatitis: A Case Report. Intern Med. 2024.
- Tajima H, Kasai H, Sugiura T, et al. Pulmonary arteriovenous fistula complicated by venous thromboembolism and paradoxical cerebral infarction during early pregnancy [J]. BMJ Case Rep. 2018.
- Yu Q, Zangan S, La Riviere P, et al. Vascular Plugs Improve Pulmonary Arteriovenous Malformation Occlusion over Coil Embolization Alone: A Proof-of-Concept Study Using Dual-Energy CT [J]. J Vasc Interv Radiol. 2024; 35(10): 1492-1497.
- Fish A, Wang D, Knight E, et al. Recurrence of Pulmonary Arteriovenous Malformation after Embolization in Patients with Pulmonary Hypertension [J]. J Vasc Interv Radiol, 2024; 35(8): 1148-1153.
- Yu Q, Zangan S, Funaki B. Preliminary Experience with a Low- Profile High-Density Braid Occluder for Transcatheter Embolization of Pulmonary Arteriovenous Malformations [J]. J Vasc Interv Radiol. 2024; 35(1): 32-35.