
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Short Report - Open Access, Volume 5
Tubular carcinoid of the appendix: A rare variant of the benign carcinoid tumor
Betül Peker Cengiz1*; Nilhan Kaya1; Hayrettin Dizen2
1Department of Pathology, Yunus Emre State Hospital, Eskisehir, Turkey.
2Department of General Surgery, Private Eskişehir Acıbadem Hospital, Eskisehir, Turkey.
*Corresponding Author : Betul Peker Cengiz
Department of Pathology, Yunus Emre State
Hospital, Eskisehir, Turkey.
Tel: 05055978868, Fax: 02222392678;
Email: betip76@yahoo.com
Received : Nov 14, 2024
Accepted : Nov 29, 2024
Published : Dec 06, 2024
Archived : www.jcimcr.org
Copyright : © Cengiz BP (2024).
Abstract
Tubular carcinoid tumor of the appendix is a rare pathology, diagnosed incidentally during histopathological examination of the appendectomy specimen. In the literature, a few cases have been reported. We presented here 28 years of age female, who was admitted in the emergency department with symptoms of acute appendicitis. After the appendectomy was performed. The final diagnosis of tubular carcinoid of appendix was confirmed in respect to histopathological examination.
Keywords: Tubular; Carcinoid; Tumor; Appendix.
Citation: Cengiz BP, Kaya N, Dizen H. Tubular carcinoid of the appendix: A rare variant of the benign carcinoid tumor. J Clin Images Med Case Rep. 2024; 5(12): 3375.
Introduction
Carcinoid tumor is not a rare neoplasm and usually arises at the gastrointestinal tract (appendix, stomach, small intestine, colon and rectum) and in the lung [1]. Although appendix is the most common localization for carcinoid tumors, it is diagnosed in 1 out of every 300 appendectomies [1]. They can occur at any age, although they occur most commonly in the 4th or 5th decade of life. They more affected in women [1]. Clinical presentation of the carcinoid tumor of the appendix usually resembles that of acute appendicitis and the diagnosis is often incidental. Tubular carcinoid is uncommon. Appendiceal tubular carcinoid is a uncommon variant of well differentiated neuroendocrine tumor [2]. In the literature, it is presented a few reports. We presented here a rare case of tubular carcinoid of the appendix.
Case report
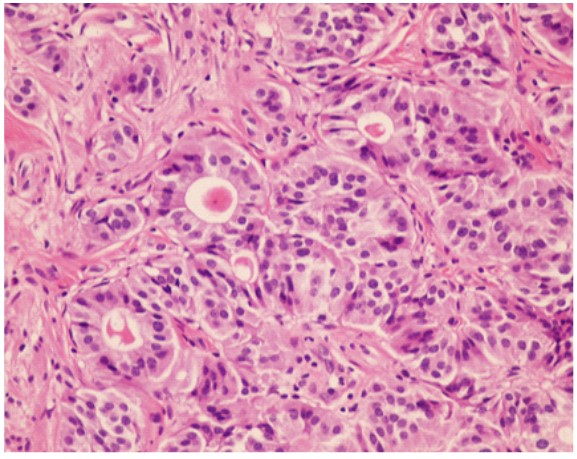
A 28-years-old female patient presented to the emergency department with complaining for abdominal pain in right lower quadrant. On physical exam, she was afebrile with rebound tenderness in the right iliac fossa. Blood investigations revealed a white cell count of 12.6×103/uL. Abdominal ultrasound was considered suspicious for appendicitis. The patient was operated for acute appendicitis. On macroscopic examination, the appendix had normal appearance. The appendiceal tissue was fixed in 10% buffered formalin and embedded in paraffin in a routine manner. The microscopic sections were stained hematoxylin and eosin. Histologically the tumor involved only the tip of the appendix. The surgical margin was intact. The appearance of the mucosa epithelium was normal. The tumor diameter was 0.8 cm and localized in the submucosa. The tumor showed widely dispersed, small round tubules composed of low columnar epithelial cells. Mitotic cells were not found (Figure 1). Immunohistochemical stains were positive for synaptophysin (Figure 2), neuron-specific enolase and pan-cytokeratin. Ki-67 proliferative index was 1%. The final diagnosis was tubular carcinoid of appendix based on the pathological finding. No recurrence was detected during clinical follow-up patient.
Discussion
In 1990, Burke et al. [3] reported 64 cases of carcinoid tumors with glandular features of the appendix. These lesions categorized into 3 groups: tubular carcinoids, goblet carcinoids, and mixed carcinoid adenocarcinomas. Tubular carcinoid is a rare variant of appendiceal well-differentiated neuroendocrine tumor. These lesions are usually no more than a few millimeters in size and are limited to the appendiceal tip. In our case, the tumor is localized in the appendiceal tip and 0.8 cm in diameter. The majority of patients present with acute appendicitis where the tubular carcinoid is discovered by coincidence in connection with surgery for acute appendicitis [2,4,5]. Our case presented with abdominal pain indicated the acute appendicitis. Tubular carcinoids were more common in young adults. These tumors are localized in the distal half of the appendix, with a low mitotic index [2-4]. The diagnosis is performed after careful histological-examination of an appendectomy specimen. Tubular carcinoids are diffusely infiltrative tumors and characterized by short lines of cells and small tubular structures and which are separated by abundant hyalinized and collagen-rich stroma. In most cases, the origin cell is the L-cell, which produces entero glucagons and peptide YY. Tumor cells often stain weakly and/or focally for neuroendocrine markers. Tubular carcinoids are stained with glucagon and chromogranin B by immunohistochemical staining [2,4,5]. The differential diagnosis of tubular carcinoid tumors includes well-differentiated adenocarcinomas. The neuroendocrine markers positivity rules out the adenocarcinoma [2,4]. In 1990, Matsukuma et al. [2] reported that Ki-67 expression in most cases was ≤2%. In our case, Ki-67 proliferative index was 1%. Treatment of tubular carcinoid tumor is based on surgery. Appendectomy for lesions less than 2 cm is sufficient. Appendiceal carcinoids larger than 2 cm require right-sided hemicolectomy and ileocecal lymphadenectomy [5]. Our case underwent appendectomy because of presented with acute apandicitis symptom. Appendicular carcinoid has the best prognosis due to its early discovery. No recurrence is detected in tumors smaller than 2 cm with simple appendectomy [4,5]. In the literature, tumor-related deaths or metastasis have not been reported.

Conclusion
Tubular carcinoid tumor of the appendix is a rare pathology, diagnosed usually after histopathological examination of the appendectomy specimen. In the literature, few cases have been reported. Tubular carcinoid should be made differential diagnosis from adenocarcinoma. Because, the prognosis and the treatment are very different. Therefore, the material should be examined carefully.
Declarations
Informed consent: Data was evaluated retrospectively after the required current treatment was completed, so the informed consent was not received.
Peer-review: Externally peer-reviewed.
Author contributions: The author contributed to all stages of the article.
Conflict of interest: No conflict of interest was declared by the author.
Financial disclosure: The author declared that this study has received no financial support.
References
- Chirilă DN, Pop TR, Turdeanu NA. Tubular carcinoid tumor of the appendix-a clinical case. Human & Veterinary Medicine. 2011; 3(1): 1-4.4.
- Matsukuma KE, Montgomery EA. Tubular carcinoids of the appendix: the CK7/CK20 immunophenotype can be a diagnostic pitfall. J Clin Patho. 2012; 65(7): 666-8.
- Burke AP, Sobin LH, Federspiel BH, Shekitka KM, Helwig EB. Goblet cell carcinoids and related tumors of the vermiform appendix.Am J Clin Pathol. 1990; 94(1): 27-35.
- Hwang J, Telem DA, Nguyen SQ, Suarez YN, Warner RR, et al. Tubular carcinoid tumor: A rare cause of appendicitis. Am Surg. 2009; 75(6): 518-9.
- Tang LH. Epithelial neoplasms of the appendix. Arch Pathol Lab Med. 2010; 134(11): 1612-20.