
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Short Report - Open Access, Volume 5
A rare case report: Meniere disease with bilateral internal acoustic canal osteomas
Fahad Al-Lhedan1*; Abdulrahman Al-Humaizi2
1Medical Imaging Department, Radiology and Nuclear Medicine Consultant, King Abdullah Bin Abdulaziz University Hospital, Riyadh, Saudi Arabia.
2Otolaryngology, Rhinology and Skull Base Consultant, ENT Department, King Abdullah Bin Abdulaziz University Hospital, Riyadh, Saudi Arabia.
*Corresponding Author : Fahad Al-Lhedan
Medical Imaging Department, Radiology and
Nuclear Medicine Consultant, King Abdullah Bin
Abdulaziz University Hospital, Riyadh, Saudi Arabia.
Email: fahad_allhedan@hotmail.com
Received : Nov 16, 2024
Accepted : Dec 02, 2024
Published : Dec 09, 2024
Archived : www.jcimcr.org
Copyright : © Al-Lhedan F (2024).
Abstract
Internal acoustic canal osteaomas are uncommon noncancerous bony growth and they have no aggressive behavior. Patient’s complaints secondary to these lesions are variable but usually related to balance problems and hearing issues [1]. Management should be tailored based on patient’s symptomatology [2-4]. This is a case of a patient who is known to have Meniere disease along with bilateral internal acoustic canal osteomas, as depicted on cross-sectional images, presenting with history of hearing loss, tinnitus and vertigo.
Citation: Al-Lhedan F, Al-Humaizi A. A rare case report: Meniere disease with bilateral internal acoustic canal osteomas. J Clin Images Med Case Rep. 2024; 5(12): 3377.
Introduction
Skull base osteaomas are rare osseous tumors but fortunately, they are benign and slowly growing masses [5,6]. CT scan is the gold standard imaging modality for diagnosing these lesions and MRI may play a role in confirming this possibility. Several differential considerations should be entertained prior to decision making. Medical treatment might be beneficial and surgical intervention can be offered whenever the former solution is not effective.
Case presentation
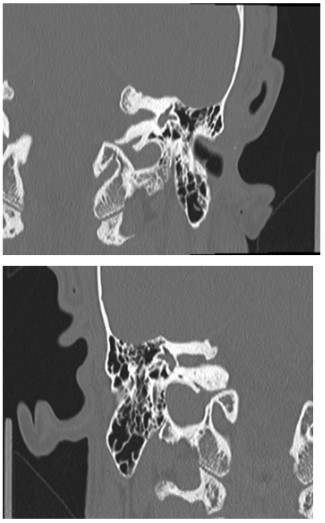
This is a 50-year-old gentleman who is known to have Meniere disease complaining of progressive hearing loss, ringing in ears and recurrent disabling attacks of vertigo with subsequent falling down and traumatic injuries that are affecting his life quality. Otoscope examination displays normal tympanic membranes. Temporal bones CT scan shows left vestibular aqueduct obliteration in addition to bilateral left larger than right internal acoustic canal osteomas. The patient was un cooperative and no further investigations were done. He was treated conservatively with anti-vertiginous therapy.
Discussion
Osteomas have unique imaging findings manifested by that they are usually solitary and pedunculated bony growths on CT scan and the presence of bone marrow is a diagnostic MR imaging feature. Under a microscope, these tumors are round to oval in shape consisting of compact bone that projects from the subperiosteal or endosteal surfaces of the cortex and they have a mature and well-differentiated bone tissue with a predominantly laminar structure traversed with Haversian canals and the latter is pathognomonic for osteoma [5,6]. Internal acoustic canal osteomas are not occurring very often and the probable differential diagnoses are exostosis, Paget’s disease, fibrous dysplasia, otosclerosis, congenital abnormalities, meningioma, schwannoma, heamangioma, lipoma and cholesteatoma [7]. The most frequent locations for osteomas are the external auditory canal, mastoid cortex and facial bones [8]. Patients with osteoma might be asymptomatic and the lesions are discovered incidentally or they may be suffering from aural fullness, tinnitus, vertigo or hearing loss [8,9]. Treatment of this bony abnormality remains controversial and serial imaging is advised whenever osteomas are silent. However, a trial with symptom-targeted medication should be given at the beginning and surgery could be considered only if there is no improvement. Of note that surgical resection is not always curative and results in milder symptoms therefore this must be explained to the patient [10].
Conclusion
In brief, osteoma is an unusual entity that is described scarcely in the literature. Consequently, the etiology, natural history and management of it is still debatable. CT scan has superior diagnostic performance with excellent accuracy in detecting osteomas. Therapeutic options are largely based on severity of symptoms. Follow up is advised for individuals with no clinical manifestations and conservative management in addition to surgical intervention are reserved for symptomatic patients.
Conflicts of interest: The authors declare that there are no conflicts of interest regarding publication of this paper.
References
- Maria K Brake, David P Morris, Jonathan Trites, S Mark Taylor, Rene G Van Wijhe, et al. A case of bilateral internal auditory canal osteomas, Ear Nose Throat J. 2014; 93(1): 15-8.
- Fred M Baik, Linda Nguyen, Joni K Doherty, Jeffrey P Harris, Mahmood F Mafee, et al. Comparative case series of exostoses and osteomas of the internal auditory canal, Ann Otol Rhinol Laryngol. 2011; 120(4): 255-60.
- Venelin M Gerganov, Amir Samii, Vincenzo Paterno, Alexandru C Stan, Madjid Samii. Bilateral osteomas arising from the internal auditory canal: Case report, Neurosurgery. 2008; 62(2): 528-9; 529.
- TC Davis, BA Thedinger, GM Greene. Osteomas of the internal auditory canal: A report of two cases, Am J Otol. 2000; 21(6): 852-6.
- JL Kemink, MD Graham. Osteomas and exostoses of the external auditory canal - medical and surgical management, J Otolaryngol. 1982; 11(2): 101-6.
- Sharon Ovnat Tamir, Francoise Cyna-Gorse, Olivier Sterkers. Internal auditory canal osteoma: Case report and review of the literature, Ear, Nose & Throat Journal. 2015; 94(6): 207-47.
- Jun Suzuki, Yusuke Takata, Hiromitsu Miyazaki, Izumi Yahata, Yasuhiko Tachibana, et al. Tetsuaki Kawase and Yukio Katori. Osteoma of the Internal Auditory Canal Mimicking Vestibular Schwannoma: Case Report and Review of 17 Recent Cases, Tohoku J. Exp. Med. 2014; 232: 63-68.
- B Liétin, A Bascoula, J Gabrillargues, S Crestani, P Avan, et al. Osteoma of the internal auditory canal, European Annals of Otorhinolaryngology, Head and Neck diseases. 2010; 127: 15-19.
- Vrabec JT, Lambert PR, Chaljub G. Osteoma of the internal auditory canal. Arch Otolaryngol Head Neck Surg. 2000; 126: 895-8.
- Moshin Khan, Michael Busby, Brent McMonagle. Exostosis of the internal auditory canal: A rare growth causing hearing loss, Otolaryngology Case Reports. 2023; 100527.