
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 5
Pregnancy in patient with Swyer syndrome: A case report
Nihar Ranjan Bhoi*; Vipin Chandra; Kritika Poddar
1Department of Reproductive Medicine, Head Research and Academics, Indira IVF Hospital Pvt Ltd, Udaipur, India.
2Department of Reproductive Medicine, Chief Clinical and Lab Operations, Indira IVF Hospital Pvt Ltd, Udaipur, India.
3Department of Reproductive Medicine, Indira IVF Hospital Pvt Ltd, Bikaner, India.
*Corresponding Author : Nihar Ranjan Bhoi
Department of Reproductive Medicine, Head
Research and Academics, Indira IVF Hospital Pvt
Ltd, Udaipur, India.
Email: drniharbhoi@gmail.com
Received : Nov 13, 2024
Accepted : Dec 03, 2024
Published : Dec 10, 2024
Archived : www.jcimcr.org
Copyright : © Bhoi NR (2024).
Abstract
Background: Swyer syndrome is a rare disorder of sexual development (DSD) characterized by a female phenotype, either normal or tall stature, bilateral gonadal dysgenesis, and primary amenorrhea. Given the risk of malignancy, gonadectomy is strongly recommended post-diagnosis. Pregnancy can be achieved through assisted reproduction technology.
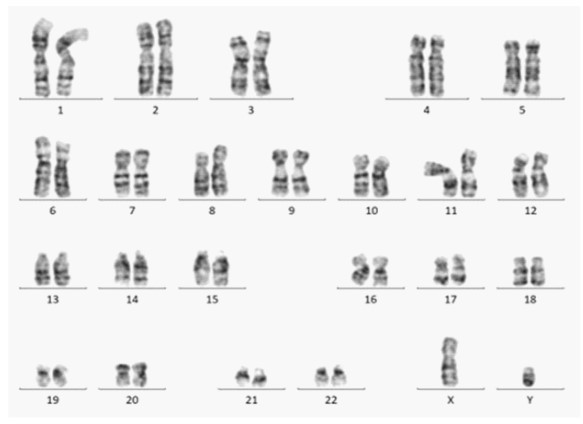
Case: A couple was evaluated for primary infertility. The wife presented with primary amenorrhea, poorly developed secondary sexual characteristics, bilateral streak gonads, and a small-sized uterus. Karyotype analysis revealed a 46 XY pattern, leading to a diagnosis of Swyer syndrome. Diagnostic laparoscopy indicated bilateral atrophic ovaries and a small-sized uterus. Gonadectomy was performed to mitigate future malignancy risk. Hormonal priming of the uterus induced normal menses. Utilizing oocyte donation, a successful pregnancy was achieved, resulting in the delivery of twins via cesarean section.
Conclusion: Disorders of sexual development pose significant challenges for assisted reproduction specialists, necessitating thorough examination and timely diagnosis. With appropriate fertility programs, including oocyte donation, individuals with 46, XY gonadal dysgenesis can achieve successful pregnancies. Despite a higher likelihood of cesarean delivery due to a poorly developed uterus, normal pregnancy and delivery are possible.
Keywords: Swyer syndrome; Karyotype; Oocyte donation; Embryo transfer.
Citation: Bhoi NR, Chandra V, Poddar K. Pregnancy in patient with Swyer syndrome: A case report. J Clin Images Med Case Rep. 2024; 5(12): 3380.
Introduction
Swyer syndrome, classified as a rare Disorder of Sexual Development (DSD), encompasses conditions where there are abnormalities in chromosomal, gonadal, or anatomical sex development [1,2]. This case is unique due to the rare and complex nature of true hermaphroditism, the late diagnosis, the reproductive challenges it presents, the need for extensive surgical interventions, and the broader societal and ethical implications associated with this condition. This condition is characterized by the non-development of sex glands. The National Organization for Rare Disorders (NORD) categorizes Swyer syndrome as 46 gonadal dysgenesis, which can manifest in complete or incomplete forms.
In fully expressed Swyer syndrome, individuals present with a female phenotype. They may exhibit normal or tall stature, bilateral gonadal dysgenesis, primary amenorrhea, and a eunuchoid habitus. Their outward appearance is entirely female, with the presence of fallopian tubes, a vagina, and various degrees of underdeveloped uterus, ranging from severe to mild hypoplasia [3,4]. Secondary sexual characteristics are typically not well-developed, and gonadectomy is strongly recommended following diagnosis due to the risk of malignancy. Achieving pregnancy is possible through In-Vitro Fertilization (IVF) using oocyte donation [5].
We report a case of Swyer syndrome in a 31-year-old female who had not previously been evaluated for primary amenorrhea until seeking consultation for primary infertility. Following a comprehensive battery of laboratory tests, physical examinations, and various radiological and surgical interventions, a diagnosis of a Disorder of Sex Development (DSD) was established. Through the utilization of IVF and oocyte donation, a successful twin pregnancy was achieved, culminating in the delivery of the babies via cesarean section [6].
Case history
A couple, comprising a 44-year-old husband and a 31-year- old wife, sought assistance at an infertility clinic after 13 years of marriage. The wife had experienced primary amenorrhea, prompting an investigation into the cause of their infertility.
The husband underwent blood tests, all of which returned within the normal range, and his sperm analysis showed normozoospermia according to the WHO 2021 reference range.
For the wife, a comprehensive gynecological evaluation was performed. Upon physical examination, it was noted that her secondary sexual characteristics were underdeveloped, and clitoromegaly (enlargement of the clitoris) was observed. Vaginal examination with one finger revealed a deep vaginal canal, and her cervix was palpable.
Laboratory reports indicated that her thyroid and prolactin values were within the normal range. However, her serum FSH (Follicle-Stimulating Hormone) levels were elevated at 50 mIU/ ml, while her serum LH (Luteinizing Hormone) levels were also elevated at 44 mIU/ml. The total testosterone level was notably low, measuring 0.18 ng/ml. A buccal smear test confirmed the presence of sex chromatin.
Ultrasound imaging (USG) revealed a hypoplastic uterus, measuring 28 mm by 8 mm, with a thin endometrial lining. Both ovaries appeared atrophic. An upper abdominal scan showed normal results.
Further investigation through laparoscopy revealed a rudimentary uterus, along with bilateral normal fallopian tubes. The left gonad appeared as a streak ovary, while the right gonad was situated in the inguinal canal and exhibited characteristics of a testis. Due to concerns about the potential risk of malignancy, bilateral gonadectomy (removal of gonads) with salpingectomy (removal of fallopian tubes) was performed.
In addition to these surgical procedures, excision of the phallus (penis-like structure) and clitoral reconstruction were carried out. Histopathological examination of the removed tissues confirmed the presence of ovarian stroma in the left gonad and testicular elements in the right gonad, leading to the diagnosis of true hermaphroditism. This rare condition involves the presence of both ovarian and testicular tissue in the same individual.
She was planned for IVF and ET with donor egg and husband’s sperm. Karyotype analysis was performed to check the chromosomal abnormalities which was normal (Figure 1). Considering the small size of uterus, uterus priming was done by Hormonal Replacement Therapy (HRT) with sequential exposure of Estradiol valerate (Abbott, India) for 25 days a month along with Dydrogestrone which was added in the last 10 days. She responded well to HRT and had regular cycles and therefore HRT was continued for 6 months. Repeat USG after 6 months showed uterus of size 6 cm x 4 cm x 3 cm and ET 7.5 cms. The vaginal canal was patent and endocervical canal was patent too as confirmed by a mock ET (embryo transfer), but the cervix was high and flushed with vagina.
Outcome and follow up: With egg donation programme 5 good quality blastocysts were formed. She was planning to receive elective SET (single embryo transfer), which resulted in a chemical pregnancy loss. Three months later she underwent a double embryo transfer (4AA and 5AB grade as per Gardner’s grading) [7], which resulted in twin pregnancy. With uterine muscle strength in suspicion, an abdominal cerclage was planned as cervix was high. She tolerated the procedure well. The antenatal period was uneventful. Owing to Doppler changes, which suggested compromised blood flow at 34 weeks, LSCS was planned and one healthy male and a female baby were delivered. The babies were 1.9 and 2 kgs respectively and kept in NICU for 5 days before shifting to mother side. The post-op period was uneventful and there was no major neonatal complication except physiological jaundice which was recovered with phototherapy. Both the babies are doing well now.
Discussion
Swyer syndrome, initially documented by Dr. Swyer, is a condition typically characterized by primary amenorrhea, with the external genitalia and vagina appearing anatomically normal [8,9]. Individuals with Swyer syndrome often present a unique set of physical traits, including a tall stature, underdeveloped breasts, normal pubic and axillary hair growth, a typical vagina and cervix, a small uterus, and a noticeable absence of palpable adnexal structures. Intriguingly, their uterus and gonads are hypoplastic, positioned in the location typically occupied by ovaries. This condition highlights a profound discordance between the genetic makeup and outward appearance, emphasizing the complexity of Swyer syndrome [10-12].
In this report, we present an exceptional case of Swyer syndrome involving a 31-year-old female who had not undergone prior evaluation for primary amenorrhea until seeking medical advice due to primary infertility. The diagnostic journey encompassed an extensive array of laboratory tests, physical examinations, radiological assessments, and surgical interventions. Ultimately, the diagnosis of a Disorder of Sex Development (DSD) was established. Remarkably, this patient achieved a successful twin pregnancy through the use of assisted reproductive technology, specifically In-Vitro Fertilization (IVF) and oocyte donation. The twins were delivered via cesarean section, marking a significant milestone in the context of Swyer syndrome.
Swyer syndrome presents a unique scenario where the phenotype aligns with female characteristics, while the genotype remains male [13]. Typically, individuals receive a diagnosis between the ages of 18 to 23 years, with primary amenorrhea being the predominant initial. Notably, individuals with Swyer syndrome face an elevated risk of developing tumors within their underdeveloped gonadal tissue, a risk that can manifest at any age, even in childhood, prior to the suspicion of Swyer syndrome [8,14,15]. Approximately 30% of women with Swyer syndrome develop tumors originating from the cells responsible for forming the testes or ovaries, known as gonadal tumors [16-18]. Among these tumors, the most prevalent type is the gonadoblastoma, which is a non-cancerous tumor unique to individuals with compromised gonadal development [19,20]. It is crucial to note that gonadoblastomas can potentially transition into malignant tumors, such as dysgerminoma, which demonstrates a higher incidence in women with Swyer syndrome compared to the general population [21]. Hence, the recommended course of action involves the prophylactic removal of dysgenetic gonads to mitigate this risk effectively. Furthermore, there are additional risks associated with gonadal dysgenesis, including extended periods of hypoestrogenemia, which can lead to conditions like osteoporosis and virilization. Addressing these risks necessitates Hormone Replacement Therapy (HRT). HRT plays a pivotal role in facilitating breast development, maintaining regular menstrual cycles, and preventing further uterine hypoplasia [22]. Consequently, HRT empowers women with Swyer syndrome to carry a pregnancy to full.
The presence of the XY genotype and H-Y antigen does not hinder the normal uterine and endometrial response, affirming the innate capacity of the uterus to support a successful pregnancy and delivery in individuals with XY dysgenesis [23,24].It is essential to acknowledge that the number of reported live births in patients with Swyer syndrome is exceptionally limited, with fewer than 13 cases documented in the existing literature. This underscores the urgent need for comprehensive reporting on pregnancies and outcomes within this rare and distinct patient population.
In cases akin to the one presented here, most reported pregnancies in individuals with Swyer syndrome were delivered via cesarean section, often for various reasons [25]. These reasons include concerns related to fetal positioning, pelvic structure influenced by androgenic factors, and the presence of a hypoplastic uterus [26,27]. There is also a possibility that caesarean deliveries occurred without strict obstetric indications, potentially due to the exceptional rarity of this condition and concerns shared by both patients and healthcare providers [28,29].
Conclusion
To summarize, Swyer syndrome offers a captivating and intricate interplay between genetics and physical appearance, presenting unique challenges and opportunities for individuals living with this condition. This case report highlights the potential for successful pregnancies in individuals with Swyer syndrome and underscores the importance of comprehensive care and thorough reporting to advance our understanding of this rare and intriguing medical phenomenon.
References
- Kan A, Abdalla H, Oskarsson T. Two successful pregnancies in a 46, XY patient. Human reproduction [Internet]. 1997; 12 7: 1434-5.
- Chen MJ, Yang JH, Mao T, Ho H, Yang Y. Successful pregnancy in a gonadectomized woman with 46, XY gonadal dysgenesis and gonadoblastoma. Fertil Steril [Internet]. 2005; 84 1: 217.
- Prokselj K, Štalc M, Stritar BŠ, Mohorko-Pleskovič P, Kozak M. Pregnancy in a patient with a bioprosthetic tricuspid valve. J Obstet Gynaecol (Lahore) [Internet]. 2013; 33: 736-736.
- Urban A, Knap-Wielgus W, Grymowicz M, Smolarczyk R. Two successful pregnancies after in vitro fertilisation with oocyte donation in a patient with Swyer syndrome - a case report. Prz Menopauzalny [Internet]. 2021; 20: 158-61.
- Swyer Syndrome in a Woman with Pure 46, XY Gonadal Dysgenesis, A Rare Disorder, Late Presentation: Case Report. 2017.
- Koi C, Kurita T, Sho T, Aramaki S, Inagaki H, Shibata E, et al. Three Cases of Disorders of Sex Development Treated by Laparoscopic Gonadectomy. Japanese Journal of Gynecologic and Obstetric Endoscopy [Internet]. 2013; 29: 508-13.
- Balaban B, Brison D, Calderón G, Catt J, Conaghan J, Cowan L, et al. The Istanbul consensus workshop on embryo assessment: Proceedings of an expert meeting. In: Human Reproduction. Oxford University Press. 2011; 1270-83.
- Sauer M, Lobo R, Paulson R. Successful twin pregnancy after embryo donation to a patient with XY gonadal dysgenesis. Am J Obstet Gynecol [Internet]. 1989; 161(2): 380-1.
- Frydman R, Parneix I, Fries N, Testart J, Raymond J, Bouchard P. Pregnancy in a 46, XY patient. Fertil Steril [Internet]. 1988; 50(5): 813-4.
- Kalra A, Nadkarni P, Singh P, Nadkarni A. Successful pregnancy outcome in a case of Swyer Syndrome with hypertension and morbid obesity. Int J Reprod Contracept Obstet Gynecol [Internet]. 2016; 5: 2061-4.
- Selvaraj K, Ganesh V, Selvaraj P. Successful pregnancy in a patient with a 46, XY karyotype. Fertil Steril [Internet]. 2002; 78(2): 419-20.
- Prokselj K, Štalc M, Stritar BŠ, Mohorko-Pleskovič P, Kozak M. Pregnancy in a patient with a bioprosthetic tricuspid valve. J Obstet Gynaecol (Lahore) [Internet]. 2013; 33: 736-736.
- Çatlı G, Alparslan C, Can PS, Akbay S, Kelekci S, Atik T, et al. An Unusual Presentation of 46, XY Pure Gonadal Dysgenesis: Spontaneous Breast Development and Menstruation. J Clin Res Pediatr Endocrinol [Internet]. 2015; 7: 159-62.
- Foyouzi N. Fertility in Disorders of Sex Development: Evidence and Uncertainties. Reproductive Medicine, Gynecology & Obstetrics [Internet]. 2019; null: null.
- Karimian N, Ghadakzadeh S, Eshraghi M. Swyer syndrome in a woman with pure 46, XY gonadal dysgenesis and a hypoplasticuterus: a rare presentation. Fertil Steril [Internet]. 2010; 93(1): 267.e13-4.
- Rasouli MA, McDaniel KE, Awadalla M, Chung K. Mosaic Turner Syndrome Presenting with a 46, XY Karyotype. Case Rep Obstet Gynecol [Internet]. 2019; 2019: null.
- Ko PC, Peng H, Soong Y, Chang S. Triplet pregnancy complicated with one hydatidiform mole and preeclampsia in a 46, XY female with gonadal dysgenesis. Taiwan J Obstet Gynecol [Internet]. 2007; 46(3): 276-80.
- Bianco S, Agrifoglio V, Mannino F, Cefalù E, Cittadini E. Successful pregnancy in a pure gonadal dysgenesis with karyotype 46, XY patient (Swyer’s syndrome) following oocyte donation and hormonal treatment. Acta Eur Fertil [Internet]. 1992; 23(1): 37-8.
- Nadkarni K. Successful Conception and Delivery in an Unusual Case of 46, XY Pure Gonadal Dysgenesis with Spontaneous Breast Development, Menses, and Bilateral Hydrosalpinx. International Journal of Infertility and Fetal Medicine [Internet]. 2016; 7: 58-60.
- Dirnfeld M, Bider D, Abramovicia H, Calderon I, Blumenfeld Z. Subsequent successful pregnancy and delivery after intracytoplasmic sperm injection in a patient with XY gonadal dysgenesisms. Eur J Obstet Gynecol Reprod Biol [Internet]. 2000; 88(1): 101-2.
- Amin S, Kumaran A. Dysgerminoma presenting at fifty, consequence to undiagnosed Swyer syndrome. Int J Reprod Contracept Obstet Gynecol [Internet]. 2021.
- Sancar C, Yildirim N, Mammadova S, Ergenoğlu A, Karadadaş N. 46, XY Gonadal Dysgenesis (Swyer Syndrome): A Case Report with Late Diagnosis. 2018.
- Murtinger M, Hradecký L, Spitzer D, Zech N. Unexpected labor and successful twin birth to a pure gonadal dysgenetic woman. Arch Gynecol Obstet [Internet]. 2013; 288: 1425-6.
- Michala L, Goswami D, Creighton S, Conway G. Swyer syndrome: presentation and outcomes. BJOG [Internet]. 2008; 115: null.
- Santis M De, Spagnuolo T, Barone D, Licameli A. Successful twin pregnancy in a 46, XY pure gonadal dysgenesis. J Obstet Gynaecol (Lahore) [Internet]. 2013; 33: 737-8.
- Milewicz T, Mrozinska S, Szczepański W, Białas M, Kiałka M, Doroszewska K, et al. Dysgerminoma and gonadoblastoma in the course of Swyer syndrome. Pol J Pathol [Internet]. 2016; 67(4): 411-4.
- Siddique H, Daggett P, Artley K. Successful term vaginal delivery in a 46, XY woman. International Journal of Gynecology & Obstetrics [Internet]. 2008; 101: null.
- Gezer C, Ekin A, Sahingoz AG, Solmaz U, Karadeniz T, Sayhan S, et al. Pregnancy outcome of a case with Swyer syndrome after bilateral gonadectomy and adjuvant chemotherapy. Medical Science and Discovery [Internet]. 2016; 3: 280.
- Plante BJ, Fritz M. A case report of successful pregnancy in a patient with pure 46, XY gonadal dysgenesis. Fertil Steril [Internet]. 2008; 90(5): 2015. e1-2.