
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Clinical Image - Open Access, Volume 5
Diaphragmatic fistula caused by subhepatic collection
Pau Cruzado-Boix*; Domingo Madera Hernández; Marta Plana Pes
Respiratory Department, Bellvitge University Hospital, Bellvitge Biomedical Research Institute (IDIBELL), The Hospital of Llobregat, Barcelona, Spain.
*Corresponding Author : Pau Cruzado-Boix
Respiratory Department, Bellvitge University
Hospital, Bellvitge Biomedical Research Institute
(IDIBELL), The Hospital of Llobregat, Barcelona,
Spain.
Tel: 93-260-7689;
Email: pcruzado@bellvitgehospital.cat
Received : Nov 15, 2024
Accepted : Dec 04, 2024
Published : Dec 11, 2024
Archived : www.jcimcr.org
Copyright : © Cruzado-Boix P (2024).
Keywords: Pleural infections; Thoracic ultrasonography; Diaphragmatic fistula.
Citation: Cruzado-Boix P, Hernández DM, Pes MP. Diaphragmatic fistula caused by subhepatic collection. J Clin Images Med Case Rep. 2024; 5(12): 3381.
Introduction
Diaphragmatic fistula is a rare complication of intra-abdominal infections, such as subhepatic abscesses, often resulting in significant morbidity. Timely diagnosis and management are crucial, to prevent the development of empyema or other serious complications.
Case presentation
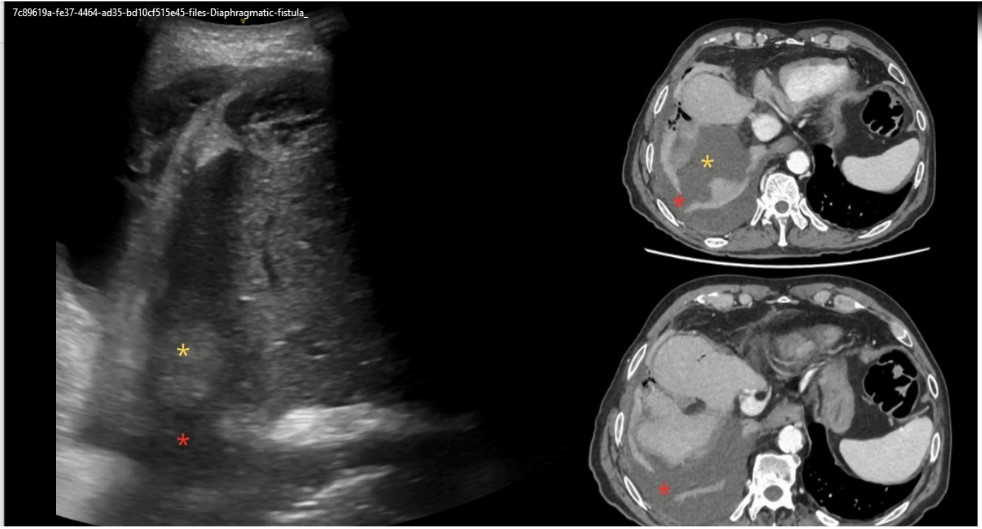
We present the case of a 76-year-old male with a history of abdominal surgery 11 months prior, complicated by a subhepatic abscess requiring percutaneous drainage and intravenous antibiotic therapy. One month after discharge, the patient developed right upper quadrant pain, dyspnea, and cough. On examination, reduced breath sounds were noted at the right lung base. A lung ultrasound revealed pleural effusion with features suggestive of empyema, a persistent subhepatic collection, and a possible diaphragmatic ruptura (Figure 1). Thoracocentesis yielded purulent fluid, confirming empyema. Computed Tomography (CT) of the thorax confirmed the presence of a diaphragmatic fistula connecting the pleural and peritoneal spaces. Treatment included pleural drainage, intrapleural urokinase, and intravenous antibiotics. The diaphragmatic fistula was managed conservatively, without the need for surgical intervention. Follow-up imaging demonstrated complete resolution of the fistula, with no empyema recurrence.
Discussion
Diaphragmatic fistula resulting from subhepatic abscesses is a rare complication, likely underdiagnosed due to its nonspecific presentation. Diagnosis is primarily achieved via CT imaging. However the use of ultrasonography in some cases may be useful. Management strategies depend on the severity and patient’s overall condition, with conservative treatment being successful in some cases, while others may necessitate surgical repair [1].
Conclusion
This case highlights the importance of considering diaphragmatic fistula as a differential diagnosis in patients with intra-abdominal abscesses and respiratory symptoms. Thoracic ultrasonography can be useful to detect this complication in order to establish the diagnosis and management in a timely manner.
Declarations
Funding sources: None.
Conflicts of interest: The authors have no conflict of interest to declare.
Informed consent: Written informed consent was obtained for the publication of the article.
References
- Ikeda M, Hatakeyama Y, Murakami S, Hashimoto R, Tauchi S, Yonekura Y, Ohnishi H. Surgical repair of hepatic hydrothorax caused by diaphragmatic fistula. Respir Med Case Rep. 2020; 32: 101325. doi: 10.1016/j.rmcr.2020.101325.