
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 5
Breus mole: A rare case of pregnancy complicated by massive subchorionic thrombohematoma
Shafaq Fatima*; Irum Sohail; Mahjabeen; Marium Riaz; Mahrukh Fatima Zaidi
KRL Hospital, Islamabad, Pakistan.
*Corresponding Author : Shafaq Fatima
KRL Hospital, Islamabad, Pakistan.
Email: shafaqfatima968@gmail.com
Received : Nov 15, 2024
Accepted : Dec 04, 2024
Published : Dec 11, 2024
Archived : www.jcimcr.org
Copyright : © Fatima S (2024).
Abstract
We present a case report of a fourth gravida, severely anemic at 22 weeks of gestation with large placental mass disproportionate of her gestational age misdiagnosed as partial placental abruption. A degenerating fibroid was also considered in the differential diagnosis. Moreover, severe oligohydramnios was there. Based on its strange appearance, severely compromised fetus and radiological evidence it was decided to do a hysterotomy which revealed a large Intra placental hemorrhage and alive fetus. The retrospective diagnosis based on clinical radiological and histopathological findings came out to be a rare condition i.e. a brews mole (Massive subchorionic thrombohematoma).
Keywords: Subchorionic hematoma; Intra placental hemorrhage; Hysterotomy.
Citation: Fatima S, Sohail I, Mahjabeen, Riaz M, Zaidi MF. Breus mole: A rare case of pregnancy complicated by massive subchorionic thrombohematoma. J Clin Images Med Case Rep. 2024; 5(12): 3382.
Introduction
Massive Subchorionic Thrombohematoma (MST) is a rare disorder characterized by a substantial maternal blood clot that detaches the chorionic plate from villous chorion, this condition was initially identified and named as Breus mole in 1892 [1]. The incidence of MST is very rare i.e. 0.03-0.08%, hence its etiology and pathogenesis are still unknown [2]. The high incidence of complications associated with this condition such as early preterm birth, severe fetal growth restriction, intrauterine fetal demise requires a careful perinatal management [1]. Ultrasound [3] and MRI are useful tools for the diagnosis of Breus mole prenatally [4].
Case report
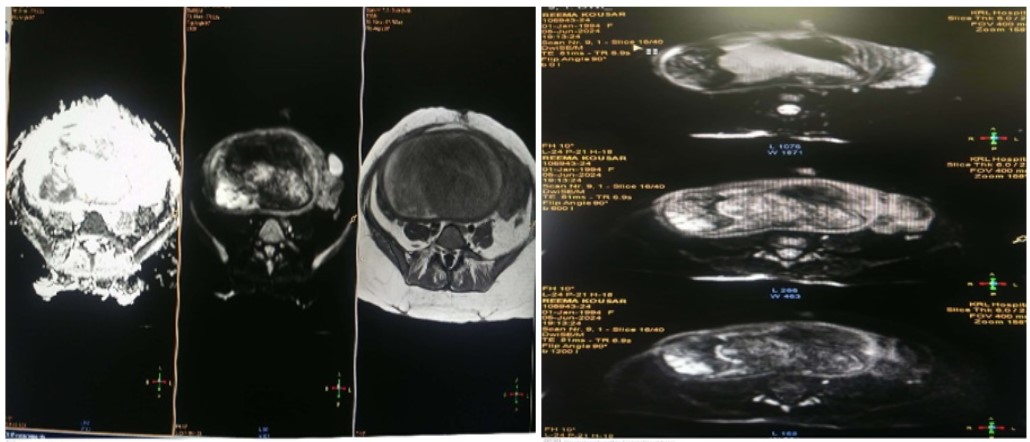
A self-referral case of Thirty 33 years old female G4P3+0 presented first time in OPD at 22 weeks of gestation with complaint of abdominal protuberance disproportionate of her gestational age. She has been in a consanguineous marriage for last 10 years, the obstetric history found to be having previously 3 alive healthy babies delivered through cesarean section with no significant antenatal, intrapartum and postpartum complications, last child born was 4 years back. She has insignificant past medical and family history. In this pregnancy, there was only one antenatal visit at some private hospital in 2nd trimester at 17 weeks of gestation, in which she was found to have severe anemia with hemoglobin level of 7 g/dL and a large placental mass on ultrasonography with a differential diagnosis that includes retroplacental hematoma and degenerating fibroid. She had 1 packed red cells transfusion over there. On General physical examination, there was significant Pallor. On Abdominal examination: soft, non-tender abdomen with Symphysio fundal height corresponds to 32 weeks of gestation, exact lie and position of fetus could not be assessed, fetal heart sounds were positive below umbilicus. There was no evidence of vaginal bleeding. She was admitted and her investigations sent. In Laboratory investigations Blood CP showed a hemoglobin level of 7.4 g/dL, TLC count of 8000/cumm, platelet count of 230x109. Coagulation profile, renal function tests, liver function tests were also within normal range. In Radiological investigations, an ultrasound for fetal well being showed a large retroplacental hematoma and alive fetus of 19 weeks, severe oligohydramnios with liquor volume of 1 cm and no gross anomaly seen. Her hemoglobin levels were built up by 2 packed red cells transfusions. MRI pelvis was done which revealed a large retroplacental hematoma of 1600 ml (14.6x11.7x19.8 cm) with contrast extravasation and pooling of contrast on delayed images-sequel of partial placental abruption.
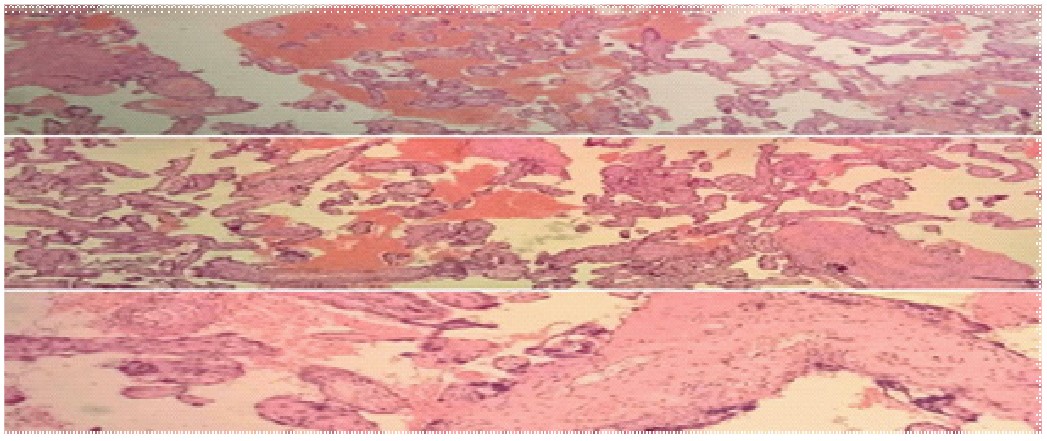
Placenta was sent for histopathological examination which showed a placental weight 443 grams more than expected weight with hypoxia associated changes in it, Placental membranes showed acute amniotic fluid infection.

Discussion
The term Breus’ “Mole” does not actually mean molar degeneration as seen in hydatidiform moles but is related to “mass” or coagulated blood, that progressively increases with gestational age. Although its reported frequency is very low, some predisposing factors are circulatory disorders, monosomies, hypertension and diabetes. The study conducted by Baxi and Pearlstone [6] suggested that antibodies are an etiological factor for subchorionic hematoma. However, we did not find any predisposing factor in our patient. The investigated cases have been associated with IUGR, which is due to uteroplacental insufficiency [5] and having poor pregnancy outcomes. These findings were present in our patient as well. Case reported in literature by Miyagi M, et al. had still birth at 22 weeks with this specific condition. Fung et al. reported that only 6 of 10 pregnancies with MST resulted in a live birth, only 2 of which reached full term.
Literature showed the significance of prenatal diagnosis of Breus mole with ultrasound and MRI. In one of the case reports from Washington [3] diagnosis of MST was made at 22 weeks with ultrasound and MRI, pregnancy continued with closed surveillance. Emergency cesarean section was performed at 34 weeks of gestation because of Non reassuring fetal status, an alive healthy baby boy of 1.2 kg delivered with good APGAR score. In our case ultrasound revealed placentomegaly, FGR, and severe oligohydramnios. However, prenatal diagnosis of MST could not be done. As MRI found a huge abnormal signal intensity of 1600 ml in retroplacental area and on post contrast sequence, contrast extravasated into the heterogenous area hence diagnosis of partial placental abruption was made which was not proven in retrospective diagnosis of the case. Although this condition is quite rare, it should still be included in the differential diagnosis, perhaps as a last consideration, when a patient presents with these clinical features.
References
- Miyagi M, Kinjo T, Mekaru K, Nitta H, Masamoto H, et al. Massive subchorionic thrombohematoma (Breus’ Mole) associated with fetal growth restriction, oligohydramnios, and intrauterine fetal death. Case Reports in Obstetrics and Gynecology. 2019; 2019(1): 9510936.
- Fung TY, To KF, Sahota DS, Chan LW, Leung TY, et al. Massive sub-chorionic thrombohematoma: A series of 10 cases. Acta obstetricia et gynecologica Scandinavica. 2010; 89(10): 1357-61.
- Kobayashi Y, Hasegawa A, Samura O, Okamoto A. Managing a case of Breus’ mole with severe fetal growth restriction via sequential ultrasonographic imaging and MRI. Radiology Case Reports. 2023; 18(12): 4474-8.
- Nishijima K, Shukunami KI, Tsuyoshi H, Orisaka M, Tajima K, et al. Massive subchorionic hematoma: peculiar prenatal images and review of the literature. Fetal diagnosis and therapy. 2005; 20(1): 23-6.
- El-Agwany AS. Large subchorionic hematoma: Breus’ mole. Journal of medical ultrasound. 2017; 25(4): 248-50.
- Baxi LV, Pearlstone MM. Subchorionic hematomas and the presence of autoantibodies. American Journal of Obstetrics & Gynecology. 1991; 165(5): 1423-4.