Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 5
Bilateral necrotizing pneumonia: A fulminant evolution
Passos R1,2*; Alves D1; Martins JD2,3; Corga R1,2
1Critical Care Department, Hospital de Santa Luzia, Viana Do Castelo, Portugal.
2School of Medicine, University of Minho, Braga, Portugal.
3Internal Medicine Department, Hospital de Santa Luzia, Viana do Castelo, Portugal.
*Corresponding Author : Rita Passos
Santa Luzia Hospital, Estrada de Santa Luzia, 50,
4900-855 Viana do Castelo, Portugal.
Email: ritamsmp@gmail.com
Received : Nov 19, 2024
Accepted : Dec 05, 2024
Published : Dec 12, 2024
Archived : www.jcimcr.org
Copyright : © Passos R (2024).
Citation: Passos R, Alves D, Martins JD, Corga R. Bilateral necrotizing pneumonia: A fulminant evolution. J Clin Images Med Case Rep. 2024; 5(12): 3383.
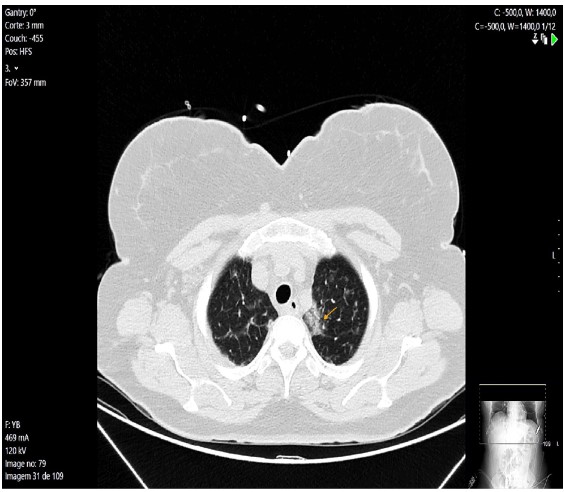
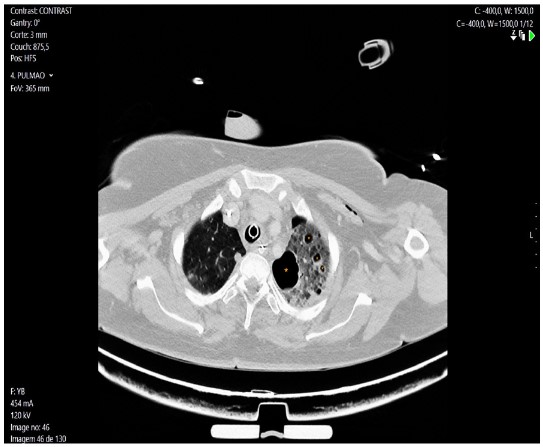
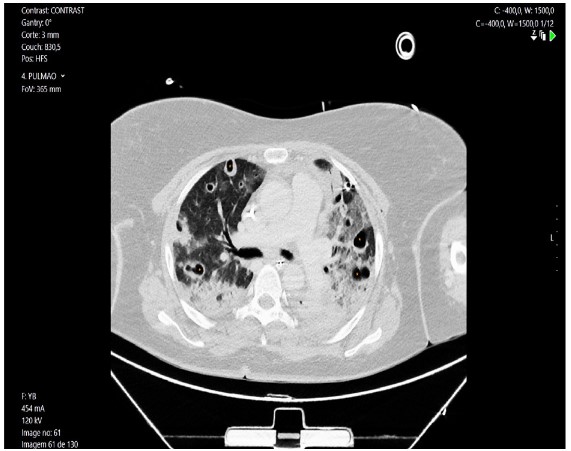
Description
A 47-year-old female patient, elderly caregiver, with no previous medical history was admitted at ICU with hypoxemic acute respiratory failure in the context of bilateral pneumonia, with an arterial blood gas at admission revealing a paO2 52 mmHg (reference value >60 mmHg) and paCO2 32 mmHg (reference value 35-45 mmHg) in FiO2 of 60% by venturi mask. The admission chest CT scan is represented in (Figure 1). At admission she was started on invasive mechanical ventilation and empirical antimicrobial therapy was started, adjusted at day two to vancomycin after identification of methicillin-resistant Staphylococcus aureus on blood cultures. Severe hypoxemia persisted besides curarization and prone position sessions, so CT scan was repeated at day six revealing a diffuse necrotizing pneumoniae (Figures 2 and 3). The patient was started on Veno-venous extracorporeal membrane oxygenation and transferred to a tertiary hospital.