
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Short Report - Open Access, Volume 5
A rare case of PDGFRA p.K385‐mutant myxoid glioneuronal tumor localized to the right frontal lobe
Grace E Hey, BS1*; Megan EH Still, MD2; Rachel SF Moor, MD2; Tara C Massini, MD3; Anthony T Yachnis, MD4; Duane Mitchell, PhD5; Ashley P Ghiaseddin, MD2
1University of Florida College of Medicine, Gainesville, FL, USA.
2Lillian S. Wells Department of Neurosurgery, University of Florida College of Medicine, Gainesville, FL, USA.
3Neuroradiology, Department of Radiology, University of Florida College of Medicine, Gainesville, FL, USA.
4Department of Pathology, Immunology, and Laboratory Medicine, University of Florida, Gainesville, FL, USA.
5Lillian S. Wells Department of Neurosurgery, Preston A. Wells Jr. Center for Brain Tumor Therapy, UF Clinical and Translational Science Institute, University of Florida, Gainesville, FL, USA.
*Corresponding Author : Grace E Hey
University of Florida College of Medicine,
Gainesville, Florida, USA.
Email: gracehey@ufl.edu
Received : Nov 20, 2024
Accepted : Dec 09, 2024
Published : Dec 16, 2024
Archived : www.jcimcr.org
Copyright : © Hey GE (2024).
Abstract
Myxoid Glioneuronal Tumor (MGNT) is a newly described tumor with a prominent PDGFRA p.K385 mutation typically located in the septum pellucidum or periventricular white matter of the lateral ventricle. Presently, there are less than 100 observations of MGNT in the current body of literature. We present the first case of PDGFRA p.K385‐mutant MGNT localized to the right frontal lobe.
Citation: Hey GE, Still MEH, Moor RSF, Massini TC, Yachnis AT, et al. A rare case of PDGFRA p.K385‐mutant myxoid glioneuronal tumor localized to the right frontal lobe. J Clin Images Med Case Rep. 2024; 5(12): 3387.
Introduction
Myxoid Glioneuronal Tumor (MGNT) is a central nervous system neoplasm characterized by a p.K385 mutation involving leucine or isoleucine replacing lysine at codon 385 of the Platelet‐Derived Growth Factor Receptor α (PDGFRA) gene, with a characteristic location in the septum pellucidum, corpus callosum, or periventricular white matter. Originally reported in 2018, MGNT has since been recognized as a novel tumor in the 2021 World Health Organization (WHO) Classification of Tumors in the Central Nervous System [1-3]. MGNT is histologically similar to the dysembryoplastic neuroepithelial tumor or rosetteforming glioneuronal tumor, having oligodendrocyte-like tumor cells embedded in a myxoid stroma [4,5]. Patients are typically treated with gross tumor resection followed by observation, and some have been treated with surgery followed by laser interstitial thermal therapy or external beam radiation [1‐5]. Though typically located in the septum pellucidum, individual cases have reported localized to the corpus callosum, midbrain tectum, and temporal lobe [1]. Herein we report the first case of MGNT localized to the right frontal lobe [1,2,6,7].
Case presentation
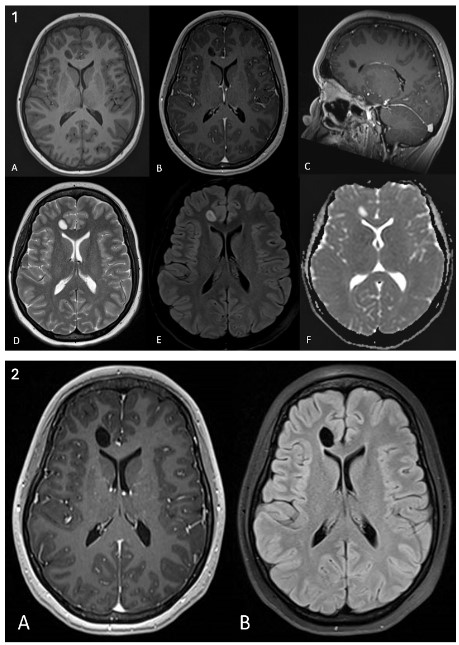
A 19‐year‐old female with a significant past medical history of migraines and endometriosis presented to our neuro-oncology clinic in January 2024 with complaints of persistent headaches. The patient had been experiencing severe headaches for more than 5 years with no relief with trials of several migraine medications. In April 2022, she was involved in a motor vehicle accident, prompting MRI imaging that revealed a nonspecific ovoid circumscribed FLAIR hyperintense lesion in the right anterior frontal lobe, measuring 0.1x0.8x0.6 cm in size, with no enhancement, diffusion restriction, adjacent cerebral edema, midline shift, or mass effect (Figure 1.1). She underwent surgical resection of this lesion in November 2023. 5‐month post‐operative MRI revealed gross total resection with regional encephalomalacia (Figure 1.2).
Limited tissue was received for pathological evaluation with focal neoplastic‐appearing cells identified mostly on the frozen section material. Classic oligodendrocyte‐like cells within a myxoid background were not apparent. Low proliferation was suggested by Ki67 immunolabeling. No mutations were identified by immunohistochemistry for IDH1 R132H, ATRX, or BRAF V600E. Molecular analysis revealed a PDGFRA p.K385L mutation. The tumor was signed out as a “low grade glial/glioneuronal tumor with PDGFRA p.K385L mutation. The latter mutation is characteristic of the “myxoid glioneuronal tumor.” Follow‐up MRI in December 2023 demonstrated expected postsurgical changes of gross total resection with no residual FLAIR signal changes or hypervascularity at 4 months postoperative.
Discussion
MGNT is a newly described tumor with few reported cases in the literature. Despite not having classic histology, the identification of a PDGFRA p.K385L mutation by molecular testing strongly suggests a myxoid glioneuronal tumor, which is the only glioneuronal tumor with this mutation. It was localized to the right frontal lobe.8 unique challenges in terms of presenting symptoms, surgical approach, and potential complications. While most tumors of the septum pellucidum present with obstructive hydrocephalus, this patient had been experiencing chronic headaches which may have been previously misdiagnosed and mistreated as headaches. The potential for cortical locations of MGNT brings to mind the possibility of a variety of presentations not currently associated with the tumor and may require future review of the 2021 WHO classification requirements. This case ultimately provides valuable insight to better understanding the clinical behavior and management of this novel tumor. Consistent with other reports, our patient’s MGNT was slow‐growing and gross total resection was achieved with no acute complications [1]. However, the lack of classic oligodendrocyte‐like cells within a myxoid background in our patient highlights the importance of correlating pathological findings with neuroimaging and molecular genotyping. Given the unique nature and presentation of this novel tumor in our patient, future research should be conducted to better understand the underlying pathophysiology of PDGFRA p.K385-mutant MGNT and any differences in symptomatology or clinical management to optimize therapeutics. Additional cases of PDGFRA p.K385‐ mutant MGNT found in novel brain regions should be reported.
References
- Lucas CG, Villanueva-Meyer JE, Whipple N, et al. Myxoid glioneuronal tumor, PDGFRA p.K385-mutant: clinical, radiologic, and histopathologic features. Brain Pathol. May 2020; 30(3): 479-494. doi:10.1111/bpa.12797.
- Gilani A, Siddiq Z, Kleinschmidt-DeMasters BK. Temporal lobe myxoid glioneuronal tumor, PDGFRA p.K385L-mutant with DNA methylation confirmation. Brain Pathol. Sep 2022; 32(5): 13079. doi:10.1111/bpa.13079.
- Bale TA, Rosenblum MK. The 2021 WHO Classification of Tumors of the Central Nervous System: An update on pediatric low-grade gliomas and glioneuronal tumors. Brain Pathol. 2022; 32(4): 13060. doi:10.1111/bpa.13060.
- Solomon DA, Korshunov A, Sill M, et al. Myxoid glioneuronal tumor of the septum pellucidum and lateral ventricle is defined by a recurrent PDGFRA p.K385 mutation and DNT‐like methylation profile. Acta Neuropathol. 2018; 136(2): 339‐343. doi:10.1007/ s00401-018-1883-2.
- Louis DN, Perry A, Wesseling P, et al. The 2021 WHO Classification of Tumors of the Central Nervous System: a summary. Neuro Oncol. 2021; 23(8): 1231-1251. doi:10.1093/neuonc/ noab106.
- Kleinschmidt-DeMasters BK, Chiang J, Donson AM, Borges T, Gilani A. Myxoid glioneuronal tumor, PDGFRA p.K385L-mutant, arising in midbrain tectum with multifocal CSF dissemination. Brain Pathol. 2022; 32(1): 13008. doi:10.1111/bpa.13008.
- Caporalini C, Scagnet M, Giunti L, et al. Myxoid glioneuronal tumor: Histopathologic, neuroradiologic, and molecular features in a single center series. Neoplasia. 2023; 37: 100885.
- doi:10.1016/j.neo.2023.100885.
- Chu J, Hu S, Wang G, Hu J, Xiao W. One case of myxoid glioneuronal tumour in the left frontal lobe. BJR Case Rep. 2024; 10(3): 014. doi:10.1093/bjrcr/uaae014.