
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 5
Unusual presentation of systemic drug-related intertriginous and flexural exanthema (SDRIFE) in children potentially caused by cisplatin and doxorubicin: A case report
Patawee Na Bangxang*; Rattanavalai Nitiyarom; Wanee Wisuthsarewong; Narin Banomyong
Division of Dermatology, Department of Pediatrics, Faculty of Medicine, Siriraj Hospital, Mahidol University, Thailand.
*Corresponding Author : Patawee Na Bangxang
Division of Dermatology, Department of Pediatrics,
Faculty of Medicine, Siriraj Hospital, Mahidol
University, Thailand.
Tel: (+66) 65-526-3628, (+66) 2-419-5678;
Email: pxang119@gmail.com
Received : Nov 20, 2024
Accepted : Dec 09, 2024
Published : Dec 16, 2024
Archived : www.jcimcr.org
Copyright : © Bangxang PN (2024).
Abstract
Systemic Drug-Related Intertriginous and Flexural Exanthema (SDRIFE) is a rare cutaneous manifestation of systemic contact dermatitis caused by drugs both in children and adults. We report a case of an 8-year-old girl with the underlying of intraosseous malignant fibrous histiocytoma presented with peculiar well-demarcated scaly erythematous macules and patches on diaper area after receiving the first course of cisplatin and doxorubicin. Diagnosis is made by clinical criteria. SDRIFE should be included in differential diagnosis when addressing patients with cutaneous eruption predominantly on diaper area.
Keywords: SDRIFE (Systemic Drug-Related Intertriginous and Flexural Exanthema); Drug eruption; Systemic contact dermatitis; Cutaneous drug reaction.
Citation: Bangxang PN, Nitiyarom R, Wisuthsarewong W, Banomyong N. Unusual presentation of systemic drug-related intertriginous and flexural exanthema (SDRIFE) in children potentially caused by cisplatin and doxorubicin: A case report. J Clin Images Med Case Rep. 2024; 5(12): 3388.
Introduction
There are several types of delayed hypersensitivity reaction to medications categorized by clinical presentation and progression [1]. The most common clinical clue is cutaneous eruption, which could range from mild maculopapular rash to generalized skin necrosis and detachment. Systemic involvement could be found in some conditions, such as Drug Reaction with Eosinophilia and Systemic Symptoms (DRESS). It is crucial to distinguish between severe reactions and non-life-threatening ones as it would have an impact on treatment and sequalae monitoring. We reported an unusual case of delayed type hypersensitivity reaction involving exclusively on diaper area caused by chemotherapy drugs in pediatric patient.
Clinical case
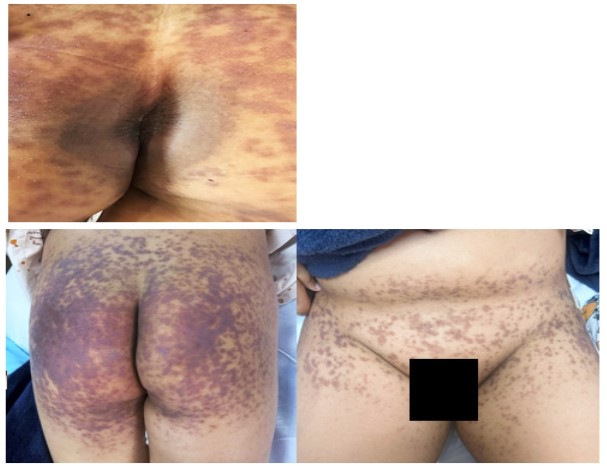
The patient was an 8-year-old girl presented with persistent leg pain on the right side for 1 month after minor trauma. She also reported awakening pain and difficulty weight bearing on right leg. Femur biopsy revealed intraosseous malignant fibrous histiocytoma at distal metaphysis extending to diaphysis of right femur. She was admitted to the hospital for chemotherapy which included an induction phase with doxorubicin, cisplatin, and methotrexate. Leucovorin was also prescribed per protocol to prevent methotrexate toxicity. Two days after receiving the first dose of doxorubicin and cisplatin, she developed a well- demarcated oval erythematous plaque on perianal area (Figure 1A). She had no itching or burning sensation. Two weeks later, the lesion became brownish and less prominent. At the time, she reported numerous well-defined itching and slightly burning erythematous macules and patches with scale on diaper area, involving perianal and inguinal fold (Figure 1B & 1C). The rash gradually increased over a few days and coalesced into purplish plaques. Drug eruption was suspected. She had no systemic symptom nor cutaneous eruption elsewhere. The diagnosis of Systemic Drug-Related Intertriginous and Flexural Exanthema (SDRIFE) was made by using clinical criteria. When considering the drug timeline, doxorubicin and cisplatin were the only two medications prescribed before onset of the rashes. They therefore were suspected of being the culprit and thenon hold. Skin biopsy was performed on the left thigh for standard histopathology examination and direct immunofluores- cence. H&E examination (Figure 2A & 2B) revealed epidermal hyperplasia with basal vacuolar interface dermatitis with sparse lymphocytes, histiocytes, and neutrophils infiltration in the dermis. PAS-D stain showed no thickening basement membrane. Masson fontana stain demonstrated melanin incontinence. Iron Perls stain was negative. Alcian blue pH-2.5 stain was negative for dermal mucin. Direct immunofluorescence showed negative result. Moderate potency topical corticosteroids were prescribed with only a slight improvement. The rash healed with some desquamation and post-inflammatory hyperpigmentation. Drug patch test for doxorubicin and cisplatin was done on the non-lesional site. The attempt failed to identify the causative agents. Drug provocation was then performed by giving 10% of the desired dose of doxorubicin and cisplatin 10 days apart. No new eruption was demonstrated. We concluded the drug provocation test to be negative. She received the full chemotherapy regimen, including cisplatin and doxorubicin, as no alternative treatment was available for her malignancy. Her dermatologic condition did not worsen following the chemotherapy, as anti-histamines were administered as pre-medication for each dose. The diagnosis of SDRIFE was made based on the characteristic rash in skin folds, without systemic symptoms.

Discussion
SDRIFE, sometimes referred to as Baboon syndrome, is the most recognized form of systemic contact dermatitis [2]. It is a rare condition, especially in children, with only a small number of cases reported to date and predominantly affects male [3]. Presentation includes symmetrical well-demarcated erythematous macules or papules symmetrically distributed on intertriginous area, such as perineum, antecubital area. It can be accompanied with local symptoms such as pruritus but not without systemic symptoms. The rash were reported to occur a few hours to days after exposure to the culprit drugs [3]. Diagnosis is usually made clinically by using five diagnostic criteria proposed by Hausermann et al. [4] as followed; [1] exposure to a systemically administered drug, first or repeated doses (contact allergens excluded) [2], sharply demarcated erythema of the gluteal/perianal area and/or V-shaped erythema of the inguinal/perigenital area [3], involvement of at least one other intertriginous/flexural fold [4], symmetry of affected areas, and [5] absence of systemic symptoms and signs. Pathophysiology of SDRIFE is thought to be the type IVc [5] hypersensitivity reaction characterized by the presence of CD3+, CD8+, TIA1+ T cells at dermoepidermal junction [6]. Recent study further highlighted the tendency of Th1- and Th17-driven process in SDRIFE by studying immunophenotypic features in biopsy specimens compared to those with psoriasis and eczema [7]. Histologic features in SDRIFE were likely to be in spectrum of spongiotic dermatitis, superficial and deep perivascular infiltration, and vacuolar interface dermatitis. Other less commonly reported findings were the presence of necrotic keratinocytes, pustular dermatitis, and interstitial granulomatous dermatitis [6,7]. There is no specific pathological feature to differentiate SDRIFE from other skin conditions. The most common etiology is β-lactam antibiotics, especially penicillin [8]. Other associated drugs are sulfa-containing antibiotics, clindamycin, fluoroquinolones, anti-tumor necrosis factor-α (anti-TNF-α), omeprazole, chemotherapy, and Epidermal Growth Factor Receptor (EGFR) inhibitors [9-11]. Latency period in SDRIFE was reported to be as soon as a few hours to days. Aside from using a drug timeline, which is necessary albeit sometimes not sufficient, to identify the culprit agent, many researchers tried to explore the benefit of standard allergic interventions in this condition. Nespoulous et al [3] reported a positive patch test in up to 50% of 55 cases with SDRIFE. There is limited evidence on the use of lymphocyte transformation test and Enzyme-Linked Immunospot (ELISpot) in SDRIFE. Drug provocation is positive in most cases thus believed to be a gold standard test for the condition. Our patient tested negative on the drug provocation test. However, it is important to note that a negative result does not rule out drug-induced eruptions, as drug provocation tests can yield negative outcomes in various cases of drug eruptions [12]. Our patient demonstrated a classic presentation of SDRIFE. Histologic characteristics were also compatible with those of the previous case reports. This could be the first report of an unsual cutaneous eruption possibly caused by doxorubin and cisplastin.
Declarations
Conflict of interest statement: The authors declare that there are no conflicts of interest.
Consent for publication: All authors have provided their consent for publication.
Ethical approval and informed consent: Informed consent was obtained from the patient, and ethical approval has been granted for the study.
References
- Schrijvers R, Gilissen L, Chiriac AM, Demoly P. Pathogenesis and diagnosis of delayed-type drug hypersensitivity reactions, from bedside to bench and back. Clin Transl Allergy. 2015; 5: 31.
- De Groot AC. Systemic allergic dermatitis (systemic contact dermatitis) from pharmaceutical drugs: A review. Contact Dermatitis. 2022; 86(3): 145-64.
- Nespoulous L, Matei I, Charissoux A, Bédane C, Assikar S. Symmetrical Drug-Related Intertriginous And Flexural Exanthema (SDRIFE) associated with pristinamycin, secnidazole, and nefopam, with a review of the literature. Contact Dermatitis. 2018; 79(6): 378-80.
- Häusermann P, Harr T, Bircher AJ. Baboon syndrome resulting from systemic drugs: is there strife between SDRIFE and allergic contact dermatitis syndrome? Contact Dermatitis. 2004; 51(5- 6): 297-310.
- Huynh T, Hughey LC, McKay K, Carney C, Sami N. Systemic drug-related intertriginous and flexural exanthema from radio contrast media: A series of 3 cases. JAAD Case Rep. 2015; 1(3): 147- 9.
- Muresan AM, Metze D, Böer-Auer A, Braun SA. Histopathological spectrum and immunophenotypic characterization of symmetrical Drug-related intertriginous and flexural exanthema. Am J Dermatopathol. 2021; 43(2): 103-11.
- Chaudet KM, Russell-Goldman E, Horn TD, Schuler AM, Chan MP, et al. Characterization of T-helper immune phenotype in Symmetrical Drug-Related Intertriginous And Flexural Exanthema (SDRIFE) endorses a delayed-type hypersensitivity reaction. Am J Dermatopathol. 2024; 46(2): 71-8.
- Schuler AM, Smith EH, Chaudet KM, Bresler SC, Gudjonsson JE, et al. Symmetric drug-related intertriginous and flexural exanthema: Clinicopathologic study of 19 cases and review of literature. J Cutan Pathol. 2021; 48(12): 1471-9.
- Alpagat G, Baccioglu A, Dumanoglu B, Alan Yalim S, Kalpaklioglu AF. Amoxicillin/clavulanic acid-induced symmetric drug-related intertrigious and flexural exanthema. Cureus. 2023; 15(1): 33849.
- Megna M, Camela E, Ocampo Garza SS, Marino V, Costanzo L, et al. Ciprofloxacin-induced symmetrical drug-related intertriginous and flexural exanthema (SDRIFE) in a psoriasis patient. Contact Dermatitis. 2021; 85(4): 467-9.
- Spigariolo CB, Barei F, Maronese CA, Barberi F, Cattaneo A, et al. Three cases of symmetrical drug-related intertriginous and flexural exanthema (SDRIFE) induced by proton-pump inhibitors. Australas J Dermatol. 2022; 63(4): 509-12.
- Misirlioglu ED, Toyran M, Capanoglu M, Kaya A, Civelek E, et al. Negative predictive value of drug provocation tests in children. Pediatr Allergy Immunol. 2014; 25(7): 685-90.