
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 5
Tofacitinib therapy in a challenging severe atopic dermatitis in an adult patient restored his quality of life: A patient perspective
*Corresponding Author : Avik Mondal
Department of Dermatology & Venereology, AIIMS,
Kalyani, West Bengal, India.
Email: avik.mondal11@gmail.com
Received : Nov 21, 2024
Accepted : Dec 10, 2024
Published : Dec 17, 2024
Archived : www.jcimcr.org
Copyright : © Mondal A (2024).
Abstract
Severe uncontrolled atopic dermatitis in adult is very troublesome which impacts negatively over social and personal life significantly. I’m presenting a case where an adult patient completely lost hope due to his chronicity and severity of disease despite being on conventional treatment, taking intermittently since his childhood. Tofacitinib, a JAK inhibitor, acts as a rescue medication for his debilitating condition and revive his daily active life in terms of interpersonal relationship, social interaction and job within 7 months of treatment. His SCORAD index, EASI (eczema area severity index) and DLQI (Dermatological Life Quality Index) were 75.25, 15.9 & 30 respectively which subsequently decreased to 3.25, 0.3 and zero.
Keywords: Tofacitinib; Atopic dermatitis; DLQI; Scorad; Depression.
Citation: Mondal A. Tofacitinib therapy in a challenging severe atopic dermatitis in an adult patient restored his quality of life: A patient perspective. J Clin Images Med Case Rep. 2024; 5(12): 3389.
Background
Atopic dermatitis is a chronic relapsing remitting inflammatory skin disease seen in children which usually resolves in adulthood [1,2]. Treatment includes topical corticosteroid, topical calcineurin inhibitors and orally steroid and cyclosporin [1]. For resistance cases, moderate to severe atopic dermatitis, IL4/ IL13 inhibitor, JAK inhibitors have been recently introduced [3]. Tofacitinib, a small molecule inhibits IL4 cytokine directly and also inhibits JAK-STAT signal in keratinocytes [4,5]. But, when it persists after adolescent in severe form, brings severe psychosocial impact as in our case which lands a person in home for several years, bedridden, indolent, apathy towards social interaction and jobless. Tofacitinib gave a new life to this patient in terms of almost complete improvement in quality of life and disease itself.
Case presentation
A 36-year-old unmarried male patient, a gym trainer by occupation with known case of bronchial asthma and atopic dermatitis since his childhood presented with chief complaints of dry itchy erythematous fissured diffuse plaques over the head and neck region, trunk and upper limb sparing the lower limbs.
Patient was apparently well before 2 years of age. He developed scaling with dryness over the flexures in his childhood which gradually extending to involve whole body. It usually exacerbated in winter and subsided up to some extent in summer. He was treated multiple times with topical corticosteroid, antihistamines, on & off prednisolone 30-50 mg on tapering dose even with methotrexate 10-15 mg/wk or cyclosporin 100-200 mg/ day, several times with mild to moderate improvement. He was in less severe form of atopic dermatitis for 16 yrs in between but never in complete remission, always had mild form of dermatitis present throughout the year. He presented us in April 2022 with BSA involvement around 60% with erythema, scaly lichenified diffuse plaque with severe itching, burning, dyspigmentation, fissuring & erosions [SCORAD index – 75.25 & Eczema area severity index (EASI) – 15.9%] for which he couldn’t not even sleep for whole night (Figures 1-4). He used to cover his whole face to avoid public attention, even in ward stay most of the time he covered the face to avoid embarrassment. He even needed assistance from her mother in his day-to-day activity. He used to look very anxietic and depressed thinking about the severity & chronicity of the disease. Had severe psychosocial impact with DLQI 30 (Table 1).



Investigations
Before starting tofacitinib routine investigations complete blood count, liver function, renal function, fasting lipid profile, mantoux test, chest X-ray had been done to look for any abnormality and to rule out latent tuberculosis. All reports are within normal limit except serum IgE which was >5000. We routinely have been checking up his lipid profile which found out to be normal.
Treatment
We have started tofacitinib 5 mg twice daily along with betamethasone 0.1% cream for body lesions and tacrolimus 0.1% ointment for face. Initially, he had moderate improvement but again had an exacerbation in June, to control the acute exacerbation a short course of oral mini pulse with betamethasone 5 mg tablet twice weekly given for 2 months and tofacitinib dose was hiked up to 10 mg at morning and 5 mg at evening and continuously taking same dose of tofacitinib with complete resolution has been achieved (Figures 1-4). He has only residual reticular post inflammatory hyperpigmentation and a mildly itchy lichenified plaque over nape of neck.
Patient has been following up for 6 months after complete improvement. Now he has been maintaining on tofacitinib 5 mg twice daily with just one time application of emollient with no flare up episode in between or no requirement of any other medications. His lipid profile and liver function tests are normal monitoring 2-3 monthly while on tofacitinib without much derangement in parameters.
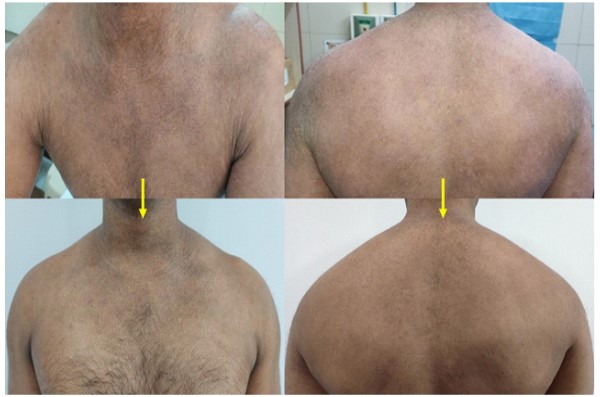
Table 1: Showing the miraculous improvement in quality of life and also in disease.
| Parameters | April, 2022 | October, 2022 | Improvement in percentage |
|---|---|---|---|
| SCORAD index | 75.25 | 3.25 | 96% reduction |
| EASI | 15.9 | 0.3 | 98% reduction |
| DLQI | 30 | 0 | 100% improvement |
SCORAD: Scoring Atopic Dermatitis; EASI: Eczema area severity index; DLQI: Dermatological life quality index.
Discussion
Severe chronic atopic dermatitis in adult patient impacts negatively in terms of quality of life, disfigurement, itching & discomfort associated with significant increase in depression and suicidal thoughts [6,7]. As patient previously took cyclosporin and methotrexate along with on and off prednisolone with mild to moderate improvement and also thought of their side effect profile and rebound flare after discontinuation, we decided to give tofacitinib as an alternate drug [8]. Tofacitinib is a JAK inhibitor that predominately blocks JAK1 and JAK3. The critical Th2-associated cytokines IL-4 and IL-13 utilize JAK1 (IL-13) and JAK3 (IL-4) for signaling in keratinocytes [9]. This medication is also without any serious side effect except infection which needs close follow up which we have been doing in this patient and he didn’t experience any adverse event due to this drug.
Patient’s perspective
“I’m very happy as there is extensive improvement in eczema, itching and also in my social interaction. Now I can go out for shopping and meet people with full confidence. I was totally bedridden and home bound for several years. Hardly go outside and meet people. Always need assistance from my mother. My marriage has been delayed due to this disease. Now I can do my job with no feeling of embarrassment in mind. Many people said that my disease is rare, it cannot be treatable, even I thought of going abroad for treatment. I’m very pleased to get all the attention received from AIIMS and do not mind if all doctors learning from my case or my condition being discussed. I feel all right now, I come to OPD regularly for follow up. In these 7 months I did not feel any adverse event related to treatment but little bit concerned about the sustainability of response after stoppage of treatment” – In patient’s own language.
Learning points
1. This is a unique case where patient subjectively and objectively got improved significantly.
2. Patient’s own words describe his satisfaction with treatment and positivity towards life which was entirely opposite just before 6 months.
3. Patient’s personal life in respect to interpersonal relationship and social interaction got restored completely.
Declarations
Funding sources: None.
Conflicts of interest: None declared.
Patient consent for publication: Obtained.
References
- Langan SM Irvine AD Weidinger S Atopic dermatitis. Lancet. 2020; 396: 345-360.
- Flohr C, Mann J. New insights into the epidemiology of childhood atopic dermatitis. Allergy. 2014; 69: 3-16.
- Drucker AM, Ellis AG, Bohdanowicz M, Mashayekhi S, Yiu ZZ, et al. Systemic Immunomodulatory Treatments for Patients with Atopic Dermatitis: A Systematic Review and Network Metaanalysis. JAMA Dermatol. 2020; 156: 659-67.
- Meyer DM, Jesson MI, Li X, Elrick MM, Funckes-Shippy CL, et al. Anti-inflammatory activity and neutrophil reductions mediated by the JAK1/JAK3 inhibitor, CP-690,550, in rat adjuvant-induced arthritis. J Inflamm. 2010; 7: 41.
- Krueger J, Clark JD, Suárez-Fariñas M, Fuentes-Duculan J, Cueto I, et al. A3921147 Study Investigators. Tofacitinib attenuates pathologic immune pathways in patients with psoriasis: A randomized phase 2 study. J Allergy Clin Immunol. 2016; 137: 1079- 90
- Patel KR, Immaneni S, Singam V, Rastogi S, Silverberg JI. Association between atopic dermatitis, depression, and suicidal ideation: a systematic review and meta-analysis. J Am Acad Derma- tol. 2019; 80: 402-410.
- Taieb C, Finlay AY, Nguyen C, Sante PF, Myon E. Adults with atopic dermatitis: quality of life impact. J Am Acad Dermatol. 2005; 52: 66.
- Drucker AM, Eyerich K, de Bruin-Weller MS. Use of systemic corticosteroids for atopic dermatitis: International Eczema Council consensus statement. Br J Dermatol. 2018; 178: 768-775.
- Peterson DM, Vesely MD. Remission of severe atopic dermatitis with dupilumab and rescue tofacitinib therapy. JAAD Case Rep. 2021; 10: 4-7.