Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Clinical Image - Open Access, Volume 5
Multi-systemic melioidosis
Naveen kumar*
Department of Radiodiagnosis, Yashoda Hospital, Secunderabad 500003, Telangana, India.
*Corresponding Author : Naveen kumar
Department of Radiodiagnosis, Yashoda Hospital,
Secunderabad 500003, Telangana, India
Email: knkumar483@gmail.com
Received : Nov 22, 2024
Accepted : Dec 11, 2024
Published : Dec 18, 2024
Archived : www.jcimcr.org
Copyright : © Kumar N (2024).
Abstract
Melioidosis is a severe infectious disease caused by Burkholderia pseudomallei, a Gram-negative bacterium endemic to tropical regions. While it most commonly affects the lungs, melioidosis can present as a multisystemic infection, impacting various organ systems, including the liver, spleen, kidneys, skin, and central nervous system. The clinical manifestations of multisystemic melioidosis are diverse and range from localized abscesses and septicemia to more severe presentations such as pneumonia, Acute Respiratory Distress Syndrome (ARDS), and disseminated infection with organ failure. Risk factors include diabetes mellitus, chronic renal disease, immunosuppression, and trauma, which increase susceptibility to the infection. The pathogenesis of melioidosis is characterized by the ability of B. pseudomallei to evade host immune responses, forming intracellular reservoirs and leading to chronic infection. Diagnosis is often challenging due to its non-specific symptoms and requires microbiological culture, PCR, and serological tests. Treatment involves prolonged courses of intravenous and oral antibiotics, with ceftazidime and meropenem being first-line agents. Despite appropriate therapy, the mortality rate remains high, particularly in cases with delayed diagnosis or in immunocompromised patients. Understanding the pathophysiology, risk factors, and optimal management strategies for multisystemic melioidosis is crucial for improving patient outcomes in endemic regions and for travelers to these areas.
Keywords: Melioidosis; Burkholderia pseudomallei; Multisystemic infection; Sepsis; Pneumonia; Organ failure; Diagnosis; Treatment; Tropical disease.
Citation: Kumar N. Multi-systemic melioidosis. J Clin Images Med Case Rep. 2024; 5(12): 3392.
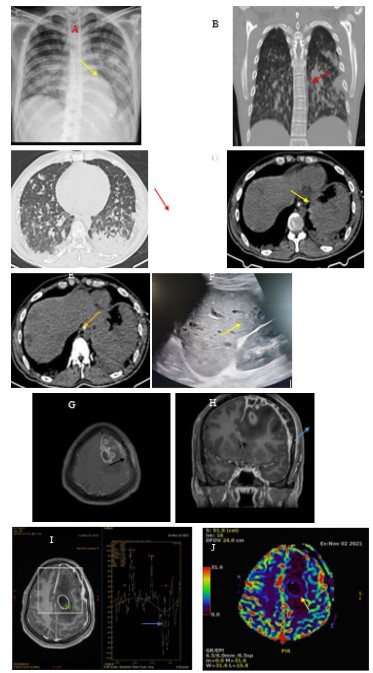
Description
A 25-year-old male who is a farmer presented to the Emergency Department with complaints of fever and headache. The patient does not have any comorbidities. Routine blood tests showed an Erythrocyte Sedimentation Rate (ESR) 36 mm, C- Reactive Protein (CRP) of 42.96 mg/L, and a White Blood Cell (WBC) count of 11.8×103 /mm3 with 75.8% neutrophils, normal platelets, and creatinine. The patient’s fasting plasma glucose level was 125 mg/dl. Pulmonary tuberculosis was suspected initially but sputum culture came as negative. Melioidosis is common in our region so systemic melioidosis was suspected No genitourinary involvement was noted in the patient. Venous blood was obtained for blood culture and selective media was used for culture. Real-time PCR also confirmed melioidosis. Intravenous Ceftazidime for 4 weeks, followed by oral maintenance therapy with cotrimoxazole for 4 months. Patient was improved after continuous antibiotic therapy.