
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Clinical Image - Open Access, Volume 5
Role of MRI in post traumatic anosmia
Nidhi Singh1*; Prasanth L1; Roohie Singh2; Varun Jerath3; KP Senger4; Hari Kumar S5
1Resident, Department of ENT & HNS, Command Hospital (Eastern Command), Kolkata, India.
2Professor, Department of ENT & HNS, Command Hospital (Eastern Command), Kolkata, India.
3Professor, Department of ENT & HNS, Army Hospital (R & R), Delhi, India.
4Associate Professor, Department of Radiology, Command Hospital (Eastern Command), Kolkata, India.
5HOD, Department of ENT & HNS, Command Hospital (Eastern Command), Kolkata, India.
*Corresponding Author : Nidhi Singh
Resident, Department of ENT & HNS, Command
Hospital (Eastern Command), Kolkata, India.
Email: nidhisingh71998@gmail.com
Received : Nov 22, 2024
Accepted : Dec 12, 2024
Published : Dec 19, 2024
Archived : www.jcimcr.org
Copyright : © Singh N (2024).
Citation: Singh N, Prasanth L, Singh R, Jerath V, Senger KP, et al. Role of MRI in post traumatic anosmia. J Clin Images Med Case Rep. 2024; 5(12): 3393.
Description
39 years male, soldier by profession, hailing from Bihar presented with chief complaints of smell disturbance within two weeks of an occipital blow on head due to fall from 10-feet height during his house construction work. The fall had happened two months back with no loss of consciousness, seizure, bleeding from any sites, blurring of vision or any other ENT complaints. Previously, he had hyposmia which a month later had developed into episodes of parosmia and phantosmia, sometimes on exposure to odorant and sometimes spontaneously. This smell disturbance gradually progressed to make him anosmic two months post head injury and now he also complained of loss of taste sensation. The patient denied history of sinonasal disease, prior facial trauma, nasal surgery or any addiction. He was empirically started on Intra-nasal Corticosteroids sprays by some medical practitioner for four weeks with no alleviation of symptoms. Patient gives history of Hansen’s disease 14 years back with no nasal involvement and also COVID-19 infection two years back with preserved smell and taste sensations. ENT and head-neck examination (including nasal endoscopy) was done which was normal except for loss of smell. Patient could identify basic tastes (sweet, salty, sour and bitter). NCCT Head (done post injury) was reviewed at our centre which revealed fracture of (L) occipital bone along with subdural hematoma. Previous 1 T MRI Brain also revealed no significant abnormality.
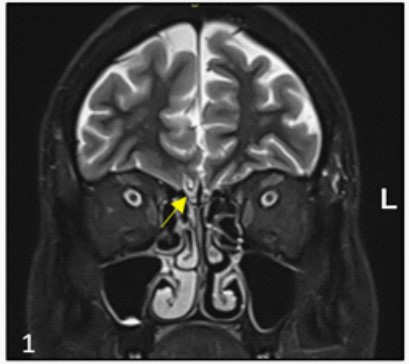
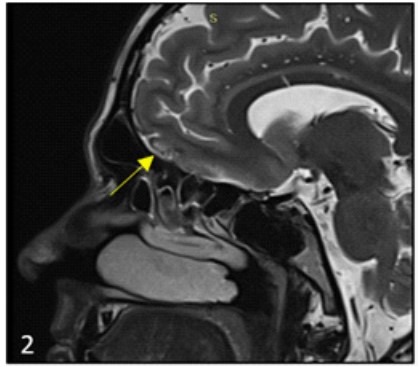
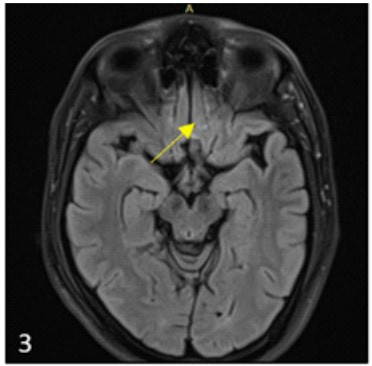
We did 3 Tesla Contrast Enhanced MRI (CE-MRI) brain with olfactory complex which showed asymmetry of olfactory bulbs (right appearing relative smaller than left side). There was focal T2/FLAIR hyperintensity involving gyrus rectus (Right > Left) which on T1W1 showed cortical laminar necrosis at places suggestive of encephalomalacia with gliotic changes in the gyrusrectus (Figures 1-3).
Discussion
In a case of head trauma, life-threatening injuries are more focussed upon due to which smell dysfunction is often missed out. Generally, total anosmia occurs in 5-10% of head trauma and as many as 30-40% victims suffer with atleast partial loss of smell sensation (anosmia) [1]. MRI has demonstrated abnormalities in olfactory bulb and tract with inferior frontal lobe in cases of post-traumatic olfactory dysfunction [3]. In acute in- jury [2], hemorrhagic contusion and shearing injuries to inferior frontal lobe and olfactory apparatus may be seen as hyperintensity on T1 weighed images (indicating hemorrhage) and T2 weighed images (indicating edema). In chronic injury, residual gliosis may be seen as hyperintensity [1,4]. Computed tomography scans remain superior to MRI in assessment of bony injury [1]. In our case, it is possible that shearing of olfactory nerve fibres at the entry through cribriform plate would have been contributory to patient’s symptoms. We propose that 3T CEMRI may alert the clinician about olfactory tract injury in such cases of head trauma which will help early and adequate patient counselling and management of this common yet troublesome sequela of head injury.
Declarations
Conflicts of interest: Nil.
Informed consent: Informed consent was taken from the patient for this publication.
Funding: No funding was received to assist with the preparation of this manuscript. The authors have no relevant financial or non-financial interests to disclose.
References
- Wise JB, Moonis G, Mirza N. Magnetic resonance imaging findings in the evaluation of traumatic anosmia. Ann Otol Rhinol Laryngol. 2006; 115(2): 124-7. doi: 10.1177/000348940611500208. PMID: 16514795.
- Costanzo RM, Becker DP. Smell and taste disorders in head injury and neurosurgery patients. In: Meiselman HL, Rivlin RS, eds. Clinical measurement of taste and smell. New York, NY: Macmillan. 1986: 565-78.
- Yousem DM. Geckle RJ. Bilker WB. McKeown DA, Doty RL. Post-traumatic olfactory dysfunction: MR and clinical evaluation. AJNR Am J Neuroradiol 1996; 17: 1171-9.
- Grossman RI, Yousem DM. Neuroradiology-the requisites. St Louis, Mo: Mosby. 1994; 149-70.