
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 5
Refractory Ogilvie Syndrome: Can we get ahead of the damage control?
Rita Marques1,4*; Ana Costa2,4; Miguel Sá Vieira3,4; Urânia Fernandes1,4; Ricardo Vaz-Pereira1,4; João Pinto-de-Sousa1,4
1Surgery Department of “Unidade Local de Saúde Trás-os-Montes e Alto Douro” (ULSTMAD), Portugal.
2Internal Medicine Department of Hospital das Forças Armadas Porto (current), previous “Unidade Local de Saúde Trás-os-Montes e Alto Douro” (ULSTMAD), Portugal.
3Anesthesiology Department of “Unidade Local de Saúde Trás-os-Montes e Alto Douro” (ULSTMAD), Portugal.
4Clinical Academic Center Trás-os-Montes e Alto Douro (CACTMAD), Portugal.
*Corresponding Author : Rita Marques
Surgery Department of “Unidade Local de Saúde
Trás-os-Montes e Alto Douro” (ULSTMAD), Portugal.
Email: RitaRA@chtmad.min-saude.pt
Received : Nov 05, 2024
Accepted : Dec 16, 2024
Published : Dec 23, 2024
Archived : www.jcimcr.org
Copyright : © Marques R (2024).
Abstract
Colonic pseudo-obstruction is a rare yet concerning pathology, that falls within the surgeon´s scope when complications arise, making surgical intervention paramount to control the damage.
The present case report aims to describe a refractory case of colonic pseudo-obstruction and its surgical management, along with a modest literature review of this challenging and often misunderstood condition.
Keywords: Colonic pseudo-obstruction; Ogilvie syndrome; Colonic endoscopic decompression; Neostigmine; Ileostomy.
Abbreviations: PCO: Colonic Pseudo-Obstruction; OSA: Obstructive Sleep Apnea; PEG: Percutaneous Endoscopic Gastrostomy; VP: Ventriculoperitoneal Shunt; EN: Enteral Nutrition; IV PEC: Percutaneous Endoscopy Colostomy; PN: Parenteral Nutrition; ASA: American Society of Anesthesiologists classification; CT: Computed Tomography.
Citation: Marques R, Costa A, Sá Vieira M, Fernandes U, Vaz-Pereira R, et al. Refractory Ogilvie Syndrome: Can we get ahead of the damage control?. J Clin Images Med Case Rep. 2024; 5(12): 3398.
Introduction
Colonic Pseudo-Obstruction (PCO) is characterized by acute colonic functional dilatation without mechanical obstruction [1-8]. It frequently affects elderly patients with multiple comorbidities [1,2,4,5]. Diagnosis is primarily radiological, upon exclusion of obstruction and often associated with electrolyte imbalance [1-3]. Treatment can be surgical, mainly in the presence of complication (cecum >12 cm and/or peritoneal signs) and therefore resection with stoma is the standard [3]. Supportive treatment includes bowel rest, correction of imbalances, fluid resuscitation, cessation of toxic medications and decompression via nasogastric tube or rectal probe [1,2,4,5]. Neostigmine and/or colonic endoscopic decompression may resolve the situation. Refractory patients pose significant challenges, leaving the burden to a surgical approach and the consequent non-negligible mortality [1-4].
Case presentation
We report the case of a 69-year male patient. He reported previous high blood pressure, obesity, tobacco use and Obstructive Sleep Apnea (OSA) requiring the use of continuous positive airway pressure therapy.
In January of 2023 he was admitted to the emergency department due to a spontaneous hemorrhagic stroke with midline shift. The patient underwent a decompressive craniotomy, later complicated with meningitis and health care associated infections culminating in long stay in the intensive care unit and hospital (101 days total). During this period, he had a Percutaneous Endoscopic Gastrostomy (PEG) placed for feeding, a tracheostomy (later closed) and a Ventriculoperitoneal Shunt (VP) due to hydrocephalus.
Upon discharge, he was described as having right hemiparesis (mainly brachyfacial), global aphasia and right homonymous hemianopsia.
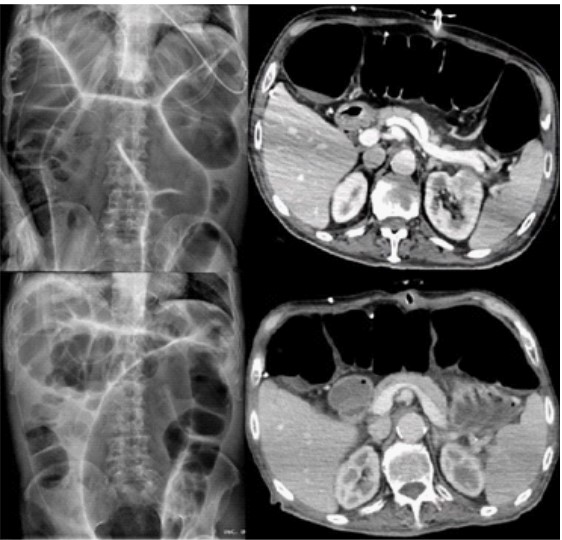
The patient was transferred to a medical recovery facility for rehabilitation, with initial good outcome. However, in the following 6 months, the patient experienced multiple emergency department admissions and hospitalizations due to abdominal distention, constipation and neurologic deterioration. Further investigation led to the diagnosis of Ogilvie syndrome (Figure 1) with implicit VP shunt compression and, thereby, compromised neurological status. At first, he was treated conservatively with success, discharged with osmotic laxatives, suspension of drugs such as selective serotonin reuptake inhibitors and a program, in the medical facility, for on-demand placement of rectal probe to decompress. However, he was re-admitted in November with a new episode of severe colonic distention, during which neostigmine (2 mg intravenous IV) was performed with limited benefit. Further need for colonic endoscopic decompressions (total of 4 in subsequent episodes) was necessary, also with short-lived success.
Due to progressive worsening and nutritional limitation, with weight loss and cachexia, rifaximin was tried, on the assumption of possible small intestine bacterial overgrowth, and culinary diet was discontinued and replaced with Enteral Nutrition (EN), with partial response.
Attempts to explore minimally invasive decompression options, such as Percutaneous Endoscopy Colostomy (PEC) was fruitless. Therefore, the decision was made to place a venous central catheter for supplemental Parenteral Nutrition (PN) along with EN in preparation for a surgical approach. Weekly clinical and laboratory evaluation indicated a weight gain of 4kg in 4 weeks, despite the need of dosage adjustments. Given his frailty, hemorrhagic stroke and OSA he was deemed as a high-risk patient (American Society of Anesthesiologists classification ASA 4) and, attempting to avoid general anesthesia, we planned the surgical procedure under continuous spinal anesthesia and minimal sedation. Crucial pre-operative endoscopic decompression was performed to minimize distention and avoid further complications.
In June 2024 an ileocolectomy with separate colonic mucosal fistula and terminal ileostomy was performed without surgical complications (Figure 2). The post-operative period was complicated with PEG dislocation, which was resolved after replacement and the patient was discharged at day 8. Subsequently, PN was gradually decreased (suspended on the 15th day of post operative) while increasing EN and incorporating culinary food by mouth whenever feasible (which was only possible due to significant enhancement of neurologic status). The last need for enema occurred on day 32th post-operative with a weight gain of 8 kg and considerable improvement in independence and rehabilitation cooperation, mainly due to neurologic enhancement.
Post-operative plain-film radiographs showed dramatic evolution (Figure 3).


Discussion
Colonic pseudo-obstruction is a functional disorder with acute dilatation of the colon in the absence of a mechanical obstruction. It typically affects the right colon but can extend till the rectum, with a higher prevalence in elderly males (over 60 years old) [1,2]. This condition is rare, occurring in 1 in 1000 admissions per year [3-5].
It frequently arises in hospitalized patients with multiple co-morbidities and in post-operative period, mainly orthopedic surgery [1,2,4,5]. Up to 9.3% of cases occur in patients with neurological conditions, such as cerebrovascular accident [3,5].
The etiology of PCO is unascertained although it is possible to point an impairment of central nervous system [5-8]. Previous theories suggested unopposed parasympathetic activity leading to uncoordinated movements. In contrast, more recent theories propose a sympathetic overdrive, reduced parasympathetic activity or a merge of both [3,8].
The condition is often referred to as Ogilvie syndrome, reported by Sir Heneage Ogilvie, who described it in 1948, although his description was of malignant infiltration of vertebral ganglia [3,6].
Clinical symptoms include abdominal distention (with rapid onset in 24-48 hours or progressive over 3-7 days), abdominal pain in about 80%, nausea and vomiting in 60%, constipation in 50% and diarrhea in 40% of cases [1,2,5,7].
Physical examination typically reveals a tympanic abdomen with present bowel sounds and in 65% of cases accompanied with tenderness. Warning signs such as fever, hypotension, tachycardia and peritoneal signs should raise the possibility of complication [3].
Laboratory tests include complete blood count, electrolytes, C-reactive protein, thyroid hormones and serum lactate level; a stool culture for Clostridioides difficile toxin may be performed if diarrhea is present [1]. Even though there are no pathognomonic findings, more often leukocytosis and electrolyte imbalance are present (50% of cases) [1]. Radiological studies consist of a plain-film abdominal radiograph [4], an abdominal Computed Tomography (CT) scan with IV, oral and rectal contrast [3] or a contrast enema; colonoscopy is not recommended in this setting due to the risk of perforation [1,2].
Treatment is contingent upon cecal diameter and duration of distension, which are good indicators for perforation risk. When the cecal diameter exceeds 10-12 cm for over 6 days, the risk is substantial, reaching 23% if over 14 cm [1-4].
In uncomplicated cases (cecal diameter less than 12 cm without warning signs), treatment is supportive consisting on treating underlying infection, correcting electrolyte imbalances, providing fluid resuscitation and allowing bowel rest. Avoidance of medications that decrease colonic mobility (such as opioids or anticholinergic drugs), ambulation and decompression (via nasogastric tube or rectal probe) are also recommended [1,2,4,5]. Serial clinical and radiological evaluations are critical, as a favorable outcome is seen in 70-90% of cases [1-4]. If successful, low dose polyethylene glycol laxatives are recommended [5].
Risk factors that decrease the likelihood of successful conservative treatment include male gender, younger age, abdominal distention as primary complaint, postoperative status, elec- trolyte imbalance and greater cecal diameter [4].
In cases of persistent symptoms (exceeding 48-72 h), neostigmine, a cholinesterase inhibitor, (2- 2,5 mg IV bolus) has proven success as a single dose in 60-94% of cases, with a recurrence rate of less than 31% and an overall long-term response of 69-100%. Absolute contra-indications include intestinal or urinary obstruction and hypersensitivity reaction while relative contraindications include bradycardia, asthma, renal insufficiency, peptic ulcer disease, recent myocardial infarction, and acidosis [4]. A second dose has been effective in 40-100% of patients [2,4]. Continuous administration or subcutaneous use is being reported but requires further validation, as the latest obliviates the need for cardiac monitoring, which may be regarded as advantageous [3].
Colonic endoscopic decompression used to be proposed as first line treatment, prior to the use of neostigmine, although it does not demonstrate a reduction in overall outcomes (length of hospital stay, intensive care unit stay or colostomy rate) and therefore is not widely recommended [4]. The goal is to achieve decompression of the hepatic flexure, because right colon decompression is therefore feasible. Although the placement of a decompression tube in transverse colon has been described, its utility has yet to be established. Signs of ischemia, such as petechial hemorrhage or superficial ulceration do not warrant surgical exploration, as they are present in 10% of cases, and require nonetheless, continuous evaluation [3,5]. The success rate is reported to be between 61-95%, though many patients require more than one procedure due to a 40% recurrence. Nevertheless, the perforation rate is 1-3% with a mortality rate of 1% [2-4].
In refractory cases, which vary in frequency amongst studies (10-24%), the use of prucalopride or pyridostigmine has been described; however, their effectiveness has yet to be confirmed [2- 4,7].
In parallel percutaneous endoscopy colostomy, preferably placed in cecum, may be considered, with reported success rate exceeding 80%, although the evidence is still insufficient [2,4,5]. The technique is similar to PEG placement (Seldinger method) under direct visualization [5].
Hence, surgery becomes the ultimate stronghold, starting with cecostomy, despite the risks of sepsis, leakage and catheter displacement [3]. Laparoscopic assisted PEC (LAPEC) is also an alternative, although the need for extensive sedation is a disadvantage [5].
Thus surgery, appears as the solution for the complication (ischemia or perforation) but specific data for elective surgery in refractory cases is sparse [2,4]. Even in asymptomatic patients, cecum diameter remains a good predictor for the need of surgery [6].
Whenever needed, urgent approach implies damage control in the form of a right hemicolectomy with terminal ileostomy, with or without mucous fistula. Anastomosis in the setting of a complication is generally inadvisable, howbeit subject to surgeon’s decision [3]. The debate between laparotomy versus laparoscopy remains; hardly evidence has enlightened it, plausibly due to the predominance of case series or expert opinions and its omission in guidelines [2,4].
Mortality rates are significant, reaching up to 40-50% in complicated cases of perforation or ischemia compared to 15% in uncomplicated patients [1,4,6,8].
Regarding our case, the optimization of electrolyte imbalances, pharmacologic therapies and nutrition, as well as the use of neostigmine, intermittent placement of rectal probe and endoscopic decompressions (total of 4 in sequential episodes) proved unsatisfactory in controlling symptoms. A second dose of neostigmine was not considered, nor was the use of prucalopride (authorized in the European Union) due to the patient’s progressively negative evolution.
Consequently, we were driven to explore more invasive procedures, such as endoscopic cecostomy, which was not feasible, perhaps due to lack of experience and, therefore, surgery remained as the last option. Albeit the scarcity of evidence regarding nutrition in these patients, its optimization, both EN and PN were, in our opinion, crucial to improving clinical status and surgical success. Thus, the involvement of a multidisciplinary team in the decision-making process was paramount in obtaining the utmost conditions for this invasive procedure and, consequently, better outcomes.
A notable downside was the time lapse and subsequent cachexia, conditioning missed rehabilitation milestones and, in the end, hindered the neurological recovery.
In respect to the surgery, this case exemplifies the transposition of the typical urgent procedure into an elective setting with the singularity of being performed without general anesthesia. Given that the patient is incapable of self-care, the construction of a separate mucous fistula and terminal ileostomy allowed, in our perception, for better healing, prevented the spillage of enteric content to the colon and possible recurrence. The remarkable recovery, evidenced by no further need for enemas, the reduction in abdominal suffering and the consequent improvement in neurologic status, leading to an improvement in quality of life, validates this approach which was pioneer in our hospital center and perhaps in the country.
Conclusion
Colonic pseudo-obstruction is a challenging pathology due to its infrequency, misunderstood etiology, the specific patient subset of patients it affects, and as the lack of highly effective targeted treatments.
Although guidelines provide orientation for complicated and non-responsive patients, there is a scarcity of defining strategies for refractory cases. This oversight appears to be imprudent, given the likelihood of complication and therefore the need to resort to damage control surgery.
Further investigation in the area is mandatory to aspire better outcomes as well as greater awareness among health professionals of its negative impact on physical and neurologic re- covery, especially for patients who are unable to complain.
Acknowledgement: Special thanks to Dra. Joana Rua for all the support.
References
- Michael Camilleri, Nicholas Talley, Kristen M Robson. Acute colonic pseudo-obstruction Ogilvie’s syndrome. 2023. https:// www.uptodate.com/contents/acute-colonic-pseudo-obstruction ogilviessyndromesearch=ogilvie&source=search_result&se lectedTitle=1%7E33&usage_type= default&display_rank=1.
- Alavi K, Poylin V, Davids SJ, Patel VS, Felder S, et al. The American Society of Colon and Rectal Surgeons Clinical Practice Guidelines for the Management of Colonic Volvulus and Acute Colonic Pseudo-Obstruction. Diseases of the Colon & Rectum. 2021; 64: 1046-1057.
- Thomas A, Burgess A. Acute Colonic Pseudo-Obstruction. Clinical Colon Rectal Surgery. 2022; 35: 221-226.
- Naveed M, Laith HJ, Fujii-Lau LL, Al-Haddad M, Fishman SD, Jue LT, et al. American Society for Gastrointestinal Endoscopy guideline on the role of endoscopy in the management of acute colonic pseudo-obstruction and colonic volvulus. Gastrointestinal endoscopy. 2020; 91(2): 202.
- Vanek P, Urban O, Falt P. Percutaneous endoscopic cecostomy for management of Ogilvie’s syndrome: a case series and literature review with an update on current guidelines (with video). Surgical Endoscopy. 2023; 37: 8144-8153.
- Joechle K, Guenzle J, Utzolino S, Fichtner-Feig S, Kousoulas L. Ogilvie’s syndrome-is there a cutoff diameter to proceed with upfront surgery?. Langenbeck’s Archives of Surgery. 2022; 407: 1173-1182.
- Haj M, BSca MH, Rockey DC. Ogilvie’s syndrome: management and outcomes, Medicine. 2018; 97: 27.
- Wells IC, O’Grady G, Bissett IP. Acute colonic pseudo-obstruction: A systematic review of aetiology and mechanisms. World Journal of Gastroenterology. 2017; 23(30): 5634-5644.