
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 5
Double management of blood lipids in male SLE patients with severe diffuse coronary artery disease
Xue Jin Chen; Ji Hao; Wen Biao Cai; Hao Ran Li; Chun Mei Qi*
Department of Cardiovascular Medicine, the Second Affiliated Hospital of Xuzhou Medical University, Xuzhou 221000, China.
*Corresponding Author : Chun Mei Qi
Department of Cardiovascular Medicine, the Second
Affiliated Hospital of Xuzhou Medical University,
Xuzhou 221000, China.
Email: 92990025@qq.com
Received : Nov 11, 2024
Accepted : Dec 17, 2024
Published : Dec 24, 2024
Archived : www.jcimcr.org
Copyright : © Mei Qi C (2024).
Keywords: Coronary heart disease; Systemic lupus erythematosus; Blood lipids; Statins; Proteinase subtilisin 9 (PCK9) inhibitor; Combined therapy.
Abbreviations: SLE: Systemic Lupus Erythematosus; CHD: Coronary Atherosclerotic Heart Disease; LDL-C: Low Density Lipoprotein-Cholesterol; Lp(a): Lipoprotein (a); PCSK9: Preprotein Converting Enzyme Subtilisin Kexin 9; EF: Ejection Fraction; CVD: Cardiovascular Diseases.
Citation: Jin Chen X, Hao J, Biao Cai W, Ran Li H, Mei Qi C. Double management of blood lipids in male SLE patients with severe diffuse coronary artery disease. J Clin Images Med Case Rep. 2024; 5(12): 3399.
Introduction
Systemic Lupus Erythematosus (SLE) is an autoimmune disease with multiple system damage, mostly in women and relatively rare in men. The disorder of immune function caused by systemic lupus erythematosus increases the risk of atherosclerosis. Coronary artery lesions in SLE patients are usually single-vessel atherosclerotic stenosis, while three-vessel lesions are rare. Coronary Atherosclerotic Heart Disease (CHD) refers to the heart disease caused by myocardial ischemia, hypoxia or necrosis due to the stenosis or occlusion of coronary vessel cavity. Long-term hormone therapy in SLE can reduce cholesterol conversion and significantly increase blood lipid. Hyperlipidemia is one of the main risk factors of coronary heart disease. Low Density Lipoprotein Cholesterol (LDL-C) and lipoprotein a [L p(a)] in blood lipids are independent risk factors of coronary heart disease, so the dual strict management of LDL-C and Lp(a) can bring more cardiovascular benefits. Pre-protein convertase subtilisin (PCK9) inhibitor is a kind of secreted protein derived from liver. It is found that PCK9 is positively correlated with LP(a) level, and statins combined with PCK9 inhibitor can effectively reduce blood lipid level.
Case presentation
The patient, a 45-year-old male, suffered from intermittent chest distress for more than 7 years, which worsened for 1 week. He have a history of hypertension for more than 4 years, and his blood pressure is up to 180/100 mmHg. After long-term oral treatment with Sacubitril Valsartan Sodium Tablets, his blood pressure can be controlled. At the same time, he has a history of diabetes for more than 7 years. He has used Dapagliflozin combined with Insulin to control his blood sugar for a long time, and his blood sugar control is satisfactory. He also has systemic lupus erythematosus and antiphospholipid antibody syndrome for more than 20 years, long-term use of “Rivaroxaban, Prednisone acetate tablets” and other drugs treatment, specific unknown. Since May 2020, the patient has experienced sudden chest tightness and discomfort after activity, showing paroxysmal symptoms without sweating, nausea or vomiting, and the symptoms can be relieved after the self-complaint containing quick-acting heart-saving pills. In July, 2020, the patient went to the local hospital for coronary angiography, and the results showed that the left anterior descending artery was narrow. A drug-eluting stent was implanted in the stenosis of the anterior descending branch (the details are unknown), and after the operation, he was treated with antiplatelet tablets of Clopidogrel Hydrogen Shlfate Tablets, anticoagulation with Rivaroxaban and lipid-lowering with Rosuvastatin. In November 2021, he went to our hospital again our hospital again for coronary angiography because of chest tightness. The results showed that the proximal stent of the anterior descending branch was narrow, the middle part of the artery were occlusive, and the lesions of the other multiple vessels were more serious. After treatments, he continued to strengthen antiplatelet therapy and statins to stabilize plaque, and symptoms occurred from time to time. In the past 1 week, the patient had no recurrent chest distress symptoms, no sweating, no nausea, vomiting, each lasting 10- 20min, which could be partially alleviated by the administration of nitric acid drugs, and was admitted to our department as “unstable angina pectoris of coronary heart disease” for further diagnosis and treatment.
There were no obvious abnormalities in the physical examination of the patient after admission. There were no abnormalities in blood routine examination, liver and kidney function, coagulation function, thyroid function, inflammatory index and immune index, and myocardial markers were negative. But his blood lipid level showed that TG 2.11 mmol/L, TC 2.56 mmol/L, LDL-C 0.58 mmol/L, Lp(a) 56.3 mg/dl. Looking back the results of previous blood lipid reexamination (November 2021 ~ April 2023), TG fluctuated from 0.91 to 2.24 mmol/L, TC from 2.80 to 4.81 mmol/L, LDL-C fluctuated from 1.22 to 3.06 mmol/L, and LP (a) was 53.0 to 58.4 mg/dl. His ECG: sinus rhythm 73 times / min, left anterior branch block, ST-T changes in V1 and V2 leads. His echocardiography: Ejection Fraction (EF) 52%, the universality of left ventricular myocardial motion weakened, and a small amount of mitral and tricuspid regurgitation. After admission, the patients were given Clopidogrel Hydrogen Shlfate Tablets 75 mg orally once a day, Rivaroxaban 15 mg orally orally once a day, Rifastatin 20 mg orally once a night, Ezetimibe 10mg orally orally once a day, Metoprolol succinate 23.75 mg orally orally once a day, Sacubitril Valsartan Sodium Tablets 50 mg orally twice daily, and Dapagliflozin 10 mg orally orally once a day.
Retrospective analysis showed that there was no obvious abnormality in immune indexes in the past, and SLE activity score was less than 10 points, which was considered as inactive stage of lupus. The results of coronary angiography in November 2021 showed that the proximal stent of anterior descending branch was stenosed, the middle segment of anterior descending branch was occluded, and TIMI blood flow was grade 0. The left circumflex branch is diseased in the whole process, with multiple stenosis of 70%-95%, stenosis of the proximal opening of the right coronary artery of 95%, and multiple stenosis of the posterior trigeminal branch of the middle and distal segment of 80%-95%, and TIMI blood flow is Grade 3 (Figure 1).
The results suggest that diffuse coronary lesions and severe stenosis may be caused by SLE. When he used statins alone, his blood lipid level was not well controlled. Therefore, he was given a treatment plan of strengthening antiplatelet, anticoagulation and lowering blood lipid. After intensive treatment of statins combined with ezetimibe for three months, the results of re- examination of blood lipids showed that LDL-C was significantly decreased, and the level of Lp(a) was still high, and he had intermittent episodes of ischemic symptoms such as chest tightness. Considering that the patients’ blood lipid level is still not well controlled, we added PCSK9 inhibitor on the basis of statins and ezetimibe treatment. After one month’s treatment, the blood lipid was rechecked, and the results showed that LDLC decreased more obviously, Lp(a) decreased by 19%, and the frequency and degree of myocardial ischemia symptoms also decreased significantly (Table 1). The patient was treated with intensive lipid-lowering and secondary preventive drugs for coronary heart disease for nearly two months, and there was no recurrence of ischemic symptoms during outpatient follow-up.
Discussion
Cardio Vascular Diseases (CVD) are currently the leading cause of human death [1].
Hyperlipidemia is one of the main causes of cardiovascular diseases, characterized by the increase of low density lipoprotein cholesterol (LDL-C). A large number of clinical trials have shown that cholesterol-lowering treatment can reduce the morbidity and mortality of cardiovascular diseases, so reducing LDL-C levels is the cornerstone of cardiovascular disease treatment [2]. The current guidelines for the management of dyslipidemia suggest that statin therapy should be optimized, and the low-density lipoprotein control target value of patients at risk of cardiovascular disease should be set at <1.8 mmol/L [3]. And a lot of research shows that [4-6], Even for patients with LDL- C <1.8 mmol/L, high Lp(a) is still a risk factor. Compared with LDL-C, Lp (a) can aggravate the occurrence and development of cardiovascular diseases by promoting thrombosis and inflammation. The patient in this case has a long history of SLE, with poor basic state of blood vessels and great brittleness. Therefore, the risk of coronary artery rupture and bleeding during surgery is high, and temporary drug conservative treatment is required. Patients achieved optimal LDL-C goals with moderateintensity statin therapy, but still experienced stent restenosis and myocardial ischemia, and Lp(a) levels were not controlled, leading to an increased risk of atherosclerotic thrombosis. For those whose LDL-C level has reached the ideal standard, but Lp(a) level has not been controlled to the standard, it is recommended to combine moderate intensity statins and ezetimibe therapy with preprotein converting enzyme subtilysin (PCSK9) inhibitors to reduce blood lipid significantly [7].
AIM-HIGH, JUPITER and LIPID study show that under the control of LDL-C, high Lp(a) level increases the risk of cardiovascular disease by promoting atherosclerosis, thrombosis and inflammation. The patient was given statins to control the blood lipid level after the first stent implantation, but it is unclear whether the blood lipid level of the patient reached the standard level. Through coronary angiography in the hospital, we found that stent restenosis and multi-vessel stenosis were serious, and the blood lipid level of patients was not up to standard after the first stent implantation, in which LDL-C was 2.75 mmol/L, Lp(a and LP(a) was as high as 56.1 mmol/L. It shows that the effect of single statins in controlling blood lipid level is slightly lacking, so the use of statins should be strengthened in treatment. After one year’s use of high-intensity statins, the reexamination of blood lipid showed that LDL-C was 3.06 mmol/L, Lp(a) was 58.4 mmol/L, and the blood lipid level was still not up to standard and increased, so statins and ezetimibe were combined for treatment. After three months of intensive treatment, the LDLC was 1.22 mmol/L and Lp(a) was 53 mmol/L, and the blood lipid level of the patient was significantly improved. According to the 2018 AHA Cholesterol Control Guidelines, the principle of LDL-C reduction is that the lower the better, and the 2019 ESC/EAS Guidelines for the Management of Dyslipidemia set the lipid control target for extremely high-risk patients as LDL-C < 1.4 mmol/L. After the patient was treated with statins combined with ezetimibe for 3 months, the LDL-C level had reached the ideal level, but the patient’s Lp(a) was still at a high level, and he had intermittent chest distress and discomfort, so PCSK9 inhibitor is added to the treatment. The results of the latest reexamination showed that LDL-C was 0.34 mmol/L and Lp(a) was 45.6 mmol/L. The blood lipid level of this case basically met the requirements after the use of PCSK9 inhibitors, and there was no recurrence of ischemic events in the patients during the recent two outpatient follow- up.
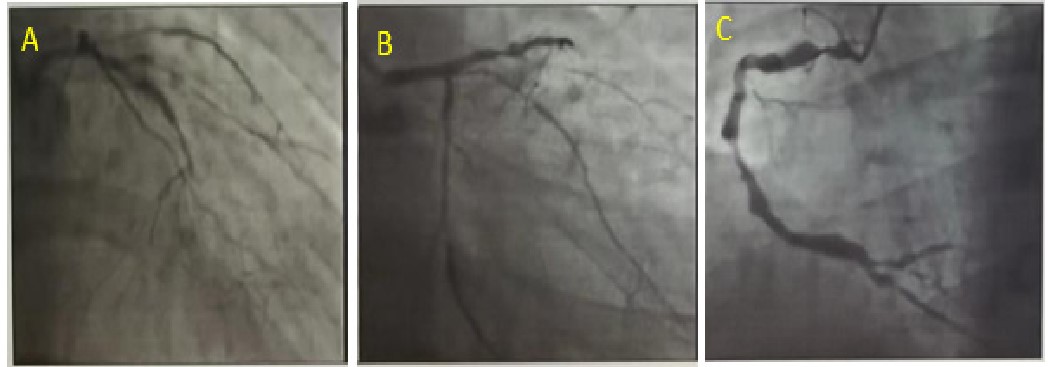
A: Left coronary head angiography.
B: Left coronary foot imaging.
C: Right coronary left anterior oblique imaging.
Table 1: Serum lipid level and treatment plan.
| Date | Blood lipids | Treatment | |
|---|---|---|---|
| Nov 9, 2021 | LDL-C 2.75 mmol/L, Lp(a) 56.1 mmol/L |
Rosuvastatin 10 mg | |
| Dec 18, 2022 | LDL-C 3.06 mmol/L, Lp(a) 58.4 mmol/L |
Rosuvastatin 10 mg | |
| Apr 18, 2023 | LDL-C 1.22 mmol/L, Lp(a) 53 mmol/L |
Rosuvastatin 10 mg + Ezetimibe 10 mg | |
| Aug 22, 2023 | LDL-C 0.58 mmol/L, Lp(a) 56.3 mmol/L |
Rosuvastatin 10 mg + Ezetimibe 10 mg + PCSK9 Inhibition 75 mg | |
| Sep 18, 2023 | LDL-C 0.34 mmol/L, Lp(a) 45.6 mmol/L |
||
Conclusion
The patient is a middle-aged male SLE, which not only has traditional cardiovascular risk factors such as diabetes and hypertension, but also has a high blood lipid level after long-term oral hormone therapy. His vascular disease is so serious that percutaneous coronary intervention is not feasible for the time being. Only statins combined with PCSK9 inhibitors can strictly control the blood lipid level, and the symptoms can be improved after controlling the risk factors. In view of SLE patients with coronary heart disease complicated with various risk factors, and the serious coronary artery stenosis can not be treated by interventional therapy, it is necessary to manage the blood lipid level and use the secondary preventive drugs of coronary heart disease reasonably and standardly so that the coronary artery stenosis will not be further aggravated, thus reducing the incidence of MACE events.
References
- Libby P. The changing landscape of atherosclerosis J. Nature. 2021; 592(7855): 524-533.
- Borén J, Chapman M J, krauss R M, et al. Low-density lipoproteins cause atherosclerotic cardiovascular disease: pathophysiological, genetic, and therapeutic insights: A consensus statement from the European Atherosclerosis Society Consensus Panel J. European heart journal. 2020; 41(24): 2313-2330.
- ESC/EAS guidelines for the management of dyslipidaemias: Lipid modification to reduce cardiovascular risk J. Atherosclerosis. 2019; 290: 140-205.
- Wilson D P, Jacobson T A, Jones P H, et al. Use of Lipoprotein(a) in clinical practice: A biomarker whose time has come. A scientific statement from the National Lipid Association J. Journal of clinical lipidology. 2022.
- Handelsman Y, Jellinger P S, Guerin C K, et al. Consensus Statement by the American Association of Clinical Endocrinologists and American College of Endocrinology on the Management of Dyslipidemia and Prevention of Cardiovascular Disease Algorithm-Executive Summary J. Endocrine practice: Official journal of the American College of Endocrinology and the American Association of Clinical Endocrinologists. 2020; 26(10): 1196-1224.
- Kronenberg F, Mora S, Stroes E S G, et al. Lipoprotein(a) in atherosclerotic cardiovascular disease and aortic stenosis: A European Atherosclerosis Society consensus statement J. European heart journal. 2022.
- Deedwania P, Murphy S A, Scheen A, et al. Efficacy and Safety of PCSK9 Inhibition With Evolocumab in Reducing Cardiovascular Events in Patients With Metabolic Syndrome Receiving Statin Therapy: Secondary Analysis From the Fourier Randomized Clinical Trial J. JAMA cardiology. 2021; 6(2): 139-147.