
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 5
Challenges in laryngeal mask ventilation: Case of a vocal cord polyp
Sangrà-Puig M; Tena B; Bergé R; Barranco de Santiago A; Garavito L; Magaldi M*
Department of Anaesthesiology, Hospital Clinic Barcelona, Barcelona, Spain.
*Corresponding Author : Marta Magaldi
Department of Anaesthesiology, Hospital Clinic
Barcelona, Barcelona, Spain.
Tel: 93-227-55-58;
Email: mmagaldi@clinic.cat
Received : Nov 19, 2024
Accepted : Dec 19, 2024
Published : Dec 26, 2024
Archived : www.jcimcr.org
Copyright : © Magaldi M (2024).
Abstract
Airway obstruction during the use of Laryngeal Mask Airway (LMA) devices is not uncommon. The most frequent causes are typically related to a superficial plane of anesthesia or misposition of the LMA. However, uncommon causes such as vocal fold polyps must also be considered, as they can significantly impact ventilation and complicate airway management. This case report presents a 53-year-old male patient scheduled for elective surgery, encountering unexpected difficulties during airway management due to a previously undiagnosed giant vocal cord polyp. Despite correct LMA placement, high peak airway pressures and persistent ventilation difficulties prompted further investigation using fiberoptic bronchoscopy, which revealed the vocal cord polyp as the source of obstruction. After a failed fiberoptic intubation through the LMA, the decision was made to awaken the patient to prevent a potentially dangerous “can’t intubate, can’t ventilate” scenario. Subsequently, awake fiberoptic intubation was successfully performed, securing the airway and allowing the procedure to continue without further complications. This case emphasizes the importance of thorough preoperative airway assessment, early recognition of airway difficulties and the strategic use of awake intubation techniques in complex airway management situations.
Keywords: Laryngeal mask; Difficult ventilation; Vocal fold polyp; Airway obstruction; Unexpected difficult airway.
Citation: Magaldi M, Sangrà-Puig M, Tena B, Bergé R, Barranco de Santiago A, et al. Challenges in laryngeal mask ventilation: Case of a vocal cord polyp. J Clin Images Med Case Rep. 2024; 5(12): 3402
Introduction
Laryngeal Mask Airway (LMA) is a widely used Supraglottic Airway Device (SAD) for airway management during general anaesthesia, especially in outpatient surgeries It has gained popularity over the past decades due to its ease of insertion, minimal invasiveness, and ability to maintain effective ventilation without the need for tracheal intubation [1]. These attributes make the LMA a preferred choice in a variety of clinical settings, especially in patients with low risk of difficult airway management. However, its insertion is performed blindly so problems related to misposition, or unnoticed glottic-subglottic obstruction may appear.
One such condition is the presence of large or obstructive lesions in the airway, such as vocal cord polyps, which can impair proper ventilation. These lesions may not only interfere with the correct positioning of the LMA but also pose a risk of airway obstruction, leading to difficulty in maintaining adequate ventilation [2]. There are several reported cases of difficult or impossible ventilation in patients with known polyps undergoing resection, but very few of previously undiagnosed polyps [3]. An obstruction caused by an undiagnosed vocal fold polyp during LMA ventilation is a rare but significant cause of difficult ventilation during general anesthesia. It requires prompt and targeted interventions for effective anesthetic management, as failure to address the obstruction can compromise airway permeability and patient safety [4].
This case report describes a rare situation of difficult ventilation through an LMA during general anesthesia caused by a giant vocal cord polyp. The patient’s airway obstruction, which was not anticipated preoperatively, resulted in significant challenges in securing effective ventilation.
Case presentation
A 53-year-old man with subacromial syndrome and no other significant previous medical history was scheduled for elective shoulder arthroscopy. While the airway assessment revealed a short thyromental distance and a Mallampati grade 3, all other parameters such as mouth opening, mandibular subluxation and neck extension were within normal limits.
The patient received 2 mg of midazolam as premedication, followed by an interscalene brachial plexus block prior to the induction of general anesthesia. Once in the operating room, baseline monitoring, including non-invasive blood pressure, oxygen saturation, and electrocardiogram were continuously recorded. General anesthesia was induced with a combination of fentanyl (1 mcg/kg) and propofol (2.2 mg/kg), followed by an infusion of remifentanil afterwards.
After induction, a Guedel airway was placed to optimize mask ventilation and a size 5 LMA Unique® (The Laryngeal Mask Company Ltd., UK) was inserted without difficulty using the standard technique. The correct positioning of the LMA was confirmed through bilateral lung auscultation, a normal capnography waveform and the absence of gastric insufflation during manual ventilation. However, upon initiating mechanical ventilation, elevated peak airway pressures over 30 cm H2O were observed, along with an air leak at 24 cm H2O. Despite deepening anesthesia with an additional bolus of propofol and administering 10 mg of rocuronium, no improvement was noted. The LMA was replaced with a size 5 LMA with gastric access to achieve a better seal, but difficult ventilation persisted, worsening over time. End- tidal CO2 levels increased to 55 mmHg, although oxygen saturation always remained above 97%.
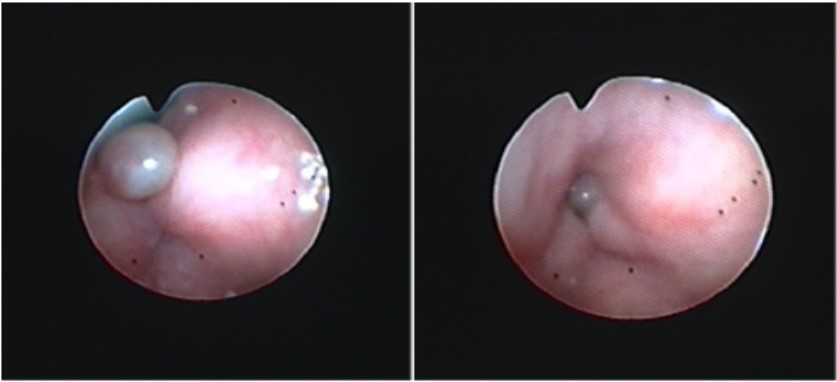
A Fiberscope (FBS) was then used to assess the LMA placement, revealing a large, previously undiagnosed white mass situated between the vocal cords, which appeared slightly edematous (Figure 1). After an unsuccessful attempt at fiberoptic intubation through the LMA, and considering the non-urgent nature of the surgery, the decision was made to awaken the patient to prevent a can’t-intubate-can’t-ventilate situation. The patient regained spontaneous ventilation without complication.
Subsequently, an awake fiberoptic intubation was performed, which revealed significantly inflamed vocal cords and a mobile vocal cord polyp causing a 50% obstruction of the glottis. A 7.5 mm endotracheal tube with a soft silicone tip was successfully passed without further complications and a dose of 125 mg of metilprednisolone was administered. The rest of the intraoperative course proceeded uneventfully, and the patient was carefully extubated in the operating room without further issues.
Discussion
This case shows an uncommon cause of airway obstruction when using a laryngeal mask due to previously undiagnosed anatomic abnormalities of vocal folds. It highlights the critical importance of thorough preoperative airway evaluation and the application of a well-defined difficult airway management algorithm during general anaesthesia.
Several factors can contribute to difficult ventilation with a LMA. Anatomical variations, such as a small oropharyngeal cavity, restricted neck mobility, or limited mouth opening, can hinder proper LMA placement and seal. Obstructive airway conditions, including masses like vocal cord polyps, airway tumors, or enlarged tonsils, may obstruct airflow and make ventilation challenging. Inadequate sizing or positioning of the LMA can lead to air leaks or improper alignment with the airway, resulting in poor ventilation. Additionally, excessive airway secretions or edema can impair the functioning of the LMA. Obesity and conditions associated with reduced lung compliance, such as pulmonary fibrosis or severe bronchospasm, can further complicate ventilation. However, only few predicting scores have been studied for validation [5,6].
Vocal fold polyps are well-localized lesions, often associated to phonotrauma, and with known risk factors as smoking, vocal abuse and pharingo-laringeal reflux. This explains their main signs being hoarseness, dysphonia and vocal fatigue, though these syntoms are present only in 11-15% of the patients [7]. In a study in South Korea, with almost 20000 participants, laryngoscopy found abnormalities in 1.96% of the population and vocal fold polyps were the second most prevalent abnormality, on 0.3-0.6% of the population, right after vocal nodules [8]. Although upper airway obstruction caused by laryngeal polyps is uncommon because they do not usually reach sufficient size to cause spontaneous airway obstruction, there have been some cases associated to sudden airway obstruction during its anaesthetic management [4,9,10]. Large and broader based polyps tend to obstruct the glottis, reducing the airflow, sometimes even during spontaneous breathing, caused by the polyp moving inwards and outwards during the breathing cycle [4].
While specific data on the prevalence of airway obstruction due to vocal fold polyps is limited [11], the occurrence is not negligible and should be considered as a potential cause of difficult ventilation. Symptoms such as hoarseness, voice fatigue, and dysphonia should be factored into the preoperative assessment, alongside other established predictors for difficult ventilation through a supraglottic airway device as the RODS acronym (Restricted mouth opening, Obstruction, Distorted airway and Stiff lung or cervical Spine). In this case, causes of potential difficult ventilation were not identified in the preoperative evaluation. Unfortunately, the undiagnosed vocal cord polyp, which caused significant obstruction during ventilation, was not detected preoperatively, leading to intraoperative difficulties.
Once difficult ventilation was encountered, the case further underscores the importance of following a structured difficult airway management algorithm.
The initial attempt at securing the airway with a Laryngeal Mask Airway (LMA) appeared successful based on standard confirmation methods, such as auscultation and capnography. However, elevated peak airway pressures and air leaks soon indicated a problem with ventilation, likely due to airway obstruction. More common causes of difficult ventilation such as superficial anesthetic plane, bronchospasm or misposition of the LMA were initially discarded. Nor deepening of anesthesia and muscle relaxing or reinsertion of a LMA with gastric access, that usually achieves a better sealing, improved ventilation. As the ventilation difficulties persisted, it became clear that an anatomical obstruction was the underlying issue. The use of a Fiberoptic Bronchoscope (FBS) proved to be crucial in identifying the source of the obstruction: a large, previously undiagnosed vocal cord polyp. Although FBS is not typically used for diagnostic purposes during anaesthesia management excepting for thoracic surgery, it can be crucial for identifying the cause of an obstruction and guiding an appropriate intervention. Awakening the patient after the failed attempt at fiberoptic intubation through the LMA was a prudent decision. In difficult airway situations, it is essential to recognize when to avoid escalating into a “can’t intubate, can’t ventilate” scenario, which carries a high risk of severe complications. The ability to safely awaken the patient allowed for a more controlled approach to securing the airway with an awake fiberoptic intubation. This strategy ultimately led to the successful placement of an endotracheal tube, ensuring safe ventilation for the remainder of the procedure. The administration of corticosteroids post-intubation to reduce vocal cord inflammation was an important step in minimizing the risk of postoperative airway complications, especially considering the significant obstruction caused by the polyp.
A more frequent but very different situation from our clinical case is when diagnosis is made before surgery and an adequate anesthetic management can be prepared [4]. Airway intubation would be the first choice to ensure ventilation overcoming the anatomic abnormality. If physically possible, the decision comes in choosing between video laryngoscope or fiberscope, both options being viable and widely reported in the literature, but as mentioned above, sometimes the polyp completely obstructs during anesthetic induction and spontaneously allows air to pass through instead. The optimal management of these situations involves close cooperation with the entire medical team prior to the intervention. In some instances, even a temporary tracheostomy may be considered if orotracheal intubation poses significant risks [12]. Another reported, uncommon cause is aryepiglottic folds positioned over the vocal cords because of LMA placement, requiring extraction of the LMA and laryngoscopy to diagnose the obstruction and posterior introduction of an endotracheal tube [13].
In conclusion, this case underscores several key points in airway management during general anesthesia. First, a thorough preoperative airway assessment is essential, especially in patients with risk factors for difficult ventilation or intubation. Second, the importance of a structured difficult airway algorithm cannot be overstated, as it provides a clear framework for managing unexpected complications [14-16]. Lastly, timely identification of airway obstructions and careful decision-making, including the option to awaken the patient, if necessary, are crucial in ensuring patient safety and avoiding potentially life-threatening complications.
Conclusions
Vocal fold polyps are an uncommon, but possible cause of obstruction during anaesthesia airway management.
Hoarseness, vocal fatigue and dysphonia are signs indicating possible vocal cords abnormalities.
If previously known, an adequate anaesthetic management can be prepared.
Both laryngoscopies, direct or through video, and fibreoptic bronchoscopy are useful to determine the cause of the airway obstruction.
The application of a well-defined difficult airway management algorithm is crucial to assure a good outcome in this critical situation.
Declarations
Conflicts interest: conflicts of interest to disclose.
Funding: There are no financial relationships.
Author contributions: This paper is not under consideration elsewhere, and the contents have not been previously published. All the authors have contributed significantly to the submitted work and have read and approved the final version of this manuscript.
References
- Hummel R, Wollschläger D, Baldering HJ, et al. Big data: Airway management at a university hospital over 16 years; a retrospective analysis. PLoS One. 2022; 17(9): e0273549. doi:10.1371/ journal.pone.0273549.
- Fuseya S, Ichino T, Tanaka S, Ishida K, Ishida T, et al. Airway obstruction due to a laryngeal polyp following insertion of a laryngeal mask airway. JA Clin Rep. 2018; 4(1): 43. doi:10.1186/ s40981-018-0180-3
- D’Hulst D, Butterworth J, Dale S, Oaks T, Matthews B. Polypoid hyperplasia of the larynx misdiagnosed as a malpositioned laryngeal mask airway. Anesth Analg. 2004; 99(5): 1570- 1572. doi:10.1213/01.ANE.0000134802.08319.CF.
- Kour, Arvin Preet, Singh, Ajaydeep. Large Vocal Cord Polyp and Anesthetic Considerations: A Case Report. Apollo Medicine. 2023; 20(Suppl 2): S49-S51. DOI: 10.4103/am.am_141_22.
- Saito T, Chew ST, Liu WL, Thinn KK, Asai T, et al. A proposal for a new scoring system to predict difficult ventilation through a supraglottic airway. Br J Anaesth. 2016; 117(Suppl 1): i83-i86. doi: 10.1093/bja/aew191.
- Saito T, Asai T, Taguchi A, Sophia CTH, Liu W, et al. Prediction of failed facemask ventilation: new scoring system for difficult airway. J Anesth. 2020; 34(3): 367-372. doi: 10.1007/s00540-020-02761-3.
- Vasconcelos D, Gomes AOC, Araújo CMT. Vocal Fold Polyps: Literature Review. Int Arch Otorhinolaryngol. 2019; 23(1): 116-124. doi:10.1055/s-0038-1675391.
- Woo SH, Kim RB, Choi SH, Lee SW, Won SJ. Prevalence of laryngeal disease in South Korea: data from the Korea National Health and Nutrition Examination Survey from 2008 to 2011. Yonsei Med J. 2014; 55(2): 499-507. doi:10.3349/ymj.2014.55.2.499.
- Pandey R, Garg R, Kumar A, Darlong V, Punj J, et al. Case report: Airway management of a patient with popping pedunculated subglottic laryngeal polyp. Acta Anaesthesiol Belg. 2009; 60(4): 251-253.
- Kurwe MS, Karim HMR, Mehta R, Nene Y. Lessons Learned from A Case of Functional Total Laryngeal Obstruction Under Anaesthesia by Vocal Cord Polyp Managed by Vortex Approach. Turk J Anaesthesiol Reanim. 2021; 49(2): 175-177. doi:10.5152/ TJAR.2021.64.
- Ahmad SM, Soliman AM. Airway obstruction: A rare complication of benign vocal fold polyps. Ann Otol Rhinol Laryngol. 2008; 117(2): 106-109. doi:10.1177/000348940811700206.
- Dubreuil M, Janvier G, Dugrais G, Berthoud MC. Uncommon laryngeal mask obstruction. Can J Anaesth. 1992; 39(5 Pt 1): 517-518. doi:10.1007/BF03008726.
- Jeong HW, Song EJ, Jang EA, Kim J. Managing a difficult airway due to supraglottic masses: Successful videolaryngoscopic intubation after induction of general anesthesia. Perioper Med (Lond). 2024; 13(1): 21. doi:10.1186/s13741-024-00377-9.
- Valero R, Orrego C, Mayoral V, Massó E, et al. Quava Group. Collaborative intervention to improve airway assessment and safety in management for anaesthesia: the Qualitat & Via Aèria (QUAVA) study. Eur J Anaesthesiol. 2014; 31(3): 143-52. doi: 10.1097/EJA.0000000000000006.
- Apfelbaum JL, Hagberg CA, Connis RT, Abdelmalak BB, Agarkar M, et al. American Society of Anesthesiologists Practice Guidelines for Management of the Difficult Airway. Anesthesiology. 2022; 136(1): 31-81. doi: 10.1097/ALN.0000000000004002.
- Frerk C, Mitchell VS, McNarry AF, Mendonca C, Bhagrath R, et al. Difficult Airway Society 2015 guidelines for management of unanticipated difficult intubation in adults. Br J Anaesth. 2015; 115(6): 827-48. doi:10.1093/bja/aev371.