
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Research Article - Open Access, Volume 5
Four different laparoscopic surgical techniques to close the gallbladder remnant/stump after a partial cholecystectomy for Mirizzi syndrome
Fahri Yetisir*
General Surgery Department, VM Medical Park, Ankara Private Hospital, Yüksek İhtisas University, Ankara /Turkey.
*Corresponding Author : Fahri Yetişir
General Surgery Department, VM Medical park
Ankara Private Hospital, Yüksek İhtisas University,
Ankara /Turkey
Tel: +90-536-297-48-88 & 03123210089;
Email: drfahriyetisir@hotmail.com
Received : Sep 09, 2024
Accepted : Dec 19, 2024
Published : Dec 26, 2024
Archived : www.jcimcr.org
Copyright : © Yetişir F (2024).
Abstract
Objective: Mirizzi syndrome is known as extrinsic bile duct compression syndrome. A longstanding impacted gallstone in the Hart- mann’s pouch can cause a compression to the adjacent bile duct and due to this compression, a pressure ulceration and inflammation occurred consecutively. These recurrent ulcerations and inflammations can cause the bile duct obstruction. Cholecystobiliary fistula may present with different degrees and it is classified five types according to the fistula’s degrees. Surgical management is the mainstay treatment for Mirizzi syndrome. Recently, although more experts reported the minimally invasive surgical techniques with high success rate, open surgery has been chosen as the mode of treatment. We operated twenty-one patients with Mirizzi syndrome by using four different laparoscopic surgical techniques to close the gallbladder remnant/stump after a partial cholecystectomy over the last eleven years. The aim of this study was to report our results and describe these four different laparoscopic approaches for the treatment of all type of Mirizzi syndrome.
Methods: Between August 2010 and March 2021, 582 patients with gallbladder disease were operated. Twenty-one of them confirmed intraoperatively as Mirizzi syndrome were included in this study. A retrospective evaluation of these patients was performed.
Results: All of the 21 patients with all types of Mirizzi syndrome were treated by these 4 different novel laparoscopic surgical techniques with 5% conversion rates and no mortality. Bile leak developed in only one patient and it was resolved after one week.
Conclusion: These four different laparoscopic surgical techniques are safe and feasible to treat Mirizzi syndrome by an experienced laparoscopic surgeon.
Keywords: Mirizzi syndrome; Subtotal cholecystectomy; Cholecystobiliary fistula; Cholecystocholedochal fistula.
Abbreviations: ASA: American Society of Anesthesiologists; BD: Bile Duct; CTT: Closure over T-Tube Technique; CT: Computed tomography; ERCP: Endoscopic retrograde Cholangiopancreatography; EST: Excision by staple technique; EHST: Excision and handmade Suturation technique; LSC: Laparoscopic subtotal cholecystectomy; LS: Laparoscopic surgery; MRCP: Magnetic resonance Cholangiopancreatography; MS: Mirizzi syndrome; PST: Purse stitch technique; US: Ultrasound.
Citation: Yetişir F. Four different laparoscopic surgical techniques to close the gallbladder remnant/stump after a partial cholecystectomy for Mirizzi syndrome. J Clin Images Med Case Rep. 2024; 5(12): 3403.
Introduction
Background: Mirizzi Syndrome (MS) is an uncommon complication of longstanding gallstone disease and it is known as extrinsic compression syndrome of the Bile Duct (BD) [1]. MS is identified in 0.06-5.7% of patients during cholecystectomy [2]. It was first described by Kehr and by Ruge as a rare form of obstructive jaundice caused by external obstruction of the BD by impacted gallstone in the cystic duct in early 1900s. However, the condition was named as MS after Pablo Mirizzi in 1948, who defined it as extrinsic compression of the BD by a gallstone in the cystic duct or gallbladder neck [3,4-6]. This impacted gallstone causes compression of the adjacent bile duct, this compression can lead to occur pressure ulceration and local inflammation resulting in partial or complete obstruction of the BD [1]. After that, further erosion into the bile duct can cause to the development of a cholecystobiliary fistula with different degrees [6-9]. Classifications of MS have been made on the presence of the cholecystobiliary fistula and its degrees by McSherry’s and Csendes’ [3]. McSherry classified the MS as two types based on ERCP findings. The extrinsic compression of the common bile duct by an impacted gallstone without a cholecystobiliary fistula was defined as type-I and with fistula was defined as type-II MS [1,7,10,11]. Later in 1989, Csendes classified the MS in four types based on the size of the fistula in relation to the circumference of the BD [3]. In 2007, at the presence of the bilioenteric fistula, ıt is classified as type-V. All types of this last classification is explained in Table 1 with scheme [1,6]. The last modified classification of MS was used in this study.
Pre-operative diagnosis of MS is also challenging. There are no pathognomonic signs or symptoms. The clinical presentation of MS ranges from asymptomatic to non-specific symptoms such as right upper quadrant abdominal pain (16.7-100%), obstructive jaundice (27.8-100%), fever, nausea, vomiting, diarrhea and constipation. They can also occur during acute cholecystitis, pancreatitis, and choledocholithiasis [9,12]. MS may also present with gallstone ileus and may be easily confused with biliary tract neoplasm [2,7,12]. For the pre-operative diagnosis, especially abdominal Ultrasound (US), Computed Tomography (CT), Magnetic Resonance Cholangiopancreatography (MRCP), and Endoscopic Retrograde Cholangiopancreatography (ERCP) can be used. The Percutaneous trans-hepatic cholangiography may be used as an option in cases where ERCP failed [2]. Preoperative diagnosis of MS is based on clinical features, a high index of suspicion, or surgical intuition, which can be accompanied with radiologic imaging test [1,9,12].
Current evidence surgical management is only option for the treatment of the MS. Laparoscopic Surgery (LS) is not recommended for the management of MS. LS can be harmful due to the presence of severe local inflammation, fibrosis and adhesions within Calot’s triangle [6]. They still recommend open cholecystectomy for the management of MS [7,13]. Some authors claim that LS can be applied for type-I MS only [14-17]. However, other authors showed that combined pre-operative ERCP and laparoscopic subtotal cholecystectomy (LSC) [6,18,19] can be useful for the treatment of MS [6].
We operated twenty-one patients with MS which including all five types by using four different laparoscopic surgical techniques over the last eleven years. The aim of this study was to report our results and describe these four different laparoscop- ic surgical approaches for the treatment of MS.
Material and methods
Retrospective evaluation of the 582 consecutive patients who operated due to gallbladder disease between August 2010 and April 2022 was performed. 21 of them confirmed as MS by preoperative and/or intraoperative evaluations and were included in this study for further analysis. Ethical approval was not needed for this study. All operations were performed by single surgeon. Seven patients (3 of them have gallbladder cancer and 4 of them have more III ASA score) were not included in this study. All patients were evaluated with pre-operative bilirubin level and imaging test; preoperative and intraoperative US, MRCP and ERCP. Pre-operative demographic information, intra-operative findings and post-operative outcomes were collected. Conversion ratio, post-operative complications, operation time and length of post-operative hospital stay were recorded.
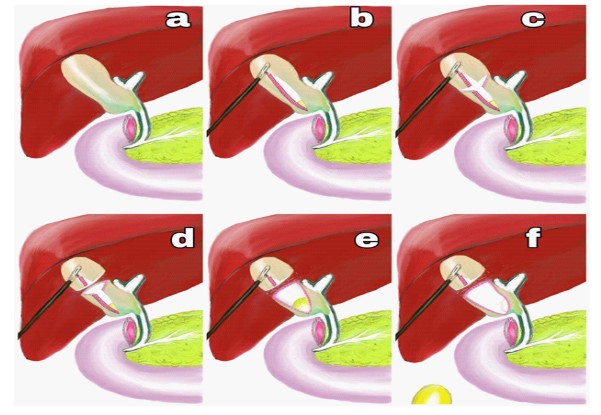
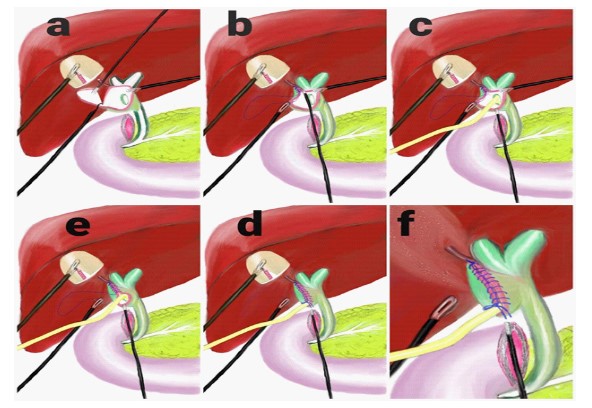
Surgical technique: Patient was positioned in supine position. The surgeon and first assistant were standing on left side of the patient. A 10 mm 30° scope was sited through the abdominal wall from the umbilical port. 12 mm port was inserted from the epigastrium and two 5 mm port also inserted from right subcostal margin. Patient was positioned 30 degrees head up and right sided position. First of all the intra-abdominal space was explored. The omentum, colon and other abdominal structure were separated by gentile dissection and liver was elevated by only pushing up from gallbladder. If there were any suspicious about the diagnosis, intraoperative US was used. For the MS with type 5, resection of cholecystoenteric fistula was performed by tri stable (Endo GIA™ 30 mm Reload with Tri-Staple™ Technology) by taking care not to narrow lumen of them. Grasper could not grasp from fundus of gallbladder due to dens fibrotic structure of it (Figure 1a). When no further dissection was possible within Calot’s triangle, gallbladder was perforated from fundus and emptied inside by aspirating. After that by grasping from the fundus, gallbladder was retracted. By using hook diathermy, a longitudinal incision was created from the fundus to up to the infundibulum of gallbladder (Figure 1b). By a second transvers incision between fundus and Hartmann’s pouch, gallbladder was divided into two separate parts (Figure 1c,d). Impacted stones within Hartmann’s pouch were removed (Figure 1e,f). By gentle and careful dissection of Hartmann’s pouch was continued like fundus down cholecystectomy as much as possible. In cases with a frozen hilum, dissection was not continued too much not to cause damage to the right hepatic duct, common bile duct and hepatic artery. It is not strictly necessary to obtain a critical view of Calot’s triangle. Some part of the Hartmann’s pouch was separated from liver posteriorly. During this dissection, so much care must be taken not to damage to the gallbladder wall also. Because this gallbladder wall of Hartmann’s pouch will be used as a flap for the reconstruction of fistula. To be able to make well saturation, if necessary additional one more 5 mm port also can be inserted from left side of the patient. All the operation up to this part similar in all four techniques. After this stage we applied 4 different laparoscopic surgical techniques according to the type of MS and the condition of the gallbladder wall.
Purse stitch technique (PST): Internal suturation of cystic duct with purse stitch (3/0 prolene® Polypropylene Suture-Ethicon): We use two rows of stitch to close the lumen of the cystic duct. The Mucosal surface of remnant gallbladder was destroyed by spray form of cautery (valleylab covidien). This technique can be applied to only Type-I MS (Figure 2a-d).
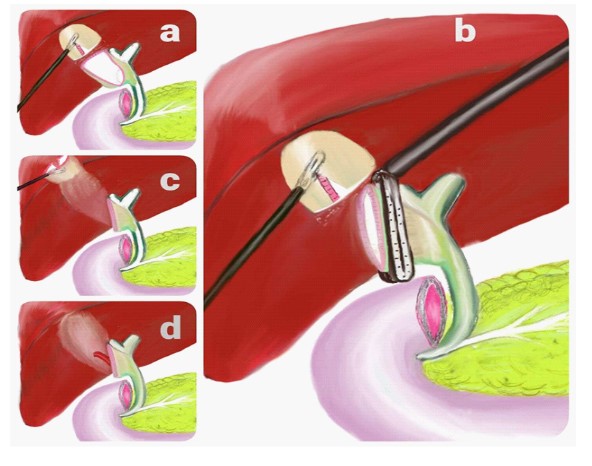
Excision by staple technique (EST): Excising from the infundibulum of gallbladder by tri-staple (Endo GIA™ Black Reload with Tri-Staple™ Technology). The Hartmann’s stump is closing while excising from the infundibulum of gallbladder by tri-staple. This technique can be applied to all types of MS. It is the easiest and shortest technique. The thicknesses of gallbladder wall must be suitable (Figure 3a-d). If the gallbladder wall is thicker or perforated during dissection, this technique cannot be applied.
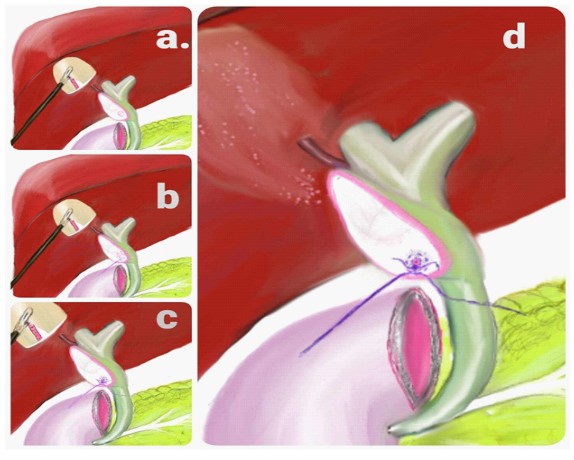
Excision and handmade suturation technique (EHST): Excising from infundibulum and closing by handmade suturation: This technique can be applied to all types of MS. It takes more time than first two techniques. This surgical approach was preferred if first two techniques were not suitable. Extra 5 mm port was used in this approach. (Figure 4a-f).
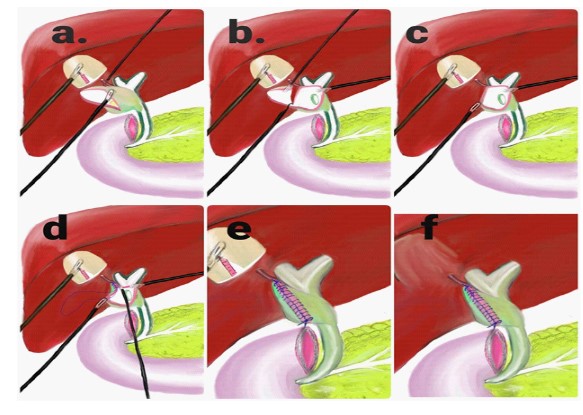
Closure over T-Tube technique (CTT): Closure of the BD defect by using gallbladder wall over T tube. This technique can be applied MS type III-V. This technique was preferred if papillotomy could not be done before by ERCP and if we were not sure about clearance of BD from gallstones fragment. This technique takes longer time and it is hardest one. Follow up of this technique is longer than the others and patient has to live with a drain for 7 weeks. Extra 5 mm port was used in this approach (Figure 5a-f).
In all four techniques, after performing good hemostasis, all repaired hepatobiliary system was careful checked for leak. Subtotal cholecystectomy was completed by resecting the remaining fundus part of gallbladder at the end of operation. Until that time fundus part was used for liver retraction in all surgical techniques. Two intra-abdominal drains were placed to all patients, one to the sub-hepatic space and one to the suprahepatic space.
Follow up: Oral intake was started at first day as a liquid diet for all patients. If there was no problem oral intake was increased day by day. All the drain was controlled every day in terms of amount and content. If there was no leak sing and the amount of drain decreased under to 20 cc, drain was removed. If bile leak continued more than one day over 100 cc amount from the drain, ERCP was applied. Patients were controlled postoperatively at 10. day, 1. Month, 3. Month and 6. Month. When T-Tube was used, a tubogram was performed 6 weeks after surgery to evaluate the anatomy. If there was no problem with bile passage and no bile leak sign, T-tupe was clamped for one week and after that it was removed.
Results
Between August 2010 and April 2022, 676 patients were operated due to gallbladder disease. 24 of them confirmed as MS and were included in this study. The mean age was 52.9±19.9 years old. The male to female ratio was 11/13. Pre-operative patient’s evaluation according to the American Society of Anesthesiologists (ASA) classification was as follows: ASA 1 (n=9), ASA 2 (n=10) and ASA 3 (n=5). The distribution of patients in this study according to the type of MS were as follows ten patients type-I, six patients type-II, two patients type-III, one patient type-IV and five patients type-V MS (Table 1).
Almost all of them (23/24) have previous history of abdominal pain for several times. Pre-operative imaging studies included US (n=24), MRCP (n=20), and ERCP (n=17) were performed in this study. 16(66%) patients were diagnosed as MS pre-operatively. In our series the sensitivity for preoperative diagnosis of MS was 29.2% for pre-operative US, 80% for intraoperative US, 70% for MRCP and 64.7% for ERCP (Table 2).
All twenty-one patients underwent LSC or near total cholecystectomy after extraction of impacted stones. Two of the 21 patients required conversion to open surgery (one of them due to make safer repair of duodenal fistula, other one due to the big choledochal fistula. Conversion ratio of this study is 9.5% (1/21). The mean length of hospital stay was 3.24±1.99 days. The mean length of operation time was 185.9±60.9 minutes (Table 2). All applied surgical technique to our patients were as fallows; 6 by PST, 8 by EST, 5 by EHST and 2 by CTT (Table 1). Stents had been placed in seven of them pre-operatively by ERCP. Post-operatively 100-150 cc daily bile leak occurred in one patient (4.7%). A papillotomy and extraction of gallstone fragment by ERCP was applied to this patient. After 4 days bile leak was stopped. Wound infection was developed in two patients. By using antibiotic and local wound care infections of both cases were resolved. One patient in CTT group was developed obstructive jaundice after 3 months, a stent was placed by ERCP to this patient. All complications were resolved with no problem in a short time.
Discussion
The exact incidence of MS is not well-known because asymptomatic cases may go undetected [6]. The incidence of MS among patients with symptomatic gallbladder disease is 0.05- 2.7% in developed countries [6,8] and 4.7-5.7% in developing countries [6,9,13]. In our series, the incidence of MS was 3.6 % (21/582). Imaging test is not so sensitive for MS. Because of that pre-operative diagnosis of MS is challenging [9]. In our series, pre-operative diagnosis rate was 52.3%. US is used as a routine imaging test during the evaluation of biliary disease. US can give evidence of MS such as an atrophic and edematous gallblad- der or ectatic common hepatic duct with a normal distal BD [17]. Sensitivity of US is between 8.3% and 77.8% [9,15,17-19]. In our series US has 14.3% sensitivity preoperatively and 50 % intraoperatively. In the recent literature, ERCP with the highest sensitivity is considered as a gold standard diagnostic tool for the diagnosis of MS (55%- 90%) [6,8,9,15,17,18]. Preoperatively therapeutic decompression with papillotomy and stent can be achieved by ERCP also. Preoperative placed stent facilitate LS of MS. ERCP can be also used in order to solve the hazardous complication such as bile leak and stricture of BD postoperatively, as we did. MRCP is commonly used as it is noninvasive and has a high sensitivity, similar to ERCP (50-90%) [6,9]. Cui at al report that, diagnosis of MS is increasing to 85.9% [17] when MRCP and ERCP were used in combination. In our series, MRCP was more sensitivity imaging tool with 58.9% success and ERCP had 46%, 2 sensitivity.
Pre-operative diagnosis is very important for optimum surgical therapy of MS, allowing better planning [2,6,8,9,20] and transferring the patient to the appropriate hospital and surgeon. Although more advanced cases of disease are easier to detect, such diagnosis is often missed preoperatively [2]. If diagnosis of MS is not achieved pre-operatively, intra-operative recognition and proper management are essential to reduce morbidity and mortality [6,15]. The intra-operative diagnosis of MS is not easy also. Because dissection of these longstanding chronically inflamed tissue with so much fibrosis and adherence is challenging and it make the visualization of the hepatic hilum anatomy more and more difficult [9]. Many patients with MS are diagnosed intraoperatively [10]. There are some signs of MS during surgery, such as an edematous or atrophic gallbladder with distortion of Calot triangle, an impacted gallstone in the infundibulum, thick fibrosis around Calot triangle, and adhesions under the liver space. If bile is coming after extraction of an impacted stone, this is a strong sing for BD fistula. Further intraoperative cholangiography and US can also be used to identify MS [2,3]. If one surgeon makes the diagnoses as MS intraoperatively and who does not have sufficient expertise on LS, what can be done? In my opinion, 1) If possible, another surgeon with sufficient expertise can be invited to operation 2). If surgeon has adequate experience on open hepatobiliary surgery, operation can be converted to open surgery, 3) If these two options are impossible, operation can be stopped at that phase and by placing drains patient can be transferred to appropriate surgeon and hospital urgently.
In our series, first, two incisions (longitudinal and transvers) to gallbladder were made and impacted stone was extracted. A little gentle dissection of Hartmann’s pouch was performed like as fundus down dissection as much as possible (Figure 1a-f). After that, we had to choose one of the four surgical techniques. If there was no BD fistula and the diameter of the cystic duct was not so large, we preferred to use PST cystic duct (n: 6) (Figure 2a-d). This technique is cheapest and easiest one. If dissected gallbladder wall was enough and suitable, EST was used (n=8) (Figure 3a-f). This technique is easiest one and it can be applied all type of MS, if the gallbladder wall is suitable. If there was a bile duct fistula and one side of gall bladder wall was destroyed during dissection, EHST was applied (n=5) (Figure 4a-f). If patients had been referred after stent placement by ERCP, closure of the BD was performed over the pre-existing stent. If there was large bile duct fistula, destroyed one side of gallbladder wall and the papillotomy had not been done before by ERCP, CTT was applied (n=2) (Figure 5a-f). This technique takes longer time and it is hardest one.
Up to now there is no standard treatment in the literature for MS. Surgical management is the mainstay treatment for MS, although this is challenging for several reasons. Treatment is often dependent on the available surgical expertise and type of MS [6,13]. It is very important to improve a clear treatment guideline modality for it [2]. Primary goal during the treatment is not to damage bile duct and hepatic artery during dissection of densely adhered fibrous tissue and proper reconstruction of the external bile ducts. Subtotal cholecystectomy leaving a suitable wall piece from Hartmann’s pouch of remaining gallbladder for the reconstruction of the defect of bile duct is one of the most acceptable approaches for MS with fistula. During this reconstruction a T-Tube may be used to avoid post-operative strictures or bile leakages [6]. For a MS with type 3 and type-IV, if the reconstruction of the bile duct cannot achieved by surrounding tissues, bilioenteric anastomosis may be needed [6,20].
In last decade, although more experts have made reported minimally invasive surgical techniques with high success rate, open surgery has been chosen as the mode of treatment [2]. Laparoscopic management of complex MS has not been suggested due to high risk of BD injury (up to 22%) and high conversion rates to open surgery (11.1-80%) [2,7,9,15,18,19 21,22]. On the other hand, some experts continue to recommend LSC for all type of MS [2,14,16]. Some authors reported robot assisted techniques in the treatment of MS [23-25]. They say that robot- assisted systems can provide better visualization with a three- dimensional camera and surgeons can do fine-tissue manipulation by it. They thought that the robot-assisted technique is safe and feasible for all type of MS, without partial cholecystectomy [6,25]. In my opinion, there is no sense of touching by robotic surgery and it is so expensive. In our series LS was applied safely to all types of MS with 5% conversions rate. One patient had a bile leak during the postoperative period that resolved after ERCP. We thought that management of MS is not easy in both laparoscopic and open surgery also. We recommend that these four different laparoscopic surgical techniques for appropriate patients can be applied safely if it is performed by experienced surgeon.
Table 1: (Classification) Mirizzi syndromeon scheme and patients distribution on types of MS with surgical technique with postoperative complication.
| Mirizzi type | Definition | Scheme | Surgical technique | Complication | |
|---|---|---|---|---|---|
| I | External compression of the bile duct by a stone impacted in the infundibulum of the gallbladder or cystic duct |  |
N | ||
| 7 | PST | ||||
| II | Cholecystobiliary fistula involving less than a third of the circumference of the bile duct |  |
3 | EST | |
| 3 | EHST | 1 Leak | |||
| III | Fistula involving up to two thirds of the circumference of the duct |  |
1 | EHST | |
| 1 | CTT | 1 Stricture | |||
| IV | Cholecystobiliary fistula with complete obstruction of the bile duct |  |
1 | CTT | C |
| V |
It includes the presence of a cholecystoenteric fistula along with any other Mirizzi Va: without gallstone ileus Vb: with gallstone ileus |
 |
4 | EST | 1 WI |
| 1 | EHST | 1 WI/C | |||
PST: Purse Stitch Technique; EST: Excision by Staple Technique; EHST: Excision and Handmade Suturation Technique; CTT: Closure over T-Tube Technique; WI: Wound Infection; C: Conversion; N: Number of patients.
Table 2: Preoperative, operative and postoperative data of all patients.
| Age | Sex | ASA score | Bilirubin level (mg/dL) | MRCP | ERCP | Preoperative diagnosis | Intraoperative US | Type of MS | Enteric part of Biliodigestive fistula | Surgical technique | Operation time | Hospital stay | Conversion and complication |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 50 | Male | 2 | 3,20 | + | + | + | + | II | EST | 210 | 2 | ||
| 78 | Female | 3 | 1,40 | + | + | + | + | V | duodenum | EHST | 240 | 8 | C/WI |
| 57 | Female | 2 | 2,10 | + | + | + | + | II | EST | 150 | 2 | ||
| 23 | Male | 1 | 2,40 | + | + | + | + | V | colon | EST | 250 | 3 | |
| 25 | Male | 1 | 3,40 | + | + | + | + | I | EST | 140 | 2 | ||
| 74 | Female | 3 | 5,70 | + | + | + | + | III | CTT | 290 | 4 | Stricture | |
| 77 | Female | 3 | 3,20 | + | + | + | + | I | EST | 170 | 2 | ||
| 80 | Female | 2 | 3,10 | + | + | + | + | I | PST | 140 | 6 | ||
| 69 | Female | 2 | 1,30 | + | + | + | + | V | stomach | EST | 280 | 6 | |
| 45 | Male | 1 | 1,90 | + | + | + | + | III | EHST | 110 | 1 | ||
| 28 | Male | 1 | 1,90 | + | + | + | + | I | PST | 145 | 1 | ||
| 66 | Female | 2 | 2,30 | + | + | + | + | I | EHST | 160 | 5 | ||
| 27 | Male | 1 | 1,80 | + | + | + | + | I | EST | 135 | 2 | ||
| 44 | Female | 2 | 2,30 | + | + | + | + | I | EHST | 210 | 9 | Leak | |
| 38 | Female | 1 | 1,80 | + | + | + | + | I | PST | 120 | 1 | ||
| 55 | Male | 2 | 2,10 | + | + | + | + | I | PST | 145 | 2 | ||
| 61 | Female | 2 | 1,80 | + | + | + | + | I | PST | 105 | 5 | ||
| 42 | Female | 2 | 1,40 | + | + | + | + | II | EHST | 185 | 6 | ||
| 71 | Female | 3 | 3,20 | + | + | + | + | IV | CTT | 230 | 9 | C | |
| 74 | Female | 3 | 1,90 | + | + | + | + | V | colon | EST | 310 | 8 | WI |
| 48 | Female | 2 | 2,60 | + | + | + | + | I | PST | 180 | 3 | ||
| 49 | Male | 2 | 1,90 | + | + | + | + | I | PST | 160 | 4 | ||
| 49 | Female | 2 | 3,5 | + | + | + | + | II | EST | 220 | 5 | ||
| 65 | Male | 2 | 2.8 | + | + | + | + | V | Duodenum | EST | 240 | 7 |
PST: Purse Stitch Technique; EST: Excision by Staple Technique; EHST: Excision and Handmade Suturation Technique; CTT: Closure over T-Tube Technique; WI: Wound Infection; C: Conversion; N: Number of patients.
Conclusion
The laparoscopic approach can be applied safely in all types of Mirizzi syndrome if the surgeon is highly proficient on laparoscopic surgery. Preoperative diagnosis is very important to guide the patients to suitable surgeons in a correct time. These four novel different laparoscopic surgical techniques are safe and feasible to treat all types of Mirizzi syndrome by choosing correct surgical technique to correct type of Mirizzi syndrome.
References
- Valderrama-Treviño AI, Granados-Romero JJ, Espejel-Deloiza M, Chernitzky-Camaño J, Barrera Mera B, et al. Updates in Mirizzi syndrome. Hepatobiliary Surg Nutr. 2017; 6(3): 170-178. doi: 10.21037/hbsn.2016.11.01.
- Chen H, Siwo EA, Khu M, Tian Y. Current trends in the management of Mirizzi Syndrome: A review of literature. Medicine (Baltimore). 2018; 97(4): e9691. doi: 10.1097/ MD.0000000000009691.
- Csendes A, Diaz JC, Burdiles P, Maluenda F, Nava O. Mirizzi syndrome and cholecysto-biliary fstula: A unifying classifcation. Br J Surg. 1989; 76: 1139-1143.
- Ruge E. Deitrage zur chirurgischen anatomie der grossen galenwege (Ductus hepaticus, choledochus, und pancreaticus). Arch Clin Chir. 1908; 78: 47.
- Mirizzi PL (1948) Síndrome del conducto hepático. J Int Chir. 1948; 8: 731-777.
- Senra F, Navaratne L, Acosta A, Martínez-Isla A. Laparoscopic management of type II Mirizzi syndrome. Surg Endosc. 2020; 34(5): 2303-2312. doi: 10.1007/s00464-019-07316-6.
- Antoniou SA, Antoniou GA, Makridis C. Laparoscopic treatment of Mirizzi syndrome: A systematic review. Surg Endosc. 2010; 24(1): 33-39.
- Payá-Llorente C, Vázquez-Tarragón A, Alberola-Soler A, Martínez-Pérez A, Martínez-López E, et al. Mirizzi syndrome: A new insight provided by a novel classification. Ann Hepato-Biliary- Pancreatic Surg. 2017; 21(2): 67-75.
- Beltrán MA. Mirizzi syndrome: history, current knowledge and proposal of a simplified classification. World J Gastroenterol. 2012; 18(34): 4639-4650.
- Safioleas M, Stamatakos M, Safioleas P, et al. Mirizzi Syndrome: an unexpected problem of cholelithiasis. Our experience with 27 cases. Int Semin Surg Oncol. 2008; 5: 12. 10.1186/1477- 7800-5-12.
- Kwon AH, Inui H. Preoperative diagnosis and efficacy of laparoscopic procedures in the treatment of Mirizzi syndrome. J Am Coll Surg. 2007; 204: 409-15. 10.1016/j.jamcollsurg.2006.12.005.
- Abou-Saif A, Al-Kawas FH. Complications of gallstone disease: Mirizzi syndrome, cholecystocholedochal fistula, and gallstone ileus. Am J Gastroenterol. 2002; 97: 249-54. 10.1111/j.1572- 0241.2002.05451.x.
- Erben Y, Benavente-Chenhalls LA, Donohue JM, Que FG, Kendrick ML, et al. Diagnosis and treatment of Mirizzi syndrome: 23-year Mayo Clinic experience. J Am Coll Surg. 2011; 213(1): 114-119.
- Yetışır F, Şarer AE, Acar HZ, et al. Laparoscopic treatment of Type III Mirizzi Syndrome by T-tube drainage. Case Rep Surg 2016; 1030358.
- Kulkarni SS, Hotta M, Sher L, Selby RR, Parekh D, et al. Complicated gallstone disease: Diagnosis and management of Mirizzi syndrome. Surg Endosc. 2017; 31(5): 2215-2222.
- Yetişir F, Şarer AE, Acar HZ, et al. Laparoscopic resection of cholecystocolic fistula and subtotal cholecystectomy by tri-staple in a Type V Mirizzi Syndrome. Case Reports Hepatol. 2016; 6434507.
- Cui Y, Liu Y, Li Z, Zhao E, Zhang H, Cui N. (2012) Appraisal of diagnosis and surgical approach for Mirizzi syndrome. ANZ J Surg. 82(10):708-713.
- Yuan H, Yuan T, Sun X, Zheng M. A minimally invasive strategy for Mirizzi syndrome type II. Surg Laparosc Endosc Percutaneous Tech. 2016; 26(3): 248-252.
- Chuang SH, Yeh MC, Chang CJ. Laparoscopic trans fistulous bile duct exploration for Mirizzi syndrome type II: a simplified standardized technique. Surg Endosc. 2016; 30(12): 5635-5646.
- Seah WM, Koh YX, Cheow PC, Chow PKH, Chan CY, et al. A retrospective review of the diagnostic and management challenges of Mirizzi syndrome at the Singapore General Hospital. Dig Surg. 2017; 35(6): 491-497.
- Binnie NR, Nixon SJ, Palmar KR. Mirizzi’s syndrome managed by endoscopic stenting and laparoscopic cholecystectomy. Br J Surg. 1992; 79: 647.
- Posta ZG. Unexpected Mirizzi’s anatomy: A major hazard to the common bile duct during laparoscopic cholecystectomy. Surg Endosc. 1995; 5: 412-414.
- Tung KL, Tang CN, Lai EC, et al. Robot-assisted laparoscopic approach of management for Mirizzi syndrome. Surg Laparosc Endosc Percutan Tech. 2013; 23: e17-21.
- Lee KF, Chong CN, Ma KW, et al. A minimally invasive strategy for Mirizzi syndrome: The combined endoscopic and robotic approach. Surg Endosc. 2014; 28: 2690-4.
- Magge D, Steve J, Novak S, et al. Performing the difficult cholecystectomy using combined endoscopic and robotic techniques: how I do it. J Gastrointest Surg. 2017; 21: 583-9.