
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Research Article - Open Access, Volume 5
Histoid leprosy mimicking secondary syphilis
Pankaj Das, MD1; Anuj Bhatnagar, MD1; Lalita Kumari, MBBS1; Thinley Wangmo, MBBS1; Lekshmi Priya Krishnan, MD1; Anand Mannu, MD1; Debdeep Mitra, MD2
1Department of Dermatology, Armed Forces Medical College, Pune, Maharashtra, India.
2Department of Dermatology, Command Hospital Air Force, Bangalore, Karnataka, India.
*Corresponding Author : Pankaj Das
Department of Dermatology, Armed Forces Medical
College, Pune, Maharashtra, India.
Tel: +919764993609,
Email: pankaj3609@gmail.com
Received : Dec 03, 2024
Accepted : Dec 20, 2024
Published : Dec 27, 2024
Archived : www.jcimcr.org
Copyright : © Das P (2024).
Citation: Das P, Bhatnagar A, Kumari L, Wangmo T, Krishnan LP, et al. Histoid leprosy mimicking secondary syphilis. J Clin Images Med Case Rep. 2024; 5(12): 3404.
Description
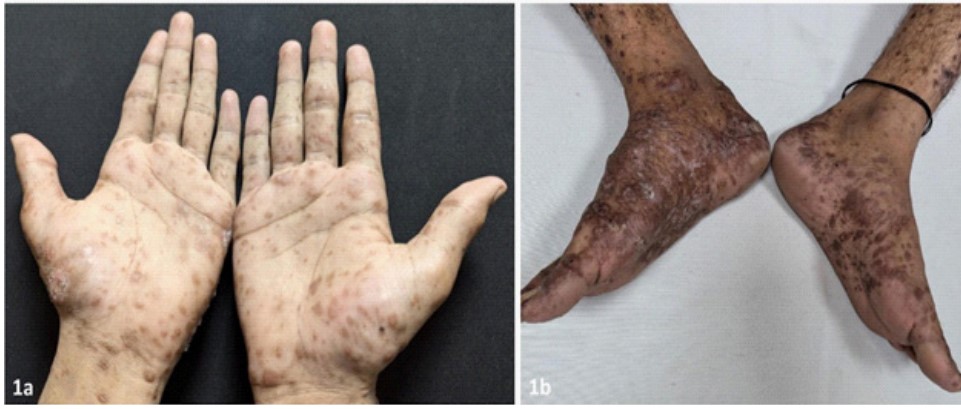
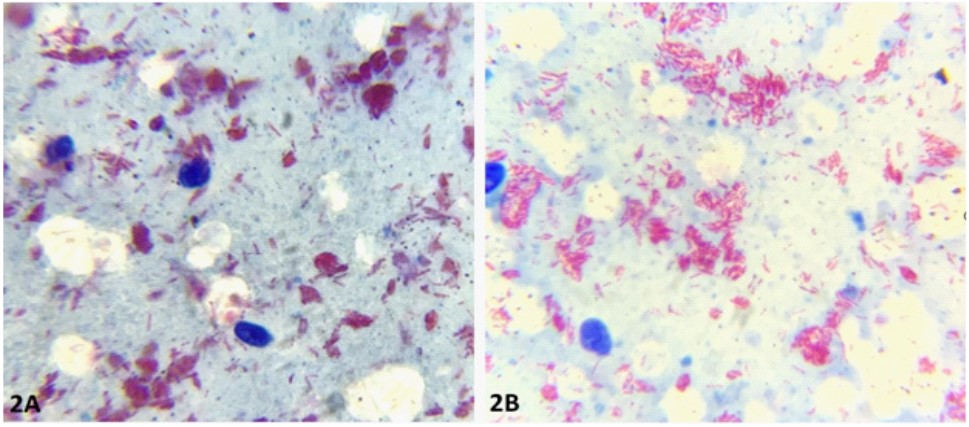
Leprosy is a chronic infectious granulomatous disease caused by Mycobacterium leprae. Histoid leprosy is an uncommon variant of multibacillary leprosy with characteristic clinical and histopathological findings. A 20-years-old sexually active unmarried male presented with multiple asymptomatic skin-colored lesions since past six months. He provided history of high-risk sexual behaviour since last two years with multiple partners with last sexual exposure a week ago. Clinical examination revealed skin-coloured papules distributed mostly over palms and soles followed by hands, feet and minimal lesions on trunk (Figure 1a,b). Buschke-Ollendorf sign was negative. There was patchy glove and stocking hypo-aesthesia over the hands and feet. Both the ulnar nerves were grade 2 thickened and non-tender. Ziehl-Neelsen (ZN) Stain on Slit Skin Smear (SSS) from one of the lesions showed acid fast bacilli in clumps arranged parallel to each other consistent with diagnosis of histoid variant of Hansen’s disease (Figure 2a). He was started on multi-drug therapy to which the lesions have started to regress and a repeat slit skin smear showed fragmented and granular acid- fast bacilli confirming the effectiveness of multi-drug therapy. (Figure 2b).
Histoid leprosy first described by Wade in 1960 and is considered as an uncommon variant of lepromatous leprosy with a estimated prevalence of 2.79% to 3.60%. It can occur de-novo before any treatment or after inadequate or irregular treatment especially after dapsone monotherapy [1]. It is seen mostly in males with a mean age of diagnosis from 21-40 years [2]. Classically it presents as discrete, non-tender, soft to firm papules, nodules and plaques with smooth and shiny surface with a normal appearing surrounding skin. The extensor aspects of the extremities, back and gluteal area are preferably affected. Other sites which may be involved are ears, face and rarely genitalia. Involvement of palms and soles are very rarely reported. Where-as the palms and soles are characteristically involved in papular syphilid in the secondary stage. Histoid leprosy mimicking nevus comedonicus, molluscum contagiosum and connective tissue disease have been reported [3]. Conversely, leishmaniasis, syphilis and Mycobacterium Avium Intracellulare infection have presented as histoid leprosy [4-6]. The peculiar histopathological finding of histoid leprosy is epidermal atrophy with a grenz zone just below epidermis. The inflammatory infiltrate consists of fusiform histiocytes arranged ina whorled, storiform pattern. Numerous intact rod shape bacilli are present in histiocytes and are arranged parallel to each other known as histoid habitus. The same histoid habitus is also appreciated in ZN stain in slit skin smear specimen as in our case.
Conflict of interest: Nil.
Patient consent: Both verbal and written consent has been taken from the patient.
References
- Kaushal I, Sharma A, Narang T, Chatterjee D, Vinay K. Histoid leprosy. QJM Mon J Assoc Physicians. 2024; 170.
- Malik N, Chaurasia P, Reddy A, Deokar SV. De novo histoid leprosy. BMJ Case Rep. 2024; 17(7): 260263.
- Abell E, Marks R, Jones EW. Secondary syphilis: a clinico-pathological review. Br J Dermatol. 1975; 93(1): 53-61.
- Histoid leprosy mimicking nevus comedonicus - PubMed [Internet]. 2024. https://pubmed.ncbi.nlm.nih.gov/39154361/.
- Molluscum contagiosum-like lesions in histoid leprosy in a 10-year-old Indian boy - PubMed [Internet]. 2024. https:// pubmed.ncbi.nlm.nih.gov/23679354/
- Histoid leprosy complicated by erythema nodosum leprosum mimicking connective tissue disease - PubMed [Internet]. 2024. https://pubmed.ncbi.nlm.nih.gov/37401254/.