
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Clinical Image - Open Access, Volume 5
Choledochal cyst during a elective laparoscopic cholecistectomy
Marcelo Pontillo-Walerovsky*; Iván Trostchansky-Vasconcellos; Roberto Valiñas Sotelo
Surgical Academic Unit F, Hospital de Clínicas “Dr. Manuel Quintela,” Montevideo, Uruguay.
*Corresponding Author : Pontillo-Walerovsky M
Surgical Academic Unit F, Hospital de Clínicas “Dr.
Manuel Quintela,” Montevideo, Uruguay.
Email: marspontillo@gmail.com
Received : Dec 02, 2024
Accepted : Dec 20, 2024
Published : Dec 27, 2024
Archived : www.jcimcr.org
Copyright : © Pontillo-Walerovsky M (2024).
Citation: Pontillo-Walerovsky M, Trostchansky-Vasconcellos I, Sotelosurgical RV. Choledochal cyst during a elective laparoscopic cholecistectomy. J Clin Images Med Case Rep. 2024; 5(12): 3405.
Description
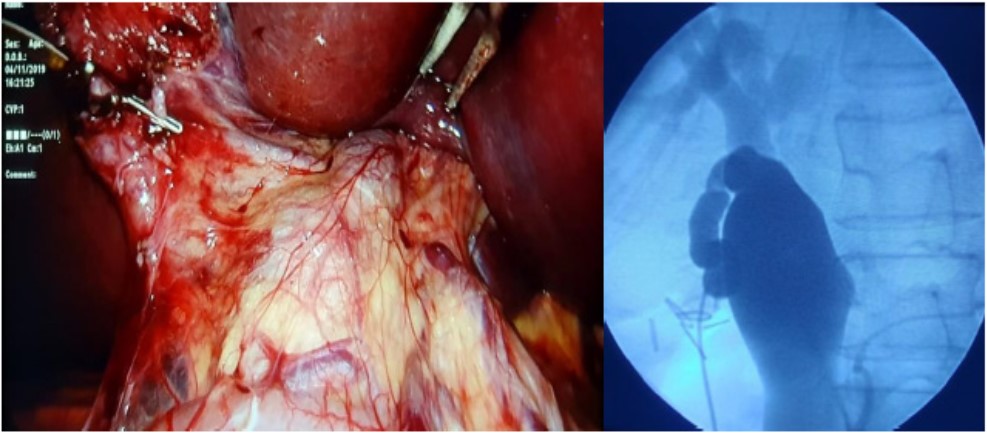
Female, 27 years old patient, healthy. During a laparoscopic cholecystectomy, a wide cystic duct (>1 cm) was found (Figure 1A). Cholangiography was performed and showed an extra hepatic bile duct dilation (>4 cm), without finding common bile duct stones inside (Figure 1B); the cholecystectomy was completed.
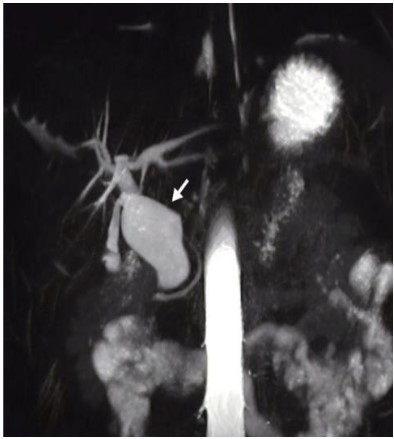
Magnetic resonance cholangiopancreatography was performed postoperatively, showing type IB choledochal cyst (Todani´s classification) [1], a sacular dilation that only involves the extrahepatic bile duct; few choledocholithiasis were also found (Figure 2).
Choledochal cyst is a rare disease (incidence of 1 in 100000 – 150000) [2] associated with primary choledocholithiasis, recurrent cholangitis, portal hypertension and increased risk of cholangiocarcinoma [3,4]. The patient underwent a resection of the extrahepatic bile duct and reconstruction with a “Roux-en-Y” hepaticojejunostomy [4,5]. Lifelong strict follow up is necessary, due to an increased risk of biliary cirrhosis development. We therefore emphasize the importance of performing intraop- erative cholangiography in the presence of anatomical alterations in biliary surgery.
References
- Miron A, Popa LG, Toma EA. The Curious Case of the Choledochal Cyst-Revisiting the Todani Classification: Case Report and Review of the Literature. Diagnostics. 2023; 13(6): 1059.
- Tariq WB, Twayana AR, Sunuwar N et al. Case Report: a rare case of choledochal cyst. F1000Res. 2022; 11: 919.
- Madadi-Sanjani O, Wirth TC, Kuebler JF et al. Choledochal Cyst and Malignancy: A Plea for Lifelong Follow-Up. Eur J Pediatr Surg. 2019; 29(2): 143-149.
- Lee KF, Lai EC, Lai PB. Adult choledochal cyst. Asian J Surg. 2005; 28(1): 29-33.
- Kowalski A, Kowalewski G, Kaliciński P, et al. Choledochal Cyst Excision in Infants-A Retrospective Study. Children. 2023; 10(2): 373.