
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 5
Bilateral choroidal folds in thyroid-associated ophthalmopathy without compressive optic neuropathy: A case report
Xintong Lin1,2,3; Wenjun Shu1,2,3; Haifeng Chen1,2,3; Lu Gan1,2,3; Rong Zhang1,2,3; Binbin Xu1,2,3; Xiaofeng Li1,2,3; Han Yue1,2,3; Jie Guo1,2,3; Jiang Qian1,2,3; Kang Xue1,2,3; Ruiqi Ma1,2,3*
1Key laboratory of Myopia and Related Eye Diseases, NHC, China.
2Key laboratory of Myopia and Related Eye Diseases, Chinese Academy of Medical Sciences, China.
3Department of Ophthalmology, Eye, Ear, Nose, and Throat Hospital of Fudan University, Shanghai, China.
*Corresponding Author : Ruiqi Ma
Department of Ophthalmology, Eye, Ear, Nose,
and Throat Hospital of Fudan University, Shanghai,
China.
Tel: 86-021-64377134;
Email: xuekang@foxmail.com
Received : Dec 02, 2024
Accepted : Dec 23, 2024
Published : Dec 30, 2024
Archived : www.jcimcr.org
Copyright : © Ma R (2024).
Abstract
A 54-year-old male developed bilateral vision loss and choroidal folds one year following COVID-19 vaccination. Initially diagnosed with thyroid-associated ophthalmopathy, he underwent an adequate course of steroid pulse therapy with no visual improvement. Further assessment revealed bilateral cataracts and lens dislocation. Computed tomography identified mild extraocular muscle thickening but no orbital apex crowding, ruling out compressive optic neuropathy. Lens surgery subsequently restored his vision and normalized his visual fields. However, two months postoperatively, he experienced recurrent blurred vision and restricted movement in the right eye. Magnetic resonance imaging confirmed extraocular muscle enlargement, leading to a diagnosis of compressive optic neuropathy, and tocilizumab therapy was initiated. Following treatment, the patient demonstrated improved vision, reduced muscle thickness, and enhanced motility. This case suggests that initial choroidal folds may be due to a combination of vaccine-related side effects and elevated orbital pressure, underscoring the potential for COVID-19 vaccination to cause atypical ocular symptoms.
Keywords: Choroidal folds; Thyroid-associated ophthalmopathy; Compressive optic neuropathy; COVID-19 vaccination; Tocilizumab.
Abbreviations: TAO: Thyroid-Associated Ophthalmopathy; DON: Dysthyroid Optic Neuropathy.
Citation: Lin X, Shu W, Chen H, Gan L, Ma R, et al. Bilateral choroidal folds in thyroid-associated ophthalmopathy without compressive optic neuropathy: A case report. J Clin Images Med Case Rep. 2024; 5(12): 3406.
Introduction
Thyroid-Associated Ophthalmopathy (TAO) is an immunemediated inflammatory disorder that affects the orbital tissues, commonly associated with Graves’ disease. The condition is characterized by symptoms such as eyelid retraction, exophthalmos, diplopia due to extraocular muscle involvement, and in severe cases, optic nerve compression leading to vision loss [1]. Treatment modalities for TAO include systemic corticosteroids, orbital radiotherapy and orbital decompression surgery [2,3]. Choroidal folds are a clinical sign observed as undulations in the retina and choroid, typically presented with blurred vision or metamorphopsia [4]. These folds can result from various conditions that cause sufficient compressive stress within the choroid, such as choroidal and orbital tumors and scleral buckling procedures [4]. Patients with TAO who exhibit choriordal folds often experience severe and chronic compression. However, this finding can also be observed during acute and severe exacerbations [5,6]. Treatment approaches for choroidal folds are primarily directed at the underlying cause, which may involve immunosuppressive therapy or surgical intervention [7]. The authors report a case of a 54-year-old male presenting with a one-year history of bilateral vision loss and choroidal folds, who was diagnosed with TAO previously. Subsequent examinations revealed bilateral cataracts and lens dislocation. Computed Tomography scan showed mild bilateral extraocular muscle thickening without orbital apex crowding. So, the patient was advised to undergo cataract surgery at first, and his vision was restored. Two months following the procedure, the patient again exhibited blurred vision, along with severe restriction of eye movements in all directions in the right eye. Further assessment confirmed the diagnosis of Dysthyroid Optic Neuropathy (DON), and the patient was subsequently treated with tocilizumab. The collection and assessment of protected patient health data were conducted in accordance with the Health Insurance Portability and Accountability Act of 1996 and aligned with the ethical guidelines set forth in the Declaration of Helsinki, as revised in 2013.
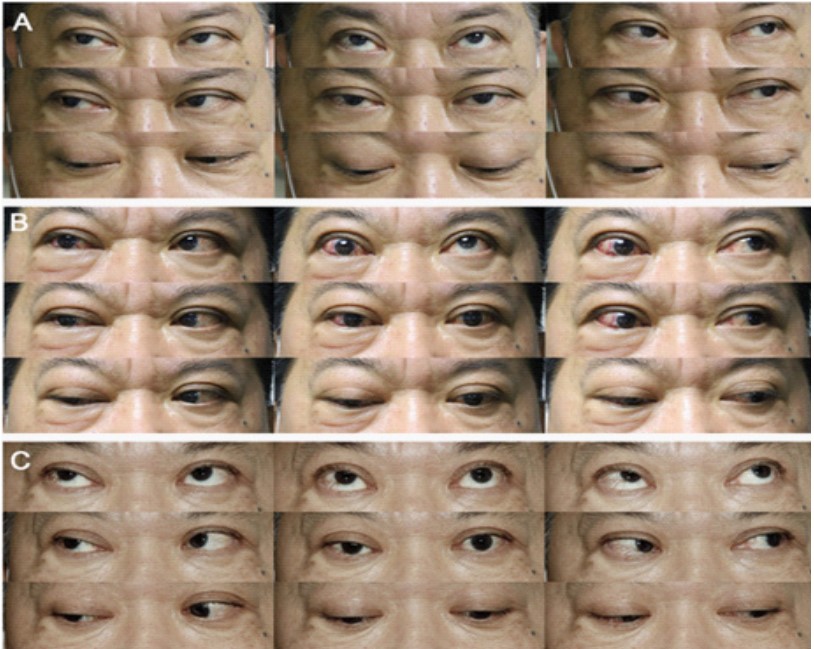
Case presentation
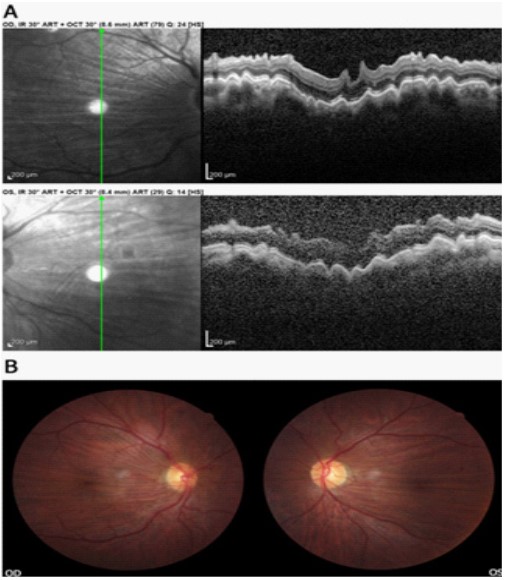
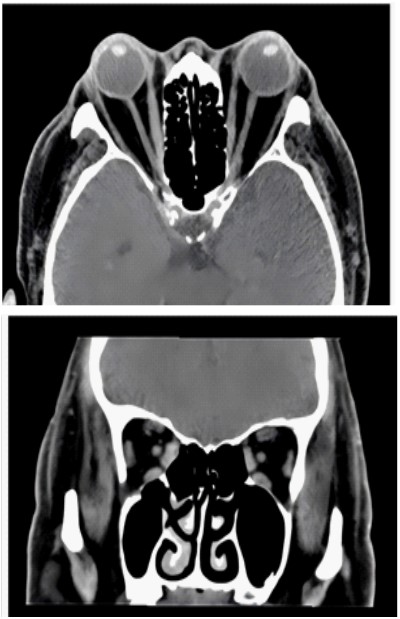
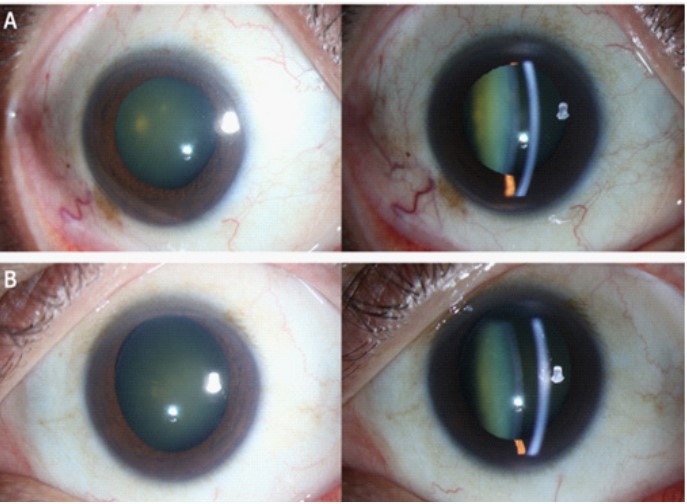
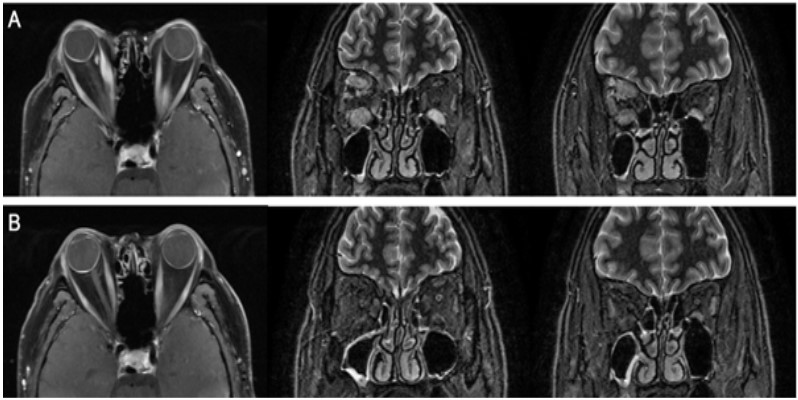
A 54-year-old man presented with a one-year history of bilaterally decreased vision. Ocular examination revealed uncorrected visual acuities of 20/40 (Snellen Chart) in the right eye and 20/1000 in the left eye, with best corrected visual acuity improving to 20/25 in the right eye and 20/200 in the left eye. Intraocular pressures were within normal limits, although the orbital pressure was slightly elevated. There was a limitation in adduction and abduction in both eyes. External examination showed mild redness of the upper eyelids, and the lower edge of the upper eyelid was found to be at the level of the pupillary margin in both eyes (Figure 1A). Slit lamp microscope examination revealed bilateral nuclear cataracts and the staging was C2N3P3 in the right eye and C2N3P4 in the left eye, according to the Lens Opacities Classification System III (LOCS III). Fundus examination indicated bilateral choroidal folds, with the optic nerves appearing normal (Figure 2A). The patient elaborated on his medical history, revealing that in May 2021, he initiated the COVID-19 vaccination series with the Sinovac vaccine, completing the standard three-dose regimen. In July 2021, he was diagnosed with Type 2 Diabetes Mellitus, which was effectively managed. Later, in October 2021, he presented with binocular diplopia and progressive vision loss, leading to a diagnosis of hyperthyroidism and TAO at an external hospital. Despite treatment with a steroid pulse therapy using methylprednisolone, totally a cumulative dose of 6.45 g, his symptoms of diplopia and vision loss continued. During this time, he tested positive for anti-AChR antibodies, resulting in a diagnosis of myasthenia gravis. Pyridostigmine was prescribed, which alleviated the diplopia but did not enhance his visual acuity. In December 2022, the patient presented to our hospital, reporting a one-year history of bilateral vision decline. So far, the patient has not been infected with COVID-19. Subsequently, we evaluated exophthalmos and conducted a computed tomography scan. The patient exhibited stable exophthalmos measurements at 23 mm bilaterally since the disease onset. The computed tomography scan demonstrated mild bilateral thickening of multiple extraocular muscles, without evidence of orbital apex crowding or optic nerve compression by muscles or other tissues (Figure 3). Choroidal folds were deemed unlikely to be caused by DON and were suspected to have other factors. Slit lamp microscope examination following mydriasis revealed a shallow anterior chamber in the right eye and an asymmetric depth of the anterior chamber in the left eye, indicative of lens dislocation (Figure 4). Consequently, the patient was diagnosed with bilateral lens dislocation and the vision loss was attributed to the dislocation and the presence of nuclear cataracts. It was recommended that the patient undergo bilateral cataract surgery initially to improve visual acuity and to facilitate the diagnostic evaluation for potential DON, given the progressive characteristics of TAO. The patient underwent cataract surgery in January and February 2023 and returned to our hospital for a follow-up visit. The examination showed that the patient’s best corrected visual acuity could reach 20/25 in the right eye and 20/22 in the left eye. Postoperative fundus photography report revealed that choroidal folds still existed in both eyes, similar to the pre-operative condition (Figure 2B). Despite the presence of choroidal folds, there was significant improvement in vision after the procedure. Notably, 2 months following the cataract operation, the patient presented with vision blurred and a significant limitation in all directions of eye movement in the right eye, accompanied by severe conjunctival hyperemia and edema (Figure 1B). And he also experienced exophthalmos measured at 26 mm in both eyes. Additionally, magnetic resonance imaging report indicated obvious thickening and enlargement of multiple extraocular muscles on the right side, suggesting optic nerve compression (Figure 5A). Since the patient had already received an adequate number of corticosteroids, further increasing the dosage might lead to systemic and local side effects. Therefore, it was recommended that the patient was treated with tocilizumab (Actemra) from July 2023 to February 2024, with a dose of 720 mg each time, for a total of six doses. Due to the favorable response to tocilizumab, the eye movement was improved and the exophthalmos was reduced (Figure 1C). After 6 months of follow-up, the patient’s visual acuity improved to 20/20 in both eyes, exophthalmos was reduced to 22 mm bilaterally, and ocular motility normalized. Magnetic resonance imaging showed that the degree of thickening and enlargement of the extraocular muscles in the right eye was reduced, and the STIR signal intensity was also decreased (Figure 5B). Ultimately, the patient did not undergo surgical intervention.
Discussion
In this case, a patient with a one-year history of vision loss and bilateral choroidal folds was previously diagnosed with TAO. Comprehensive examination revealed that the primary causes of vision loss were binocular lens dislocation and nuclear cataracts. The presence of choroidal folds was deemed idiopathic rather than due to DON. Consequently, cataract surgery was performed as an initial step to establish a basis for further therapeutic interventions. While some studies have implicated COVID-19 vaccination in causing ocular manifestations such as blurred vision, scleritis and choroidal folds [8,9]. Given these associations, we hypothesized that our patient might have developed posterior scleritis as an adverse effect of COVID-19 vaccination, which subsequently improved with steroid therapy. However, the choroidal folds observed did not show improvement following the steroid treatment, indicating a separate or ongoing pathological process. The pharmacological management of TAO includes corticosteroids, immunosuppressants, and monoclonal antibodies. Notably, in this case, a patient with DON unresponsive to corticosteroids showed a favorable response to tocilizumab treatment, which is consistent with another reported case [6]. Tocilizumab, a recombinant humanized monoclonal antibody targeting the interleukin-6 (IL-6) receptor, is FDA-approved for the treatment of patients with moderately to severely active TAO who do not respond to corticosteroids [10,11]. Adverse reactions can include infections, gastrointestinal issues, elevated liver enzymes, neutropenia, thrombocytopenia, hypercholesterolemia, and urticaria [12]. The standard treatment protocol is an 8 mg/kg dose administered intravenously every 4 weeks. However, the potential for relapse after discontinuation of the medication remains uncertain, necessitating further exploration and clinical experience to determine the optimal treatment duration and approach. This case presents a unique diagnostic and therapeutic approach, highlighting the importance of carefully exploring the reasons behind choroidal folds when they appear with TAO. To achieve effective management, it’s crucial to consider all therapeutic options available. By employing tocilizumab treatment, patients can potentially avoid orbital decompression surgery and still achieve favorable outcomes. We encourage more research on this targeted medical therapy as a potential alternative to surgical intervention. Additionally, larger study samples and longer durations of research are necessary to validate the effectiveness of these treatment methods.
Declarations
Ethics approval and consent to participate: The collection and assessment of protected patient health data were aligned with the ethical guidelines set forth in the Declaration of Helsinki and were approved by the Institutional Review Board at Eye, Ear, Nose, and Throat Hospital of Fudan University. Informed consent had been obtained from the patient.
Consent for publication: Informed consent had been obtained from the patient in the consent to publish.
Availability of data and materials: Not applicable.
Competing interests: The authors declare that they have no competing interests.
Funding: (1) National Natural Science Foundation of China (Grant No.82371101, No.82171099, No.82000940, No.81970835, No.81800867); (2) Natural Science Foundation of Shanghai (Grant No.20ZR1409500); (3) Shanghai Municipal Health Commission (Grant No.202340221); (4) Shanghai Hospital Development Center Foundation (Grant No.SHDC12024118).
Author information: Xintong Lin, Wenjun Shu and Haifeng Chen contributed equally as co-first authors. Kang Xue and Ruiqi Ma contributed equally as co-correspondence authors.
Authors’ contributions: Concept and design: Ruiqi Ma, Kang Xue; Acquisition, analysis, or interpretation of data: All authors; Drafting of the manuscript: Xintong Lin, Wenjun Shu, Haifeng Chen; Critical revision of the manuscript for important intellectual content: All authors; Obtained funding: Jiang Qian, Han Yue, Jie Guo, Ruiqi Ma; Administrative, technical, or material support: Jiang Qian, Binbin Xu, Xiaofeng Li, Rong Zhang; Supervision: Ruiqi Ma, Kang Xue; All authors read and approved the final manuscript.
References
- Rashad R, Pinto R, Li E, Sohrab M, Distefano AG. Thyroid Eye Disease. Life (Basel). 2022; 12(12).
- Hoang TD, Stocker DJ, Chou EL, Burch HB. 2022 Update on Clinical Management of Graves Disease and Thyroid Eye Disease. Endocrinol Metab Clin North Am. 2022; 51(2): 287-304.
- Burch HB, Perros P, Bednarczuk T, Cooper DS, Dolman PJ, et al. Management of Thyroid Eye Disease: A Consensus Statement by the American Thyroid Association and the European Thyroid Association. Thyroid. 2022; 32(12): 1439-70.
- Abazari A, Sibony PA. The Cause of Retinal and Choroidal Folds in Optic Disc Drusen. Ophthalmology. 2020; 127(11): 1583-5.
- Tran AQ, Zhang-Nunes SX, Cahill K, Alabiad CR, Shriver EM, et al. Thyroid eye disease with choroidal folds. Orbit. 2021; 40(3): 206-14.
- Almazrouei O, Alalawi F, Albrashdi S, Alsharqi H, Alsaadi A, et al. A 46-Year-Old Woman with a 4-Year History of Graves Disease, with Severe Corticosteroid-Unresponsive Thyroid Eye Disease, Successfully Treated with Tocilizumab. Am J Case Rep. 2023; 24: 938487.
- Jaworski A, Wolffsohn JS, Napper GA. Aetiology and management of choroidal folds. Clin Exp Optom. 1999; 82(5): 169-76.
- Negretti GS, Zeiger JS, Cherkas E, Shields CL. Posterior scleritis following COVID-19 vaccination or infection simulating uveal melanoma in 8 consecutive patients. Eye (Lond). 2024; 38(1): 185-91.
- Agarwal M, Patnaik G, Gupta A. Uveal effusion syndrome following COVID-19 vaccination. Am J Ophthalmol Case Rep. 2023; 32: 101884.
- Perez-Moreiras JV, Alvarez-Lopez A, Gomez EC. Treatment of active corticosteroid-resistant graves’ orbitopathy. Ophthalmic Plast Reconstr Surg. 2014; 30(2): 162-7.
- Toro-Tobon D, Rachmasari KN, Bradley EA, Wagner LH, Tooley AA, et al. Medical Therapy in Patients with Moderate to Severe, Steroid-Resistant, Thyroid Eye Disease. Thyroid. 2023; 33(10): 1237-44.
- Cabezas L, Jouve T, Malvezzi P, Janbon B, Giovannini D, et al. Tocilizumab and Active Antibody-Mediated Rejection in Kidney Transplantation: A Literature Review. Front Immunol. 2022; 13: 839380.