
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Research Article - Open Access, Volume 6
Can computed tomography of chest help in diagnosis of pulmonary arterial hypertension - Correlation between findings of computed tomography and echocardiography
Anurag Gupta*; Narinder Kaur; Jeet Ram Kashyap; Ravinder Kaur
Department of Radiodiagnosis, GMCH Sector 32, Chandigarh, India.
*Corresponding Author : Anurag Gupta
Resident, Department of Radiodiagnosis, GMCH Sector 32, Chandigarh, India.
Email: anuragg978@gmail.com
Received : Dec 12, 2024
Accepted : Jan 07, 2025
Published : Jan 14, 2025
Archived : www.jcimcr.org
Copyright : © Gupta A (2025).
Abstract
Introduction: Pulmonary Arterial Hypertension (PAH) is a condition characterized by increased pulmonary vascular resistance, which causes gradual rise in pulmonary artery pressure, compensatory right ventricular hypertrophy, and finally failure of right heart. It is a significant cause of morbidity in patients of ILD, COPD and other lung diseases, and imaging like echocardiography and CT scan can detect PAH at an earlier stage because at early stages signs of PAH may not be clinically evident and invasive cardiac catheterization is usually not available everywhere.
Objectives: Evaluate signs of pulmonary hypertension on computed tomography and to correlate them with signs of pulmonary hypertension on echocardiography.
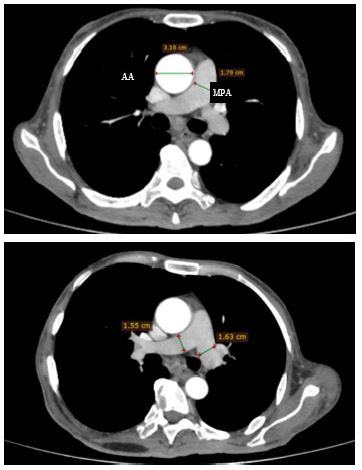
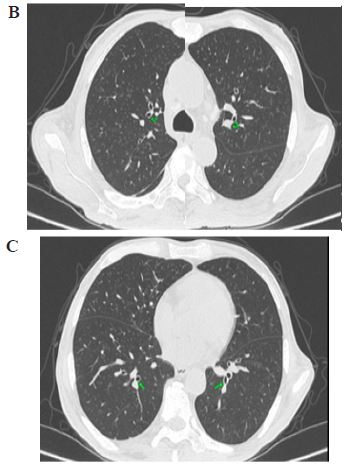
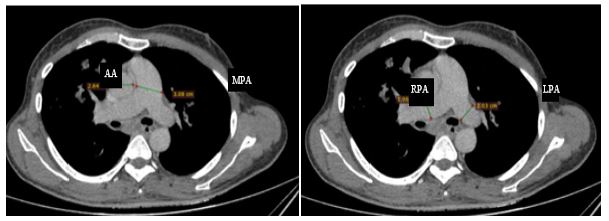
Methods: Fifty-five (55) patients clinically suspected of having pulmonary arterial hypertension of different age and sexes underwent chest computed tomography and echocardiography from November 2022 to March 2024. Cardiac chamber size, Pulmonary Artery Systolic Pressure (PASP) and Tricuspid Annular Plane Systolic Excursion (TAPSE) among other were measured on Echocardiography. Main pulmonary artery diameter, Aortic diameter, Ratio of main pulmonary artery and ascending aortic diameters, Right and left main pulmonary artery diameter and segmental artery-to-bronchus diameter ratio at the level of origin of right apical, left apicoposterior, bilateral posterobasal segmental arteries and adjacent bronchi were measured on Computed tomography. These were then correlated.
Results: The data showed that significant positive correlation was seen in our study between main, right and left pulmonary artery diameter, main pulmonary artery diameter-to-ascending aorta diameter ratio and four segmental pulmonary artery-to-segmental bronchus ratios with PASP, right atrium & ventricle dimension. This suggests that the degree of dilation of pulmonary arterial system is proportional to the increasing severity of pulmonary artery hypertension. In our study negative correlation was seen between most of the chest computed tomography parameters with TAPSE which decreases with increasing severity of pulmonary artery hypertension.
Keywords: Pulmonary artery hypertension; Computed tomography; Echocardiography; Chest; Invasive cardiac catheterization; Pulmonary artery systolic pressure; Tricuspid annular plane systolic excursion; Main pulmonary artery diameter-to-ascending aortic diameter ratio; Segmental pulmonary artery-to-segmental bronchus ratio.
Citation: Gupta A, Kaur N, Kashyap JR, Kaur R. Can computed tomography of chest help in diagnosis of pulmonary arterial hypertension - Correlation between findings of computed tomography and echocardiography. J Clin Images Med Case Rep. 2025; 6(1): 3422.
Background
Pulmonary arterial hypertension is an abnormal pressure elevation in pulmonary vessels, with mean pulmonary artery pressure >25 mmHg, which is as a result of severe vascular proliferation and remodelling. It is associated with significant morbidity and mortality. Clinically, these pulmonary vessel changes first show up as vague signs and symptoms including chest pain, fatigue, syncope, and unexplained exercise-induced dyspnoea. These are frequent symptoms indicating malfunction in the right ventricle. The possibility of PAH is given on computed tomography if mean pulmonary artery diameter exceeds or equal to 29 mm [1,2]. Despite growing awareness of PAH, most cases still have delayed detection [2]. Due to its non-specific clinical features along with costly and scarcely available investigations, PAH diagnosis remains difficult. In the recent corona virus disease pandemic of 2019, higher chances are that severe COVID in the patients could impair the lungs and its arteries permanently, encouraging development of PAH. However, diagnosis of PAH in patient treatment is necessary at an early stage for an overall better outcome [3]. The outlook for PAH is dismal; if it is not identified and treated promptly, it could progress to right heart failure, which leads to higher deaths [3].
Multiple imaging modalities are available for evaluation of PAH.
• Chest X-ray
• Echocardiography (ECHO)
• Invasive cardiac catheter angiography
• Computed Tomography (CT)
• MRI
All these techniques have their own limitations and benefits.
Chest X-ray is a widely available and cost-effective investigation and has high accuracy for detection of PAH. The sings of PAH on chest X-ray include enlarged pulmonary artery, right ventricle, right atrium with peripheral pruning of pulmonary vessels, however, it has low sensitivity, specificity and normal chest X-ray does not rule out PAH in early and asymptomatic cases. Therefore, there is a need for widely available, more sensitive investigation [1].
Echocardiography: Though, echocardiography is not the gold standard for diagnosing PAH, it is a key screening test and usually the first step in the diagnostic algorithm because it has the advantage of evaluating PAH in a non-invasive manner, is safe, easily available and repeated and can be done as a portable investigation as well. Despite the fact that pulmonary arterial hypertension is a vascular condition, the structural and functional assessment of the right ventricle is very important for pulmonary arterial hypertension diagnosis and follow-up. Several complementing criteria of right ventricular size and function should be included in overall evaluation of the right ventricle in pulmonary arterial hypertension [4]. Echocardiography enables assessment of other indicators of persistent right heart pressure overload, such as right ventricular hypertrophy or enlargement, enlarged right atrium and pulmonary arteries, abnormal interventricular septum with D-shaped left ventricle, systolic/diastolic flattening of the interventricular septum with right heart systolic dysfunction. However, in pulmonary hypertensive patients, these other signs of right heart overload might frequently manifest later and have a dismal prognosis [5]. One of the most important predictors of prognosis in individuals with Pulmonary arterial hypertension is function of right ventricle. However, in mild and asymptomatic cases of PAH this test is quite insensitive [5]. Pulmonary artery systolic pressure is measured by tricuspid regurgitation jet velocity and right atrial pressure (using collapsibility index of Inferior Vena Cava). Pulmonary artery diastolic pressure can be indicated by pulmonary regurgitation. Echocardiography also helps in ruling out left heart disease as a cause of PAH. Echocardiography can measure increased Pulmonary Artery Systolic Pressure (PASP), show dilatation of right heart, ventricular septal bowing to left, measuring of Tricuspid Annular Plane Systolic Excursion (TAPSE), right outflow tract dilation, right ventricle hypertrophy, increased right atrial pressure, abnormal blood flow velocity and pattern of right heart outflow and atrial septal bowing, all these are considered indirect signs of Pulmonary arterial hypertension [6]. Invasive cardiac catheter angiography- This is the gold standard technique for direct and accurate measurement of pulmonary artery pressure. It involves gaining access to the vascular system through a peripheral vessel and reaching towards right heart and pulmonary artery to measure Pulmonary Artery Pressure (PAP) [7], pulmonary capillary wedge pressure (PCWP-indirect measurement of left atrial pressure), Cardiac Output (CO) and Pulmonary Vascular Resistance (PVR). These measurements are crucial for confirming the diagnosis of PAH, distinguishing it from other types of pulmonary hypertension, and assessing disease severity. By directly measuring Pulmonary Vascular Resistance (PVR) and other hemodynamic parameters [8], cardiac catheterization allows clinicians to assess the severity of PAH. This information is essential for risk stratification, treatment planning, and prognostication. Serial cardiac catheterization enables clinicians to monitor the response to PAH-specific therapies over time. Changes in hemodynamic parameters, such as mPAP, PVR, and CO, can indicate the effectiveness of treatment and guide adjustments to therapy to optimize patient outcomes [8]. It is a complex procedure requiring technical expertise and well-equipped catheterization labs [10]. Close collaboration among multidisciplinary teams, including interventional cardiologists, pulmonologists, and specialized PAH centers, is essential to ensure optimal patient care and outcomes. Computed tomography is a routinely used imaging tool in work-up for pulmonary arterial hypertension patients due to its high resolution and multi-planar reconstruction capabilities, but with risk of ionizing radiation and complications of iodine containing contrast media in some cases. It detects dilatation of pulmonary artery and a maximum diameter (MPA) of more than 29 mm, just above its bifurcation, has a 97% Positive Predictive Value (PPV). However, a maximum pulmonary artery diameter <29 mm does not rule out PAH completely [14]. Ratio of MPA to aortic diameter (at the same level) >1.0 indicates towards PAH particularly in young patients of PAH without aortic ectasia. It can also measure heart chamber size which, if dilated is an indirect sign of pulmonary artery hypertension. In patients with severe interstitial lung disease particularly, segmental artery diameter/ segmental bronchus diameter ratio of more than 1:1 in three or four lobes along with dilated pulmonary artery has around 100% accuracy in the diagnosis of PAH. Enlarged main right and left pulmonary artery more than 18 mm may also predict prognosis [11]. Mural calcifications, tortuosity of vessels and pruning of peripheral arterial branches may also indicate long standing cases of PAH [12]. Magnetic Resonance Imaging (MRI) and Echocardiography are cornerstones of non-invasive cardiac imaging, each offering unique advantages in the assessment of cardiac structure and function. While echocardiography provides real-time, bedside imaging with excellent temporal resolution, MRI offers superior tissue characterization and spatial resolution [13]. MRI enables visualization of the pulmonary vasculature, including the main pulmonary artery, pulmonary arteries, and pulmonary veins, using contrast-enhanced Magnetic Resonance Angiography (MRA). Phase-contrast MRI allows for non-invasive measurement of blood flow velocities and quantification of pulmonary artery flow dynamics, facilitating the assessment of Pulmonary Vascular Resistance (PVR) and right ventricular afterload. MRI’s ability to provide high-resolution images with excellent tissue contrast makes it indispensable for tissue characterization in various cardiac pathologies. It enables the differentiation between normal and abnormal myocardial tissue, allowing for the detection and characterization of myocardial infarction, myocarditis, infiltrative cardiomyopathies (such as amyloidosis and sarcoidosis), and ischemic and non-ischemic cardiomyopathies, which are important determinants of right ventricular function and prognosis in PAH. MRI’s accuracy and reproducibility in quantifying cardiac chamber volumes, myocardial mass [14], and blood flow velocities make it an invaluable tool for assessing cardiac structure and function. By providing precise measurements of left ventricular volumes, ejection fraction, myocardial strain, and tissue perfusion, MRI complements echocardiography findings and enhances diagnostic accuracy. MRI also offers comprehensive evaluation of cardiac function, providing insights into ventricular volumes, ejection fraction, myocardial strain, and tissue perfusion [15]. Its ability to visualize cardiac motion in multiple planes allows for accurate assessment of regional wall motion abnormalities and myocardial contractility. Moreover, MRI facilitates the assessment of valvular function, quantifying regurgitant volumes and assessing the severity of valvular lesions, such as aortic stenosis and mitral regurgitation. The integration of MRI findings with echocardiography enhances diagnostic capabilities and improves patient management in pulmonary hypertension [16]. While echocardiography remains the primary imaging modality for initial assessment and serial monitoring in pulmonary artery hypertension due to its accessibility and real-time imaging capabilities, MRI serves as a valuable adjunct for cases requiring further characterization or when echocardiography is inconclusive.
Methodology
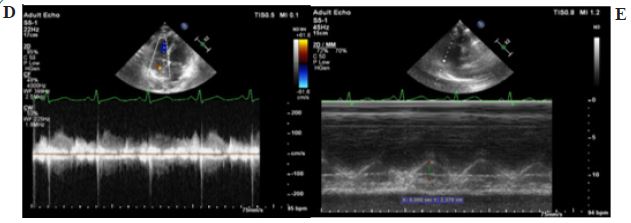
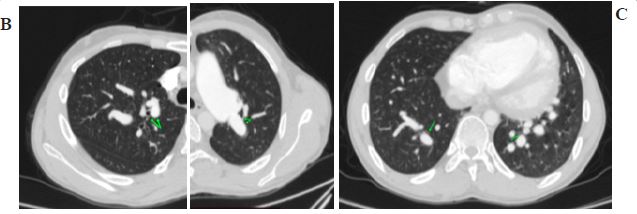
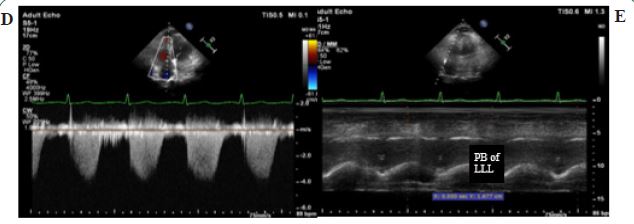
Patients: This prospective observational study was approved by the Institutional Ethics Committee (837R/2022/237, November 2022). A standard protocol was being followed for all patients who meet the inclusion criteria with no conditions of exclusion criteria. Patients coming to pulmonary, cardiac or medicine OPDs with relevant clinical history and high suspicion underwent echocardiography and CT. These patients were enrolled as study subjects only after taking their written informed consent. Relevant clinical history, previous investigation details were taken from the patient. Exclusion criteria was congenital heart disease patients, patients with history of allergy to iodine containing contrast media, patients having deranged renal function where contrast study is required. For Echocardiography patients were scanned with PHILLIPS EPIQ 7C (Model GMDW 40761, Massachusetts-USA) machine with S5-1(1-5 MHz) probe. The imaging was done by 2-Dimensional, M-mode and color doppler echocardiography. The dimensions of various chambers of heart were recorded by using M-mode echocardiography in end diastolic and end systolic phases of cardiac cycle. Tricuspid valve was assessed by 2-D and color doppler modes of echocardiography. Tricuspid Annular Plane Systolic Excursion (TAPSE) was measured using M-mode echocardiography. Patients then underwent HRCT, NCCT, CECT of chest and CTPA. The patients undergoing contrast CT/angiography were included only if they had normal RFTs (Urea and Serum creatinine). Patients were scanned using 64 slice Multidetector Computed Tomography (MDCT) machine (Phillips INGENUITY CT machine equipment number 60326268, Ohio-USA). NCCT/HRCT/ CECT/CTPA volumetric scan were acquired with scanning and reconstruction parameters as Tube Voltage – 120 KVp; Effective Tube Current-Time/slice – 250 mAs/slice; Collimation–64 X 0.625 mm; Rotation Speed – 0.75s; Pitch 1.014, Section Thickness-1 mm and Reconstruction Interval–3 mm. In axial CT scans following measurements taken were, Main pulmonary artery and ascending aorta diameter at the level showing bifurcation of main pulmonary artery in mediastinal window from which ratio of main pulmonary artery and ascending aortic diameters was calculated, right and left main pulmonary artery diameters and segmental artery-to-bronchus diameter ratios at the level of origin of right apical, left apicoposterior, bilateral posterobasal segmental arteries and adjacent bronchi in axial scans on lung window as segmental bronchi are better appreciated on lung window. Findings of pulmonary arterial hypertension on CT were observed and the same were compared with that of echocardiography.
Statistical analysis: The data was collected, tabulated, and analysed. The data normality was checked by using Shapiro-Wilk test. Pearson correlation coefficient was used for correlation of echocardiography parameters with Computed tomographic parameters. The association of the variables which were quantitative in nature was analyzed using ANOVA. The data entry was done in the Microsoft EXCEL spreadsheet and the final analysis was done with the use of Statistical Package for Social Sciences (SPSS) software, IBM manufacturer, Chicago, USA, ver. 25.0. For statistical significance, p value of less than 0.05 was considered statistically significant.
Results
By doing this study, we tried to correlate findings of PAH on chest CT with echocardiography and look for features of PAH on chest CT so that we can study the current role of chest CT in screening and follow up of PAH patients in the north Indian population of the country. We enrolled 55 patients who aged more than 18 years and less than 85 years. Maximum number of patients belonged to the age group 51 to 60 years constituting about 25.45% of the total study population. The mean age of patients having PAH was 54.3±16.5 years. 36 (65.45 %) of the total participants with PAH were females, while 19 patients (34.54%) of the participants were males. Our study reported mean (±SD) for diameter of the main pulmonary artery (MPA) as 34.3 (±7.53) mm and the MPA to Ascending Aorta (AA) ratio averaged 1.26 (±0.35). The right pulmonary artery diameter averaged 24.05 (±4.59) mm, while the left pulmonary artery diameter was slightly smaller at 23.16 (±4.31) mm. Additionally, means (±SD) for segmental artery to bronchus ratios for apical segment of RUL was 1.81 (±0.34), for posterobasal segment of RLL was 1.72 (±0.4), for apicoposterior segment of LUL was 1.83 (±0.5), and for posterobasal segment of LLL was 1.72 (±0.42). The subjects were also subjected to Echocardiography and various parameters relevant in the context of PAH were taken such as pulmonary artery systolic pressure (PASP), Tricuspid Annular Plane Systolic Excursion (TAPSE), right atrial and ventricular dimensions, tricuspid regurgitation, maximum, minimum diameters and collapsibility of inferior vena cava.
The mean (±SD) values for Pulmonary Artery Systolic Pressure (PASP) were 54.3 (±24.99) mm, for tricuspid annular plane systolic excursion (TAPSE) was 16.42 (±3.38) mm, right atrium dimension was 50.2 (±8.12) mm, right ventricle dimension was 51.02 (±10.48) mm, maximum inferior vena cava (IVC) diameter was 23.64 (±3.53) mm, minimum IVC diameter was 14.12 (±3.53) mm, and IVC collapsibility index was 40.73 (±8.62%). Moderately positive correlation was seen between main pulmonary artery with PASP, right atrium dimension with correlation coefficient of 0.463, 0.4 respectively. Weak negative correlation was seen between main pulmonary artery with TAPSE with correlation coefficient of -0.181. Weak positive correlation was seen between MPA: AA ratio with PASP, right atrium dimension, right ventricle dimension with correlation coefficient of 0.358, 0.286, 0.264 respectively. Weak negative correlation was seen between MPA: AA ratio with TAPSE and IVC Collapsibility Index with correlation coefficient of -0.158 and -0.215 respectively. Weak positive correlation was seen between right pulmonary artery diameter with PASP, right atrium dimension and right ventricle dimension with correlation coefficient of 0.377, 0.341, and 0.323 respectively. Weak negative correlation was seen between right pulmonary artery diameter with TAPSE with correlation coefficient of -0.164. Weak positive correlation was seen between left pulmonary artery diameter with PASP, right atrium dimension and right ventricle dimension with correlation coefficient of 0.348, 0.307 and 0.347 respectively. Weak negative correlation was seen between left pulmonary artery diameter with TAPSE with correlation coefficient of -0.206.
Apical segment of RUL: Moderately positive correlation was seen between segmental artery to bronchus ratio Apical segment of RUL with PASP, right atrium dimension with correlation coefficient of 0.439, 0.404 respectively. Weak negative correlation was seen between segmental artery to bronchus ratio Apical of RUL with TAPSE with correlation coefficient of -0.25.
Posterobasal segment of RLL: Weak positive correlation was seen between segmental artery to bronchus ratio posterobasal segment of RLL with PASP, right atrium dimension, right ventricle dimension, with correlation coefficient of 0.353, 0.332 and 0.311respectively. No correlation was seen between segmental artery to bronchus ratio Posterobasal of RLL with TAPSE with correlation coefficient of 0.035.
Apicoposterior segment of LUL: Moderately positive correlation was seen between segmental artery to bronchus ratio Apicoposterior of LUL with PASP with correlation coefficient of 0.429. Weak positive correlation was seen between segmental artery to bronchus ratio Apicoposterior of LUL with right atrium dimension, right ventricle dimension with correlation coefficient of 0.339 and 0.322 respectively. No correlation was seen between segmental artery to bronchus ratio Apicoposterior of LUL with TAPSE with correlation coefficient of 0.012.
Posterobasal segment of LLL: Weak positive correlation was seen between segmental artery to bronchus ratio Posterobasal of LLL with PASP, right atrium dimension with correlation coefficient of 0.185 and 0.11 respectively. Weak negative correlation was seen between segmental artery to bronchus ratio Posterobasal of LLL with TAPSE with correlation coefficient of -0.126.
Discussion/conclusion
Pulmonary Artery Hypertension (PAH) is a pathological condition characterized by elevated pressure in the pulmonary arteries, leading to progressive right ventricular dysfunction and, ultimately, heart failure. It is diagnosed when the mean pulmonary artery pressure exceeds 25 mmHg at rest, as measured by right heart catheterization, the gold standard diagnostic method. Since right heart cauterization is an invasive test, there is urgent need for a sensitive noninvasive investigation that can be used to prioritize patients which are to be referred for right sided heart catheterization [3].
Other investigations for Pulmonary artery hypertension include computed tomography, echocardiography, magnetic resonance imaging etc. Findings on computed tomography and echocardiography individually can at best, act as a screening test for PAH with high number of false positives. The combination of findings on computed tomography and echocardiography can provide stronger evidence for PAH, prompting further confirmatory testing, and aiding in the differentiation of PAH from other causes of dyspnea and right heart failure [17]. The pathophysiology behind the findings of dilation of the pulmonary arterial tree on chest computed tomography in pulmonary artery hypertension is a combination of increased vascular resistance, increased pressure and vascular remodeling [4].
Age: The mean age of patients having PAH was 54.3±16.5 years. This is seen in concordance with a study conducted by Humbert et al. in 2006 who showed median age of diagnosis of PAH to be around 50 years indicating that PAH affects middle-aged adults predominantly [18,19].
Gender: In our study, PAH is twice as more common in females than males with a female-to-male ratio of 1.9:1. Which is consistent with observations as per studies done by Humbert et al. in 2006 and McGoon et al. in 2013 which show that PAH affects females more than males, with a female-to-male ratio of about 2:1 [19]. Mean MPA in our study was 34.3 mm which is greater than 29.63 in the study done by Fakharian et al. in 2011 [20]. Mean for PASP in our study was 56.42 mmHg which was significantly higher than 37.1 mmHg found by Devaraj et al. in 2010 [17]. Mean PASP was 45.60 mmHg in the study done by Fakharian et al. in 2011 [20]. Our findings are in concordance with study done by Devaraj et al. in 2010 wherein the ratio of diameter of the main pulmonary artery-to-ascending aorta diameter correlated strongly with mPAP [17]. Findings of study done by Rehman et al in 2022 were also concordant with our finding [21]. However, our findings are discordant with findings of a study done by Fakharian et al in 2011 wherein no significant linear correlation was found between main pulmonary artery diameter calculated on CT scans and pulmonary artery pressure calculated by echocardiography (P value=0.17, r=0.15) in patients of interstitial lung disease [20]. The negative correlation of main pulmonary artery with TAPSE is consistent with the fact that the value of TAPSE generally reduces in pulmonary artery hypertension [22,23]. The IVC collapsibility index is inversely related to pulmonary artery hypertension and associated RV dysfunction, which is consistent with the finding of negative correlation between MPA and IVC collapsibility index in our study [24]. Chen et al. in 2015 showed that right and left pulmonary artery diameter correlated with PASP, which is consistent with our findings [25]. Our findings are also consistent with findings of study done by Ratanawatkul et al. in 2020 which showed correlation between right and left pulmonary artery with mPAP [26].
The negative correlation of Right and left pulmonary artery diameters with TAPSE is consistent with the fact that the value of TAPSE generally reduces in pulmonary artery hypertension [22,23]. We found a correlation between the segmental pulmonary artery and adjacent bronchus of all four segments as mentioned above with pulmonary artery systolic pressure. Our findings are in concordance with a study done in 2010 by Devaraj et al. wherein the same ratio of the four segmental pulmonary arteries and adjacent bronchus correlated strongly with mPAP [17].
Tan RT et al. also found similar correlation in a study done in 1998 [27]. Refini et al. in 2020, in partial concordance with our findings, found a strong correlation between the ratio of the segmental artery-to-adjacent bronchus diameters of the apicoposterior segment of the left upper lobe, but not between mPAP and other three segmental artery-to-adjacent bronchus diameter ratios [28]. The negative correlation of Apical segment of RUL and Posterobasal segment of LLL with TAPSE is consistent with the fact that the value of TAPSE generally reduces in pulmonary artery hypertension [22,23]. Refini et al. in 2020 tried to combine the parameters of computed tomography and echocardiography and synthesize a composite index which, according to their study, was found to be more precise than the same parameters considered separately in predicting and for follow up of patients with pulmonary arterial hypertension. Same index was also used by Devaraj et al. in 2010. Similar composite index should be synthesized in Indian population to reduce the need for invasive procedures like cardiac catheterization to diagnose pulmonary hypertension [17-23]. The study was conducted using proper methodology but like in any other study, our study has a few noteworthy limitations. First, this study had a small sample size. Large-scale multicentric studies with larger population sizes are needed to validate and standardize the findings of our study before their use in clinical practice. Second, we did not include the gold standard invasive cardiac catheterization in our study due to non-availability at our institution which might have resulted in a greater number of false positives. Third, we did not take controls i.e. patients without PAH in our study and therefore were unable to calculate the sensitivity and specificity of chest computed tomography in diagnosing PAH. Fourth, as the results were recorded by the same two radiologists, inter-observer agreement was not possible. Based on our study, the conclusions drawn were that Pulmonary artery hypertension is seen more commonly in the late middle to old age group (50-70 years), is twice more common in females as compared to males and findings of pulmonary arterial hypertension on chest computed tomography correlate well with the findings on echocardiography.
References
- Bossone E, Ferrara F, Grünig E. Echocardiography in pulmonary arterial hypertension. Curr Opin Cardiol. 2015; 30: 574-86.
- Goerne H, Batra K, Rajiah P. Imaging of pulmonary arterial hypertension: an update. Cardiovasc Diagn Ther. 2018; 8: 279-96.
- Dunlap B, Weyer G. Pulmonary arterial hypertension: Diagnosis and Treatment. Am Fam Physician. 2016; 94: 463-9.
- Shen Y, Wan C, Tian P, Wu Y, Li X, et al. CT-base pulmonary artery measurement in the detection of pulmonary arterial hypertension: a meta-analysis and systematic review. Medicine (Baltimore). 2014; 93: 256.
- Bossone E, D’Andrea A, D’Alto M, Citro R, Argiento P, et al. Echocardiography in pulmonary arterial hypertension: from diagnosis to prognosis. J Am Soc Echocardiogr. 2013; 26: 1-14.
- Haddad F, Hunt SA, Rosenthal DN, Murphy DJ. Right ventricular function in cardiovascular disease, part I: Anatomy, physiology, aging, and functional assessment of the right ventricle. Circulation. 2008; 117: 1436-48.
- Qaiser KN, Lane JE, Tonelli AR. Right heart catheterization for pulmonary arterial hypertension during the coronavirus disease 2019 pandemic. Pulm Circ. 2020; 10: 2045894020948783.
- Ullah W, Minalyan A, Saleem S, Nadeem N, Abdullah HM, et al. Comparative accuracy of non-invasive imaging versus right heart catheterization for the diagnosis of pulmonary arterial hypertension: A systematic review and meta-analysis. Int J Cardiol Heart Vasc. 2020; 29: 100568.
- Humbert M, Weatherald J. Right heart catheterisation is still a fundamental part of the follow-up assessment of pulmonary arterial hypertension. Eur Respir J. 2018; 52: 1800738.
- Galie N, Humbert M, Vachiery JL, Gibbs S, Lang I, et al. Right heart catheterization in pulmonary hypertension. European Respiratory Journal. 2020; 48(1): 56-69.
- Pérez-Enguix D, Morales P, Tomás JM, Vera F, Lloret RM. Computed tomographic screening of pulmonary arterial hypertension in candidates for lung transplantation. Transplant Proc. 2007; 39: 2405-8.
- Zisman DA, Karlamangla AS, Ross DJ, Keane MP, Belperio JA, et al. High- resolution chest CT findings do not predict the presence of pulmonary arterial hypertension in advanced idiopathic pulmonary fibrosis. Chest. 2007; 132: 773-9.
- Hundley WG, Bluemke DA, Finn JP, Flamm SD, Fogel MA, et al. ACCF/ACR/AHA/NASCI/SCMR 2010 expert consensus document on cardiovascular magnetic resonance: a report of the American College of Cardiology Foundation Task Force on Expert Consensus Documents. Journal of the American College of Cardiology. 2010; 55(23): 2614-2662.
- Pennell DJ, Sechtem UP, Higgins CB, Manning WJ, Pohost GM. Clinical indications for cardiovascular magnetic resonance (CMR): Consensus Panel report. European Heart Journal. 2004; 25(21): 1940-1965.
- Plein S, Schulz-Menger J, Almeida A, Mahrholdt H, Rademakers F, et al. European Society of Cardiology Working Group on Cardiovascular Magnetic Resonance: Recommendations for cardiovascular magnetic resonance imaging. European Heart Journal. 2007; 29(6): 587-593.
- Devaraj A, Wells AU, Meister MG, Corte TJ, Wort SJ, et al. Detection of pulmonary arterial hypertension with multidetector CT and echocardiography alone and in combination. Radiology. 2010; 254: 609-16.
- McGoon MD, Benza RL, Escribano-Subias P, et al. Pulmonary arterial hypertension: epidemiology and registries. J Am Coll Cardiol. 2013; 62(25): 51-59.
- Humbert M, Sitbon O, Chaouat A, et al. Pulmonary arterial hypertension in France: results from a national registry. Am J Respir Crit Care Med. 2006; 173(9): 1023-1030.
- Fakharian A, Hamidi N, Hosseinloo BH, Rezaei S, Afshar EE, et al. Correlation between the Pulmonary Artery Pressure Measured in Echocardiography and Pulmonary Artery Diameter in the CT-Scan of Patients Suffering from Interstitial Lung Disease. Tanaffos. 2011; 10: 37-41.
- Freed BH, Gomberg-Maitland M, Chandra S, Mor-Avi V, Rich S, et al. Late gadolinium enhancement cardiovascular magnetic resonance predicts clinical worsening in patients with pulmonary hypertension. JACC: Cardiovascular Imaging. 2012; 5(4): 348-358.
- Alunni JP, Degano B, Arnaud C, et al. Cardiac magnetic resonance imaging in pulmonary arterial hypertension: correlations of right ventricular function with clinical and hemodynamic parameters. Arch Cardiovasc Dis. 2012; 105(3): 167-175.
- Van Wolferen SA, Marcus JT, Boonstra A, et al. Prognostic value of right ventricular mass, volume, and function in idiopathic pulmonary arterial hypertension. Eur Heart J. 2007; 28(10): 1250-1257.
- Huang S, Wan J, Wang H, et al. Relationship between inferior vena cava collapsibility index and pulmonary artery pressure in patients with pulmonary hypertension. J Thorac Dis. 2015; 7(3): 416-422.
- Chen X, Liu K, Wang Z, Zhu Y, Zhao Y, et al. Computed tomography measurement of pulmonary artery for diagnosis of COPD and its comorbidity pulmonary hypertension. Int J Chron Obstruct Pulmon Dis. 2015; 10: 2525-2533.
- Ratanawatkul P, Oh A, Richards JC, Swigris JJ. Performance of pulmonary artery dimensions measured on high-resolution computed tomography scan for identifying pulmonary hypertension. ERJ Open Res. 2020; 6(1): 00232-2019.
- Tan RT, Kuzo R, Goodman LR, Siegel R, Haasler GR, et al. Utility of CT scan evaluation for predicting pulmonary hypertension in patients with parenchymal lung disease. Chest. 1998; 113(5): 1250-1256.
- Refini RM, Bettini G, Kacerja E, Cameli P, d’Alessandro M, et al. The role of the combination of echo-HRCT score as a tool to evaluate the presence of pulmonary arterial hypertension in idiopathic pulmonary fibrosis. Intern Emerg Med. 2021; 16: 941-7.