
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 6
Boerhaave syndrome resulting from psychogenic induced vomiting mistaken for hyperemesis gravidarum: A case report
Ioannis Boutas1*; Adamantia Kontogeorgi1; Panagiotis Krokos1; Nektarios Koufopoulos2; Pantelis Messaropoulos1; Antonios Makrigiannakis3; Sophia N Kalantaridou1
1National and Kapodistrian University of Athens, Attikon University Hospital, Rimini 1, 12462, Chaidari, Greece.
2Second Pathology Department, Attikon University Hospital, National and Kapodistrian University of Athens, Athens, Greece.
3Medical School, University of Crete, 13 Andrea Kalokairinoy Ave., 715 00 Giofirakia, Greece.
*Corresponding Author : Ioannis Boutas
National and Kapodistrian Unoversity of Athens, Attikon University Hospital, Rimini 1, 12462, Chaidari, Greece.
Tel: +30 6936829726;
Email: ioannis.boutas@gmail.com
Received : Dec 18, 2024
Accepted : Jan 09, 2025
Published : Jan 16, 2025
Archived : www.jcimcr.org
Copyright : © Boutas I (2025).
Abstract
Boerhaave syndrome is a rare and life-threatening condition characterized by spontaneous esophageal rupture, often associated with high mortality rates. Its diagnosis is traditionally based on the Mackler triad, requiring urgent recognition and intervention due to its low incidence. The condition is frequently misdiagnosed, particularly in cases resembling hyperemesis gravidarum. We report the case of a 31-year-old gravida 2, para 0 woman at 11 weeks of gestation, admitted with recurrent vomiting and significant electrolyte imbalance. The patient had a history of severe depression and psychogenic vomiting, as documented by her treating psychiatrist. Prior to conception, she experienced eating disorders with multiple episodes of vomiting over six months, ultimately precipitating Boerhaave syndrome. During hospitalization, the patient developed hematemesis secondary to esophageal rupture. Conservative management was implemented, resulting in a favorable outcome. The pregnancy culminated in delivery via cesarean section due to maternal hemodynamic instability, although Boerhaave syndrome itself is not an indication for surgical delivery. This case highlights the diagnostic challenges posed by Boerhaave syndrome, emphasizing the importance of accurate identification and timely intervention to avoid complications and achieve positive outcomes.
Keywords: Boerhaave syndrome; Esophageal perforation; Mediastinitis; Pneumomediastinum; Pregnancy; Stenotrophomonas maltophilia.
Citation: Boutas I, Kontogeorgi A, Krokos P, Koufopoulos N, Messaropoulos P, et al. Boerhaave syndrome resulting from psychogenic induced vomiting mistaken for hyperemesis gravidarum: A case report. J Clin Images Med Case Rep. 2025; 6(1): 3427.
Introduction
Boerhaave’s syndrome has a very rare occurrence and is one of the most lethal clinical conditions of the gastrointestinal tract. It can be characterized by a spontaneous rupture of the esophagus due to vomiting. This gastrointestinal disorder has been proven to be extremely lethal since the mortality rate in cases of its occurrence has been proven to be very high [1]. Spontaneous rupture of the esophagus without any underlying pathology was first described in 1724 by Hermann Boerhaave, a Dutch physician and professor of medicine at Leiden University [1]. The incidence of Boerhaave’s syndrome in the general population still remains unknown due to the fact that most cases are diagnosed as an autopsy finding [2]. The most common cause of Boerhaave syndrome is heavy vomiting, although it can be caused by other reasons that lead to an increase of intraesophageal pressure such as weightlifting, delivery, abdominal trauma and epileptic seizures. The triad of Mackler (intense vomiting, sudden chest pain and subcutaneous emphysema) is pathognomonic for the diagnosis of the syndrome [3]. Fever, hypotension and tachycardia are some other non-specific findings of the syndrome. The clinical symptoms for this syndrome may be unusual and bizarre, such as laughter during sleep or even a random asthma crisis [4]. It is imperative to diagnose this unusual condition in a very early stage in order to prevent severe complications such as infection or sepsis [3]. The authors present the case of a 31-year-old G2P0 woman in their 11th gestational week that was diagnosed with Boerhaave’s syndrome.
Case presentation
Patient information: A 31-year-old G2P0 woman was admitted to the emergency department at the 11th week of gestation due to episodes of projectile vomiting carrying on for 10 days prior to the date of admittance. The patient complained that she had around 10 episodes of vomiting per day during a 4-week period preceding her visit. Vomits would include food contents if they followed a meal. If not, the vomits consisted of gastric fluids with obvious traces of blood. From past medical history, the patient suffered from severe depression and had an eating disorder that took place before pregnancy. She was diagnosed and treated about the disorder without any medication.
Clinical findings: During the examination, the patient remained conscious and communicative but exhibited fatigue and dehydration indicators. Her skin lacked normal elasticity, and her mucous membranes were markedly parched. She was mentally oriented, although her speech was subdued. Her vital signs registered a blood pressure of 100/72 mmHg and a pulse rate of 87 beats per minute. Respiratory rate was stable at 16 respirations per minute, and she was fever-free with a temperature of 36.5°C. The patient had experienced a significant weight loss of 7 kilograms over the past four weeks, accounting for a 10% decrease from her original weight. Examination of the head, eyes, ears, nose, and throat did not show any paleness in the conjunctiva, but her mouth was notably dry. No yellowing of the skin was observed, and her neck veins appeared collapsed, suggestive of dehydration. The thyroid was of normal size without any nodules, and her overall demeanor did not convey any immediate distress. Her heart maintained a consistent and regular beat without any abnormal sounds. While her peripheral pulses were slightly quickened, there was no evidence of swelling in the extremities. The abdominal assessment revealed a pliable, pain-free abdomen with normal bowel activity. There was no sign of liver or spleen enlargement, and the size of the uterus corresponded with the expected stage of pregnancy. Neurologically, the patient was completely responsive, with no specific deficits detected. Her cranial nerve function was normal, as were her muscle strength and sensory responses.
Diagnostic assessment: Laboratory and imaging testing including blood tests and ultrasound examination were performed.
Laboratory examinations revealed electrolyte imbalance (Na=124 mmol/L, K=3,1 mmol/L) (Indicative normal values: Na=136-146 mmol/L, K=3,5-4,5 mmol/L). The remaining laboratory test results were normal (Hematocrit=28.1%, WBC=6280 K/μL, PLTs=201 K/μL, TSH=0.08 mlU/L). The sonographic examination of the upper abdomen revealed no pathology. The patient was admitted with the diagnosis of severe hyperemesis gravidarum for further investigation and treatment.
Therapeutic intervention: The physicians decided that the patient should carry on fasting and that she should be managed with intravenous hydration and electrolyte supplementation. During hospitalization the patient’s persistent vomiting continued but their clinical status remained stable. Sonographic evaluation of the pregnancy revealed normal findings. Following multiple episodes of vomiting, the family members of the patient were worried and asked for specialized, psychiatric help. After the patient was induced for hospitalization, they informed the physicians that all the episodes of vomiting were caused by the patient herself and were associated with her psychiatric disorder.Despite the psychiatric supervision during the hospitalization of the patient, the induced vomiting carried on.
Follow-up: Nine days after the patient’s admission, fever (up to 39.5oC) and weakness manifested. The patient underwent complete laboratory testing, including blood cultures which revealed a very rare aerobic, gram-negative, multi-drug-resistant pathogen called Stenotrophomonas maltophilia. The clinical condition of the patient, the elevated C-reactive protein (48,1 mg/L, normal values 0,00-6,00) and the presence of pancytopenia (HCT=20,5%, WBC=2180 K/μL, PLTs=70.000 K/μL) led to the diagnosis of sepsis. The patient was treated with piperacilline/tazobactam and ampicilline IV, which was replaced after two days with trimethoprim/sulfamethoxazole, based on the blood culture sensitivity report. On the 14th day of hospitalization, approximately on the 13th week of pregnancy, after several episodes of induced vomiting, the patient underwent an episode of massive hematemesis which resulted in severe anemia (HCT=13,7%, HB=4.7 g/dL) and hemodynamic instability (BP=78/55 mmHg, BPM=157). Due to criticality of the incident, gastroenterologists, thoracic surgeons, psychiatrists, anesthesiologists and intensive care specialists of the institution were summoned immediately. Red blood cells, platelets and fresh frozen plasma transfusion were administered to the patient. Following, the patient underwent an urgent upper gastrointestinal endoscopy under general anesthesia, which revealed a great tear in the wall of the lower third of the esophagus. In order to set the diagnosis of spontaneous rupture of the esophagus, a chest computerized tomography was performed, which indicated a pneumomediastinum and right pleural effusion as it is shown in (Figure 1). The patient was admitted to the Intensive Care Unit (ICU) and underwent another upper gastrointestinal endoscopy for esophageal stent placement under radiological guidance. The patient remained hemodynamically stable, and the pregnancy remained uneventful. After six days of hospitalization in the ICU, there was another episode of hemorrhage of the upper gastrointestinal tract. A new endoscopic evaluation revealed that the metallic stent has moved into the patient’s stomach. To cater for that, a metallic clip was inserted to secure the stent along with injections of adrenaline near the lesion. In the two weeks that followed after the patient’s last operation, her condition improved, and she was transferred to the High-Risk Pregnancy Unit of the Department. The patient was hospitalized for 81 days and her recovery was uneventful. The prolonged stay was due to multiple vomiting and electrolyte disorders. To ensure stability for delivery, the patient was schedule for a follow-up visit every two weeks until delivery. At the 34th week of pregnancy, as low abdominal circumference (< 5th percentile) and low estimated fetal weight (<2nd percentile) were revealed in ultrasound, a diagnosis of intrauterine growth restriction (IUGR) was made. The fetal umbilical artery and middle cerebral artery Doppler evaluations appeared normal.

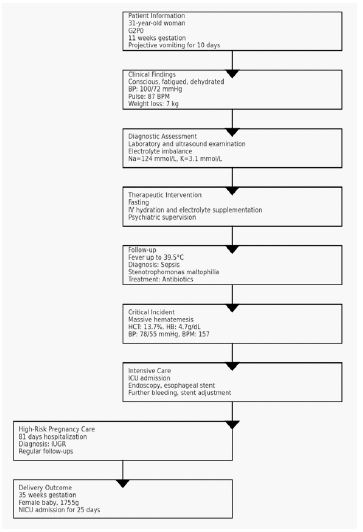
Outcomes: The patient delivered a female baby by cesarean section in the 35th week of pregnancy, weighing 1755 g; Apgar scores were 9 at the 1st minute and 10 at the 5th minute. The newborn was admitted in the Neonatal Intensive Care Unit for 25 days. We summarize information from the case as a timeline in (Figure 2).
Discussion
Boerhaave’s syndrome is infrequent during pregnancy; only a few cases have been reported in the literature [1-8,4-7,5-9]. The syndrome tends to be spontaneous and is associated with excessive vomiting. Although hyperemesis gravidarum is a very common complication during the first trimester of pregnancy, it can rarely become extremely dangerous due to the nature of this life-threatening emergency complication called the Boerhaave’s syndrome, as described previously [9]. Hyperemesis gravidarum associated with electrolyte imbalance and weight loss is a challenging situation for any Obstetrician. Vomiting is the most common accompanying symptom of Boerhaave’s syndrome during pregnancy and can lead to severe complications such as electrolyte disorders, coma, seizures or cardiac arrest [1,3]. Interestingly, there appears to be a case of esophageal rupture during the second stage of labor which possibly occurred due to prolonged active pushing [5]. The patient in this study was hospitalized for electrolyte disorders due to hyperemesis.This led to electrolyte imbalance and sepsis due to occult esophageal rupture, which occurred because of repeated episodes of projectile vomiting. During the occult phase of the esophageal rupture, pathogenic microorganisms colonized the mediastinum through the esophageal tears and caused mediastinitis, leading to high fever, weakness, sepsis and finally massive hematemesis. Stenothophomonas maltophilia was the pathogen that was isolated from the first result set of blood cultures. It is an aerobic, gram-negative, multidrug-resistant pathogen known for its high mortality rate in immunocompromised patients with bacteremia [9]. The most common manifestations of a Stenothophomonas maltophilia infection is pneumonia and bacteremia [9]. The collaboration of different medical specialists for the management of the presented case and patient was crucial. Boerhaave’s syndrome is characterized by an extremely rapid deterioration of the patient’s health, with high morbidity and mortality [8]. The differential diagnosis of this severe complication includes tension pneumothorax, dissection of thoracic aorta, cardiac tamponade and major gastrointestinal hemorrhage examinations [10]. Hematemesis, when present, makes the diagnosis clearer, which was the case in the presented study. The prognosis is highly dependable on the time of the diagnosis; a delay of the latter can increase the mortality rate to as high as 100% [6]. The patient should undergo therapeutic management as soon as possible after the first signs and manifestation of the syndrome in order to avoid the cardiovascular instability and reduce the effects of sepsis. The data gathered from various published research studies regarding the most appropriate therapeutic approach leads to a controversial outcome; in most cases the management was conservative but there were incidents of surgical management during pregnancy [1-3,5-10]. The main principles for managing this condition consist of prevention for further contamination of the mediastinum with pathogens, administration of wide spectrum antibiotics and parenteral feeding [10].
Most cases of Boerhaave’s syndrome during pregnancy were reported during the first trimester, mimicking symptoms of hyperemesis gravidarum [6,8,10] and only in one case it manifested during a prolonged second stage of labor [8]. All cases in the literature were uneventful after conservative management [1-3,5-10] - except for one case where the patient underwent a thoracotomy after diagnosis of the esophageal rupture [10]. To the best of the authors’ knowledge, this is the first case of Boerhaave’s syndrome and pneumomediastinum that occured due to psychogenic vomit during the first trimester of pregnancy; most reported cases were secondary to hyperemesis gravidarum. The institution’s psychiatry specialists’ contribution was significant in managing this case. Bulimia and anorexia were both eating disorders that the patient suffered from but were excluded as a cause for vomiting. Psychogenic vomiting is defined as a vomiting without an obvious organic pathology. The patient was diagnosed with a major depressive disorder. The frequency of the episodes decreased gradually after treatment with sertraline (SSRI) and benzodiazepines that was instructed by the institution’s specialists. The patient’s condition improved after the treatment with SSRIs. The patient delivered a healthy female baby by cesarean section due to an obstetric indication of IUGR.
Conclusion
Boerhaave’s syndrome is a rare, uncommon and extremely lethal clinical condition. It can result from psychogenic vomiting. This can result in sepsis following bacterial colonisation of blood. The authors present a case of Boerhaave’s syndrome occurring due to psychogenic vomiting, anxiety distress and severe depression in a 31-year-old G2P0 pregnant woman.
The esophageal rupture led to sepsis and colonization of pneumomediastinum with Stenothophomonas maltophilia. Taking into consideration the fact that the septic symptoms preceded hematemesis for almost a week, it is crucial to mention that early recognition and multidisciplinary care greatly improves the outcome. Eluding timely diagnosis can lead to a fatal outcome. In our case, early diagnosis and care resulted in a good outcome.
Declarations
Informed consent and patients perspective: In the preparation of this case study, explicit informed consent was obtained from the patient involved. This crucial step ensures adherence to ethical standards and respects the patient’s autonomy and privacy. The patient was thoroughly informed about the nature and purpose of the case report, including how their medical information would be used and presented in the study. They were also assured that their identity would be kept confidential and that all personal identifiers would be removed or altered to maintain anonymity. Only after understanding these aspects and agreeing to participate, did the patient provide their written consent, thereby endorsing the use of their medical data for educational and scientific purposes. This process underscores the commitment to ethical medical practices and the importance of patient rights in clinical reporting. In the development of this case study, we meticulously respected and integrated the patient’s perspective, recognizing its fundamental importance in providing comprehensive and compassionate healthcare. From the outset, we engaged in open, empathetic communication with the patient, ensuring that their experiences, concerns, and preferences were not only heard but actively considered in every phase of the study. This approach enabled us to understand the patient’s unique viewpoint, including their perceptions of their condition, treatment experiences, and expectations from the healthcare system. By doing so, we ensured that the case study reflects not just the clinical aspects of the patient’s condition but also their personal journey and challenges, providing a holistic view of their healthcare experience. This patient-centered approach not only enriched the depth and relevance of our study but also upheld the principles of ethical and empathetic medical practice, demonstrating our commitment to respecting and valuing the patient’s voice in their healthcare narrative.
Statement of ethics: The authors hereby declare that the research material presented in this study has been conducted ethically in accordance with the World Medical Association declaration of Helsinki.
Conflicts of interest statement: The authors declare no conflict of interest.
Funding: No funding has been given for this study. None of the authors has any financial interest in the information contained in this manuscript.
Authors’ contributions: Ioannis Boutas and Adamantia Kontogeorgi had equal contribution in conceptualizing and designing the study and gathering the data. Adamantia Kontogeorgi, Ioannis Boutas, Panagiotis Krokos, Nektarios Koufopoulos and Pantelis Messaropoulos contributed to the drafting of the manuscript. Sophia Kalantaridou and Antonios Makrigiannakis had the conceptualization and appropriate revision of the article.
References
- Rokicki M, Rokicki W, Moj M, Bsoul T, Rydel M. Boerhaave Syndrome-over 290 years of surgical experiences. Can the disorder recur? Pol Przegl Chir. 2018; 91(3): 27-9.
- Henderson JA, Peloquin AJ. Boerhaave revisited: Spontaneous esophageal perforation as a diagnostic masquerader. Am J Med. 1989; 86(5): 559-67.
- Lieu MT, Layoun ME, Dai D, Soo Hoo GW, Betancourt J. Tension hydropneumothorax as the initial presentation of Boerhaave syndrome. Respir Med Case Rep. 2018; 25: 100-3.
- Necdet OZ, Ahmet BK. Esophageal Stenosis as a Cause of Spontaneous Esophageal Perforation(Boerhaave Syndrome): A Case Report and Explanation of Possible Mechanism. J Trauma Treat 2016; 5: 3.
- Whelan S, Kelly M. Pneumomediastinum following a prolonged second stage of labor-an emphasis on early diagnosis and conservative management: a case report. J Med Case Rep. 2017; 11(1): 313.
- Rissoan C, Louerat C, Riou R, Lantheaume S. Boerhaave syndrome and pregnancy. A case report and review of the literature. J Gynecol Obstet Biol Reprod (Paris). 2009; 38(3): 250-3.
- Kim EJ, Kim YC, Ahn JY, Jeong SJ, Ku NS, et al. Risk factors for mortality in patients with Stenotrophomonas maltophilia bacteremia and clinical impact of quinolone-resistant strains. BMC Infect Dis. 2019; 19(1): 754.
- Eroglu A, Kurkcuoglu C, Karaoglanoglu N, Tekinbas C, Cesur M. Spontaneous esophageal rupture following severe vomiting in pregnancy. Dis Esophagus. 2002; 15(3): 242-3.
- Blencowe NS, Strong S, Hollowood AD. Spontaneous oesophageal rupture. BMJ. 2013; 346: 3095.
- de Schipper JP, Pull ter Gunne AF, Oostvogel HJ, van Laarhoven CJ. Spontaneous rupture of the oesophagus: Boerhaave’s syndrome in 2008. Literature review and treatment algorithm. Dig Surg. 2009; 26(1): 1-6.