
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Research Article - Open Access, Volume 6
Youth friendly reproductive health service utilization and associated factors among preparatory school students in Addis Ababa, Ethiopia: The school-based mixed research design
Hiwot Belay*; Wondimye Ashenafi
Center for Population Studies, College of Development Studies, Addis Ababa University, Sidist Kilo Campus 1176, Ethiopia.
*Corresponding Author : Hiwot Belay
Center for Population Studies, College of Development Studies, Addis Ababa University, Sidist Kilo Campus 1176, Ethiopia.
Email: hiwotbelay711@gmail.com
Received : Nov 30, 2024
Accepted : Jan 21, 2025
Published : Jan 28, 2025
Archived : www.jcimcr.org
Copyright : © Belay H (2025).
Abstract
Background: Youth make up a large, important, and rapidly growing segment of Ethiopia’s population, but they account for a disproportionately high proportion of the country’s unmet reproductive health needs. Promoting comprehensive youth-friendly services is critical for assisting young people in making responsible reproductive Health decisions and empowering them to follow through on those decisions. Great majority of youths in school are undeserved for utilizing users’ friendly services due to lack of awareness to the service, poor communication on reproductive health issues and inadequate service and counselling specifically targeted for this specific youth group.
Objective: To assess of youth friendly sexual and reproductive health service utilization among preparatory schools students in Addis Ababa, Ethiopia.
Methods: The school based cross-sectional study with qualitative approach was conducted to evaluating YFRHS utilization and related factors among Addis Ababa city preparatory school students. From April 2021 to July 2021 the data collection was carried out. Multistage clusters sampling technique was used on a total of 695 sampled students by proportionally allocated to the selected government and private school. Logistic regression analysis performed on important predictor variables and odds ratio was used to determine the factors that predict the utilization of YFRHS with p- value of <0.05 as measure of statistical.
Result: The study participants were 695 students, with 100% response rate. Only 73(11%) of students had ever used the service in the past twelve months, among them most of the respondent 572(82.3%) had heard about YFRHS, More than half of the study participant 443(63%) had knew where they could find YFRHS delivered. According to this study the main factors that affecting utilization of youth friendly reproduction health service was the study participants altitude which was negative toward the importance of YFRHS it was manifested through qualitative study.
Conclusion and recommendation: The study result shows low utilization of reproductive health service among the participant student due to negative attitude and benign less awareness about usefulness of youth friendly reproductive health service, the stake-holder should give more focus than ever on the YFRHS implementation and follow the service provided under YFRHS.
Keywords: Youth; Reproductive health; YFRHS; Utilization.
Abbreviations: AIDS: Acquired Immune Deficiency Syndrome; EDHS: Ethiopian Demographic Health Survey; ESAA: Education Statistics Annual Abstract; HIV: Human Immune- Deficiency Virus; IEC: Information, Education and Communication; MOH: Minster of health; MOE: Minster of Education; NGO: Non-Governmental Organization; RH: Reproductive Health; RHS: Reproductive Health Service; SPSS: Statistical Package for Social Science; SRH: Sexual and Reproductive Health; STD: Sexually Transmitted Disease; STI: Sexually Transmitted Infection; VCT: Voluntary Counseling and testing; WHO: World Health Organization; YFRHS: Youth friendly Reproductive Health Service.
Citation: Belay H, Ashenafi W. Youth friendly reproductive health service utilization and associated factors among preparatory school students in Addis Ababa, Ethiopia: The school-based mixed research design. J Clin Images Med Case Rep. 2025; 6(1): 3442.
Introduction
There is 1.2 billion youth in the world by 2018 which accounts one out of every six people worldwide. In Africa, there is 226 million youths live which accounts 19 percent of the global youth population (www.unpopulation.org). In East and Southern Africa, youth make up more than a third of the population. By 2050, the population of 15-24 year olds is predicted to grow to 341 million, up from 182 million today. For most young people, this is a time when they are confronted with a variety of reproductive health issues, such as early and unintended pregnancy, HIV and sexually transmitted infections, and child marriage. Investing in young people’s education and health at the correct time helps them grow into healthy adults who can contribute to the economy [1]. According to UN numbers, Ethiopia’s population was expected to reach 114,963,588 people by 2020 [2]. Ethiopia has the second-largest population in Sub-Saharan Africa, with more than half of the population under the age of 25. Since they lack sufficient education, adventure, and advice about reproductive health and related matters, youth all over the world are vulnerable to reproductive health risks [3]. In Ethiopia, youth make up a huge, significant, and rapidly increasing demographic, and they account for a disproportionately high proportion of the country’s unmet reproductive health needs. Promoting robust youth-friendly programs is critical in assisting young people in making informed sexual and reproductive choices and encouraging them to follow through with those decisions [4]. WHO defined youth are as persons between 15 and 24 years of age who are identified by significant physiological, psychological and social changes that expose their life at high risk and contains about 20% of the world population, of whom 85% live in developing countries (WHO). In Ethiopia, youth accounts 20.4% of the total population. Youth is also regarded as the healthiest stage of life, but it is also a time when young people are exposed to a unique range of health and survival challenges. They are often faced with choices that can have far-reaching consequences for their potential morbidity and mortality risks. Unprotected sexual activity, Sexually Transmitted Infection, HIV/AIDS, illegal abortion, premature pregnancy, failure to meet family planning requirements, and excessive alcohol intake are all risks that young people face [5,6].
The commitments made by governments at the 1994 International Conference on Population and Development (ICPD) included support of youth sexual and reproductive health, as documented in the program of Action. Since the ICPD, achievements in improving the health of youth, in particular young girls, have linked or integrated essential components of Reproductive Health and Rights (RHR), such as comprehensive RH education (CSE) and provision of quality Reproductive Health (RH) services, with efforts to create safe and supportive youth-friendly environments at schools, health-care facilities and other venues in the community. Packages of interventions have been used to address SRH problems such as early and/or unintended pregnancy, unsafe abortion, sexually transmitted infections (STIs), including HIV, However, many challenges remain if we are to provide services that meet their RH needs [6]. Across a variety of global contexts, it has been demonstrated that YFRHS can address this situation by improving the availability, acceptability, accessibility, and equity of health services for young people [7]. Youth-friendly, accessible, and confidential options are limited. Furthermore, the environment in which sexual and reproductive health services are delivered is often insensitive to the unique needs of this demographic of young people. Little is known about the level of utilization to the standard and the predators that influence the utilization [8]. Recognizing that adolescents are vulnerable to reproductive health issues, the Ministry of Health (MOH) has developed a national strategy with a minimum service package for scaling up adolescent and youth reproductive health services. High rates of maternal mortality and morbidity due to abortion, fistula, and other pregnancy-related complications are thought to be due to limited access to and use of adolescent and youth-friendly reproductive health services. (MOH, 2019/2020) YFRHS programs are an approach that combines the values that young people seek with the high standards that the best public services must meet. Such programs are accessible, appropriate, and affordable for young people. They’re in the right place at the right time, for the right price (free whenever possible), and presented in a way that appeals to young people. They’re fair because they’re all-inclusive, meaning they don’t discriminate against any segment of this young clientele based on gender, race, religion, disability, social status, or any other factor. They do reach out to the most vulnerable and insecure people [4].
The aim of this study was to assess youth friendly reproductive health service utilization and associated factors among preparatory school students in Addis Ababa, Ethiopia.
Research methodology
The school-based mixed research was conducted using both qualitative and quantitative methods, the study was take place in Addis Ababa, the capital city of Ethiopia. The study participant were all students aged from 15-24 years who were selected and available during the study period at preparatory school in Addis Ababa. The study was conducted over a period of a months. The data collection was carried out from April 2021 to July 2021. A single population proportion formula is used to estimate the sample size. From the study conducted in Debre Tabor town taking youth friendly sexual and reproductive health service utilization as 28.8% [9] a confidence level of 95%, marginal error of 5%, design effect of 2 and adding 10 percent non- response rate. The final total sample size was 695.
A multi stage cluster sampling method was used to select the study participants. There were 222 schools, where73 governmental and 148 private preparatory schools in Addis Ababa. The total number of students is 50,566 in both governmental and private preparatory schools according to (ESAA, 2018\2019). The calculated sample size was proportionally allocated for the number of students in each of the school types (i.e. Governmental and private schools). Accordingly, 3 governmental and 2 private secondary and preparatory schools has been first selected randomly. Then, 24 sections (8 sections for each selected school) from a total of 184 sections of the governmental schools were randomly selected. Similarly, 6 sections were randomly selected from total of 12 section private preparatory sections. The study eligible participants from these randomly selected sections would be systematically selected using the list of student’s ID number as a sampling frame. A total of students from governmental where 600 and 95 from private preparatory schools was be considered eligible for the study.
The questionnaire contains socio-demographic characteristics, health system factors and knowledge related factors and utilization parts. For quantitative approach data was collected using a structured, self-administered questionnaire. Two Health officer and one teacher was recruited to participate as supervisors in data collection. The supervisors was selected from those residing in the study area and fluent in local language such as Amharic. The supervisors was takes through a two days training; the training which focuses on administration of questionnaires, interviewing techniques and reading through all the questions and agreeing on the way of asking respondents in Amharic language/Local language for the qualitative study investigation, we were use a non-probability sampling approach called Purposive sampling, which was result in four In-Depth Interviews (IDIs), two of which was conducted with school stockholders and the other two with YFRHS providers from governmental and private health care facilities. A Face-to-face interview with research participants was conducted using an unstructured approach (open ended questions). For the interview, the interview guides were written in English and then translated into Amharic. Every interview lasted between 45 and 50 minutes, depending on the respondent’s level of detail. In addition, six Group Discussions (FGDs) was held, three with female students and three with male students. Each group was consisting of 5 to 7 youths who was chosen from the school. The conversations was moderated using a pre-prepared discussion guide that has been pre-tested with students from a school that is not participating in the survey. The FGDs were administered in a private and quiet atmosphere by a moderator of the same sex. The talks lasted about an hour on average. The FGD will be completely taped and registered, with the moderator’s assistants taking notes.
Results
Socio-demographic characteristics of study participants: The study involved 695 participants, and every single one of them completed the questionnaires, resulting in a 100% response rate. Nearly half of the respondents (55.1%) were male students, with the remaining (44.9%) were female. The majority of the participants (66.7%) were ages between 15 to 18 years, and the rest were of 19-22 years old. The majority of them (86.3%) were attendants of governmental schools (Table 1).
Knowledge on reproductive health and YFRHS: The study participant student as reported that they got information from different source about reproductive health issue, according to this (45.9%) of respondent got information from radio, followed by (42.9%) of respondent got information from their peer the reaming participant got information from different source as indicated in Figure 3.
In terms of knowledge on YFRHS, most of the respondents (82.3%) claimed they have heard about it, with higher proportion of the knowledge was about VCT services (44.2%). According to awareness on the right of youth getting reproductive health service, a great deal of the participants (78.7%) reported that they knew their rights of the services (Table 2).
Out of the total study participant student only 167(27%) of them were reported that they had parental discussion about the reproductive health issue. According to the study participant knowledge of STI, half of them (52.7%) respondent reported that they had ever heard about sexual transmitted infection. The most commonly reported sexual transmitted infection was HIV/AIDS (50.5%) followed by syphilis (22.3%) (Table 3).
Health system factors: Most of the study participant students 569(81.9%) had awareness about the presence of youth friendly reproductive health service provider facility around their living compound. About 426(61.3%) of the respondent students mentioned that they were asked to pay for the service they got and only 149(21.4%) of them said that they were not asked to pay. According to the working hours of health facility which provided youth friendly reproductive health service 380(54.7%) of the study participant students were agree that was convenient to them, but 195(28.1%) of them were not agree on the convenient of service provided time. Among those who were asked about their optional time that was convenient to use the service 51(7.3%) said that afternoon was convenient to them, followed by 144(20.7%) of them also mentioned that weekend was convenient time to them. The distance of health facility from their residence was estimated by the time interval to reach heath center, so that 62(8.9%) of respondent said that it takes 5-10 minutes, 159(22.9%) 15-30 minute, 224(32.2%) 45 min-1 hours and 3(0.4%) 1-2 hours respectively for a single journey to reach the health center from their living area to utilize YFRHS.
Prevalence of youth friendly RH service utilization: About a tenth (11%) of study participants reported they have ever used the YFRH services in the past twelve months.
The study participant reported that they use different health facility, to received youth friendly reproductive health service, according to this (8.3%) of the respondent received from different governmental and private hospitals (1.7%) of them received from health center.
Factors associated with youth friendly reproductive health service: Utilization of youth friendly reproductive health service was assessed for its association with predicting variables. On the bivariate analysis sex of respondents, age of respondents, types of school which student learning, living arrangement, mothers educational status, having pocket money, heard about of YFRHS provided service, knew about YFRHS provide such that condom use, source information about RH service from peer/friend, discussion of RH issue with their parents, knew about STI disease such as HIV/ADIS, knowledge of STI symptoms such as genital ulcer and itching, the presence of YFRHS in the living area, convenient working hour of health facility and utilization of reproductive health service in the past 12 months were found to be significantly associated.
The variable which were significant on bivariate were entered into multivariate logistic regression analysis. After that being male respondents, age of respondent between 17-18 years old, being governmental school student, living with mother only, maternal education being secondary school, preparatory school and above, heard of YFRHS provide STI treatment, knew YFRHS provide condom use, discuss about RH with parents, knew about STI such as HIV/AIDS, knew symptom of STI genital ulcer, knew symptom of STI genital itching, the presence of YFRHS in living area, convenient working hour of health facility remained significantly and independently associated with YFRHS utilization. The odds of utilizing YFRHS were 2 times higher (AOR=2.531, 95% CI: 1.66, 4.37) among male participants as compared to females. Also, the utilization of service among those age group of 17-18 were 82% times lower than those of other age group (ACR=0.187, 95% CI: 0.044,0.794). Governmental school student were low utilize YFRHS than the private school student (AOR= 0.243, 95% CI: 0.141, 0.419). According to study participants those who live with their mother 93% of them not utilize YFRHS than other (AOR=0.061, 95% CI: 0.008, 0.496). The study participant source of information which is peer were higher to utilize YFRHS than other source of information (AOR=1.374, 95% CI: 0.822, 2.297). Those study participant who had parental discussion on RH issue were low to use YFRHS than their counterpart (AOR=0.197,95% CI: 0.083,0464). Participants in the study who knew the STI symptom of genital itching and genital ulcer were double times and four times higher to use the RH service respectively, than those of who doesn’t knew STI symptom (AOR=4.211,95% CI: 2.486,7.131), (AOR= 2.91,95% CI: 1.735,4.882). Among the study participant those who found YFRHS around there living area 60% of them were low utilized the service than other (AOR= 0.4 95% CI: 0.235, 0.682). Those who utilize YFRHS were two times got the working hour convenient to them than not utilize (AOR=2.431 95% CI: 1.154, 5.121).
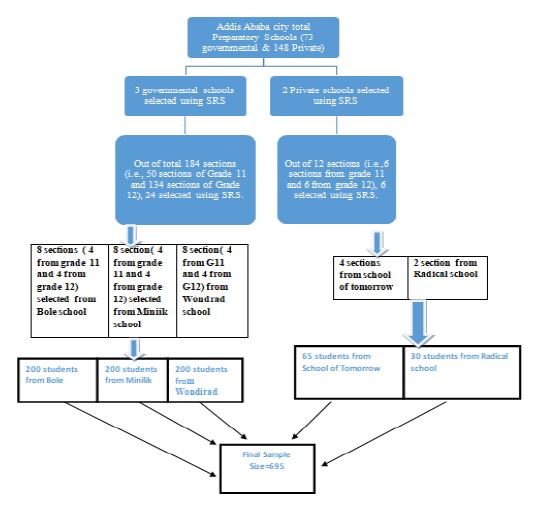
Table 1: Demographic characteristics of students (n=695).
| Variable | Frequency | Percent (%) | |
|---|---|---|---|
| Gender | male | 383 | 55.1 |
| female | 312 | 44.9 | |
| Total | 695 | 100 | |
| Age | 15-18 years | 464 | 66.7 |
| 19-24 years | 231 | 33.3 | |
| Total | 695 | 100 | |
| Marital status | single | 692 | 99.6 |
| married | 3 | 0.4 | |
| Total | 695 | 100 | |
| Educational Level | grade 11 | 347 | 49.9 |
| grade 12 | 348 | 50.1 | |
| Total | 695 | 100 | |
| School Type | governmental | 600 | 86.3 |
| Private | 95 | 13.7 | |
| Total | 695 | 100 | |
| Religion | Orthodox | 668 | 96.1 |
| Muslim | 11 | 1.6 | |
| Protestant | 7 | 1 | |
| Catholic | 9 | 1.3 | |
| Total | 695 | 100 |
Summary of qualitative study finding
Demographical characteristic of FGD and key informant interview: Due to the sensitivity of the subject matter and the difficulty of genuinely reporting youth related RH issues, the study was better to supplemented by a qualitative approach to explore in greater depth the underlying behaviors, attitudes, and perceptions that may have an impact on YFRHS. The study was conducted on 6 Focus Group Discussion (FGD), three with female student and the other three with male student, in each discussion five to seven study participant was involved. The study participant was selected from two governmental and one from private school by purposively sampling technique with a consideration of sex of convenient students during FDG, also the study conducts the key informant heath provider during interview session with three health provide, according to that two nurse from Efoyta health center that found in kirkos sub city werda 02, and from Bole private health center participated respectively. The other interview was made from the school club that provide reproductive health service such as VCT and IEC. Table 3 represent the background characteristics of FGD participant.
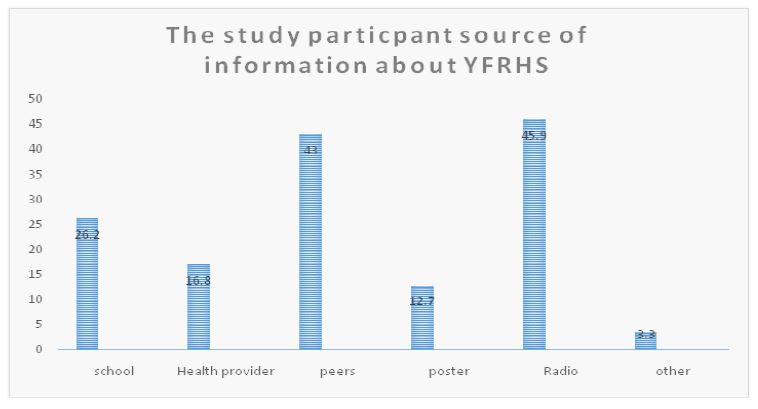
Table 2: Shows the study participant knowledge about YFRHS.
| Variable | Frequency | Percent (%) |
|---|---|---|
| Ever heard YFRHS | ||
| Yes | 572 | 82.3 |
| No | 123 | 17.7 |
| Total | 695 | 100 |
| Knew service provided under YFRHS | ||
| FP | 236 | 34 |
| STI | 63 | 9.1 |
| VCT | 307 | 44.2 |
| Abortion service | 61 | 8.8 |
| ANC | 231 | 33.2 |
| Health education | 42 | 6 |
| Condom use | 158 | 22.7 |
| Other | 48 | 6.9 |
| Knew where to get YFRHS | ||
| Health center | 443 | 63.7 |
| Drug shop | 99 | 14.2 |
| Traditional healer | 24 | 3.5 |
| Other | 6 | 0.9 |
| Total | 572 | 82.3 |
| Knew had right to use service | ||
| Yes | 547 | 78.7 |
| No | 25 | 3.6 |
| Total | 572 | 82.3 |
| Knew any family planning | ||
| Condom | 419 | 60.3 |
| Implant | 326 | 46.9 |
| Pills | 232 | 33.4 |
| IUCD | 119 | 17.1 |
| Injectable | 215 | 30.9 |
| Other | 118 | 17 |
Table 3: The study participant knowledge of STI.
| Variable | Frequency | Percent (%) |
|---|---|---|
| Ever heard of STI | ||
| Yes | 366 | 52.7 |
| No | 206 | 29.6 |
| Ever heard of STI | ||
| Syphilis | 155 | 22.3 |
| Gonorrhea | 127 | 18.3 |
| Cancroid | 70 | 10.1 |
| HIV/AIDS | 351 | 50.5 |
| Other | 27 | 3.9 |
| Knew sign/symptom of STI | ||
| Genital Ulcer | 116 | 16.7 |
| Genital discharge | 65 | 9.4 |
| Genital itching | 150 | 21.6 |
| Genital burning sensation | 136 | 19.6 |
| Other | 121 | 17.4 |
| Mode of STI transmission | ||
| Mother to child | 101 | 14.5 |
| Contact with infection blood | 116 | 16.7 |
| Unprotected sexual intercourse | 183 | 26.3 |
| Using sharp materials withinfected person | 164 | 23.6 |
| Other | 97 | 14 |
Knowledge about youth friendly reproductive health service: More than half of those who took part in the focus group agreed that they had heard about reproductive health services but didn’t know much about the service provided under YFRHS. The information they had seems not well structured, and it appeared fragmented; the majority of information came from unreliable sources such as peers those who not specially trained on This has an impact on student IEC and professional support for their basic RH requirements. A male FDG participant said ‘I don’t know about any of you mentioned services, the only thing I know is that once a year we have a celebrity HIV/AIDS day in our school, after all of this, I’m afraid I can’t think of any other service. Some of the participants were familiar with STI disease and transmission modes, and the majority of those who were familiar with STI were also familiar with HIV/AIDS and syphilis. The students believed they had the right to use RH services, but the majority of them were embarrassed to discuss the RH issue with their parents. In the key informant interview, the participant stated that students engage in a variety of risky behaviors such as peer pressure, unsafe sex, drug abuse, exposure to sugar mom or dad, and pornography, these risky behaviors have an impact on youth’s reproductive health. Some policies and strategies were established by the government and Non-Governmental Organizations (NGOs), but they were hampered by a lack of follow-up. There was a lack of well-trained professionals, equipment, and facilities to provide the service in the school setting. The only service available to the student was IEC, and they attempted to communicate with their parents whenever possible, but this was insufficient.
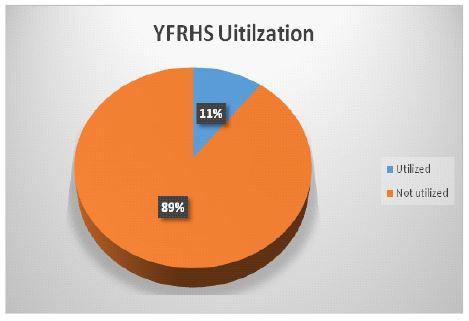
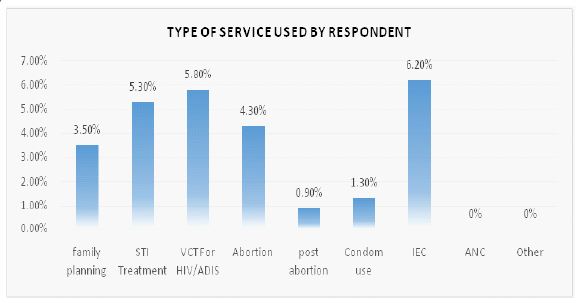
Table 4: Factors associated with utilization of YFRHS.
| Variables | Category | YERHS Utilization | COR (95%,CI) | AOD(95%,CI) | |
|---|---|---|---|---|---|
| Yes | No | ||||
| Gender | Male | 54(14%) | 329(85.9%) | 4.186(2.209, 7.933)** | 2.531(1.66,4.37)** |
| Female | 19(6%) | 293(93.9%) | 1 | 1 | |
| Age | 15-16 years | 34(16.9%) | 167(83%) | 7.156(2.78,18.421)** | 1.629(0.464,5.717) |
| 17-18 years | 6(2.2%) | 257(97.75) | 0.447(0.174,1.146)* | 0.187(0.044,0.794)* | |
| 19-20 years | 30(14.75) | 174(85.2%) | 7.156(2.78,18.421)** | 1.379(0.391,4.869) | |
| 21-22 years | 3(11.1%) | 24(88.8%) | 1 | 1 | |
| School type | Governmental | 48(8%) | 552(92%) | 0.155(0.078,0.309)** | 0.243(0.141,0.419)* |
| Private | 25(26.3%) | 70(73.6%) | 1 | 1 | |
| Living arrangement | With both mother and father | 60(13%) | 399(86.9%) | 1.662(0.363,7.616) | 0.902(04.24,1.922) |
| With father only | 3(6%) | 47(94%) | 4.659(0.406,53.392)** | 0.383(0.098,1.498) | |
| With mother only | 1(1%) | 98(98.9%) | 9.67(0,0) | 0.061(0.008,0.496)** | |
| With friends | 0 | 0 | 1 | 1 | |
| Mother educational status | No formal education | 33(32%) | 70(67.9%) | 44.292(138.50,0.088)** | 0.578(0.308,1.085) |
| Primary school | 6(1.8%) | 322(98.1%) | 361966.215(0.00,0) | 0.023(0.009,0.058)* | |
| Secondary education | 3(1.5%) | 192(98.4%) | 20616.512(0,0) | 0.019(0.006,0.066)** | |
| Preparatory schooland above | 31(44.9%) | 38(55%) | 1 | 1 | |
| Father educational status | No formal education | 6(6.25%) | 90(93.7%) | 0.407(0.163,1.012)* | 0.086(0.034,0.219)** |
| Primary school | 30(14%) | 183(85.9%) | 107698324.4 | 0.213(0.119,0.379)** | |
| Secondary education | 301(100%) | 0.086(0.034,0.219)** | 3.558E11(3.558E11,3.558E11) | ||
| Preparatory schooland above | 37(43.5%) | 48(56.4%) | 1 | 1 | |
| Have you for daily expenses | Yes | 34(13%) | 227(86.9%) | 5.918(2.763,12.6790** | 1.517(0.931,2.471) |
| No | 39(8.9%) | 395(91%) | 1 | 1 | |
| Source of information from peers | Yes | 43(14.4%) | 255(85.5%) | 9.901(2.127,46.08)** | 1.374(0.822,2.297) |
| No | 27(10.9%) | 220(89%) | 1 | 1 | |
| Have you ever discussed about RH withpatent | Yes | 6(3.5%) | 161(96.4%) | 0.197(0.083,0.64)** | 0.197(0.083,0464)** |
| No | 64(15.9%) | 338(84%) | 1 | 1 | |
| New symptoms of STI genital ulcer | Yes | 40(34.4%) | 76(65.5%) | 0.007(0.001,0.081)** | 4.211(2.486,7.131)** |
| No | 33(11.1%) | 264(88.8%) | 1 | 1 | |
| New symptoms of STI genital itching | Yes | 42(28%) | 108(72%) | 57.357(3.937,835.705)* | 2.91(1.735,4.882)** |
| No | 31(11.7) | 232(88.2%) | 1 | 1 | |
| Where a YFRHS in your living | Yes | 49(8.6%) | 520(91.3%) | 0.4(0.235,0.682)** | 0.4(0.235,0.682)* |
| No | 24(19%) | 102(80%) | 1 | 1 | |
| Working hour of the health | Yes | 40(10.5%) | 340(89.47) | 2.431(1.154,5.121)** | 2.431(1.154,5.121) |
| Convenien time for you | No | 9(4.6%) | 186(95.38) | 1 | 1 |
*= Significant at P-value < 0.05 and *=Significant at P-value < 0.25.
Table 5: Demographic characteristics of FGD participant students.
| Characteristics | Frequency | Percent (%) | |
|---|---|---|---|
| Gender | Male | 24 | 54% |
| Female | 20 | 47% | |
| Age | 15- 19 | 44 | 100% |
| 20- 24 | |||
| Religion | Orthodox | 38 | 87% |
| Muslim | 2 | 5% | |
| Protestant | 3 | 7% | |
| Catholic | 1 | 1% | |
| Marital status | Single | 44 | 100% |
| Married | |||
| Education | Grade 11 | 14 | 32% |
| Grade 12 | 30 | 66% | |
| School type | Governmental | 28 | 64% |
| Private | 16 | 36% | |
Attitudes and exposure toward youth friendly reproductive health service: The majority of FGD participants believe they should be aware of their own reproductive health needs and protective measures, but they do not use the YFRHS service. One female respondent expressed her dissatisfaction with the service by saying, Now that we are students, our focus should be on our educational status, we don’t have time for such kind of staff, but if we get involved in such risky behavior, we can easily access the YFRHS service. Some participant student was aware of the current RH service, but the main challenge was that it was provided in conjunction with other health services because YFRHS lacked a dedicated area for providing the service. Client confidentiality was jeopardized as a result of this. The service must be provided in a separate area for the youth. They were embarrassed when their colics and other compound members saw them. Also, the health providers’ attitudes toward the students were not friendly; students were afraid to tell what had happened to them or they didn’t share their story with the RHS provider. It has an impact on YFRHS usage. The female FGD participant express her idea to ward the health provider altitude’s by emotional way ‘‘The health providers, not all but most of them, were blaming us for being exposed to risky behavior rather than educating us, we were considered as a faulty or guilty person, for that reason most of us prefer not to go to the health center instead we use a pharmacy as a safe way of getting treatment. The other factors that the participant listed out was cost of service. Whether it is governmental or private health center most of them ask to pay for the service they received, unless it was family planning implementation. The key informant participant, on the other hand, stated that YFRHS could be found in every health center and some selected non-governmental organizations at a low cost with well-trained health professionals on reproductive health issues, also health provider’s attitude toward their client was good, which they developed through experience and that they also received some refresher training based on youth behavioral and their need. In some private health centers, the service is also available at a reasonable cost. ‘‘I believe the problem was an informational gap; most of the students were not using the service, which could be due to a lack of awareness, the stake holder should focus on awareness creation” one health provider said.
Discussion
This study tried to determine youth friendly reproductive health service utilization and its associated factors among preparatory school students in Addis Ababa, Ethiopia. The prevalence of YFRHS among the study participant youths was found to be 11%. This level of prevalence was the lowest finding compared to a previous study conducted in Addis Ababa, Ethiopia, which indicated that 28.7% of study participated high school students reported to use YFRHS in the previous year of the survey [10]. Accordingly, the study conducted in Ambo revealed a prevalence of 20.7% [11], and more recently a much higher prevalence was also reported in a study conducted in Adama town [12]. The unusually lower prevalence of YFRHS reported in our study compared to the previous studies conducted in Ethiopia could be due to the effect of COVID-19 pandemic during our survey which might affect the study participants’ visit of service provides for RH services. The finding has shown a significant difference when compared to a community-based study, nearly 64% of Harare’s youth and nearly 69% of Mekele’s youth had used youth friendly services at least once at the time of the survey [13]. Due to the fact that this study was an institution-based study involving only preparatory school students, whereas the Harar and Mekelle study was a community-based survey involving a large sample size of youth.
The other possible reason to these discrepancies could be difference in cultural, methodology, sample size, time of study and participants in those areas. The odds of utilizing YFRHS were 2 times higher (AOR=2.531, 95% CI: 1.66, 4.37) among male participants as compared to females. Which is similar with previously conducted study in Addis Ababa [10]. Also, the study conducted in Hosanna, SNNPR, Ethiopia reported that male sex was more associated with increased uptake of RH service than female sex [14] which is consistent with the finding of Kenya where male participants utilized the service than females. This might be explained by the fact that fear of being seen while utilization of reproductive health services is more common among female students [15].
According to this study being in the age group of 17-18 were 0.18 times lower to use the RH service it could be significantly correlated with youths involved in reproductive health problem (ACR=0.187, 95% CI: 0.044,0.794). This was similar with the study conducted in ambo town, the age groups of 15 - 19 years were 0.38 times less likely to use youth friendly RH services than youth of age 20-24 years [AOR=0.380,95% CI=(0.176 - 0.819)] [10]. According to EDHS data a higher percentage of young women reported having sex before the age of 15 was 9%and before age18 was 40% also young men reported having sex before the age of 15 was 1% and before age18 was 12%. This early initiation of sexual activity with less utility of YFRHS could be an indicators for demographic factors such as high fertility rate and high mortality rate. Due to the fact this less utilization of YFRHS may exposure youths to high incidence of unwanted pregnancies, STI, unsafe abortion, pregnancies related complication, death, and begin childbearing at an even earlier age than indicated by the median age at first marriage.
This study found that governmental school student were 0.2 times lower to utilize YFRHS than the private school student. (AOR= 0.243, 95% CI: 0.141, 0.419). Which was negatively affect the students utilization of YFRHS. This discrepancy might be due to that private school student had better chance to get guidance and counseling service rather than the governmental school students. Students who’s living only with their mother were 0.06 times much lower to utilize RH service than other (AOR=0.061 95% CI: 0.008, 0.496) Also those study participant who had parental discussion on RH issue were 0.19 times lower to use YFRHS than their counterpart AOR=0.197,95% CI: (0.083,0464). This happened probably parental discussion on RH issue may help the student become abstained until their school ended which was good habit. The study participant’s source of information which was peer were 1.37 times higher to utilize YFRHS than other source of information (AOR=1.374, 95% CI: (0.822, 2.297). If this source of information supported by peer educators who was specially trained young student undertake informal or organized health education session in school with their peers those similar to themselves in age, background or interests aimed at developing young people’s knowledge, attitudes, beliefs and skills, it will help to enabling them to be more responsible for, and to, protect their own health In this study the knowledge of study participant toward RH service seems not well developed, about 82.3% was heard about YFRHS, But they were not utilized the provided service. This may imply student may suffer from lack of reproductive health education service. In most governmental school there were lack of YFRHS education. This assumption was supported by FGD participant.
Participants in the study who knew the STI symptom such as genital itching and genital ulcer were double times and four times much higher to use the RH service respectively, than those of who doesn’t knew STI symptom (AOR=4.211,95% CI: 2.486,7.131), (AOR=2.91,95% CI: 1.735,4.882). This could be the participant who had exposure to STI had a chance of getting treatments and education from health provider, therefore they may know STI better than other who didn’t have exposure. Among the study participant those who found YFRHS around there living area 60% of them were less utilized the service than those who had no youth friendly service in their living area (AOR= 0.4 95% CI: 0.235, 0.682). This finding was not similar with the study conduct in Ambo town study, those who had the services in their living area were 7 times more likely utilized YFRHS as compared to those who had no youth friendly service facility in their living area (AOR=7.1, 95% CI=2.676-19.015) [11]. According to this study the participant had less knowledge toward the YFRHS, this might affect the utilization of the YFRHS which was provided in their living area. Also, this respondent had negative attitudes toward YFRHS utilization which manifest on FGD section, this may lead them to not utilized the service. Such problem was elaborated with in FGD participant.
The study participant those who utilize YFRHS were two times got the working hour convenient to them than not utilize. (AOR=2.431 95% CI: 1.154, 5.121) This could be in Addis Ababa there are a lot of private health center which provided the service for 24 houres. According to the study participant student those who didn’t use YFRHS the respondent set different reason; out of this the majority respondents mention I don’t need the service accounts 476(68.5) which was similar with the study conducted in Ambo town those who did not use the service about 107(35.9%) of the respondents reported that the reason not to use YFRHS was because they do not want the services [11].
Conclusion
The prevalence of YFRHS in this study was 11% and this is relatively a much lower prevalence when compared with findings from previous studies. According to this study the main factors that affecting utilization of YFRHS was the study participants altitude which was negative toward the importance of YFRHS it was manifested through FGD. The government and other non-organization try to develop strategies to improve youth RH need but the existing RH service was not fulfilling the expected out come due to low promotion of YFRHS, fail to provide the service in school, lack of privacy and confidentiality to in-school service, resulting poor RH service utilization among young students. The current police limited to provide the service only in health facility but it should must implement in school setup.
Promoting youth-friendly programs is critical in assisting young people in making informed reproductive health choices and encouraging them to follow through with those decisions, therefor the stakeholder should expand this promotion to the lower level such as in school. From this finding we can judge youth are exposing to many RH risky, therefor the governmental, non- governmental body should give their attention towards youth reproductive health unless the effects were not simple as it seems it had national even world wild effect, due to demographical and public health accept this was serious agenda. YFRHS can address this situation by improving the availability, acceptability, accessibility, and equity of health services for young people in their school.
Recommendations
According to the study result different responsible part should take some action such as:
The parent should be aware of about their children need and they should participate in YFRHS provision
Each school should work on their student by collaboration with each werda health office
Health centers should not exclusive their service only in health station, they should form a chain in different school
YFRHS, MOH, MOE and Secretary General for Women, Children, and Adolescents affairs should be work together on policy making and implementation
Initiate researcher to study further on the hidden issue of adolescents and youth reproductive health.
Declarations
I hereby declare that this MSc proposal on youth friendly reproductive health service utilization and associated factors among preparatory school students is my original work and all sources of material used for this thesis have been duly acknowledged.
Acknowledgements: I would like to thank the almighty GOD for his mercy and his love, also I appreciate the center of Population Studies, College of Developmental Studies of Addis Ababa University for giving the chance to do this research proposal also I would like to express my deepest gratitude and thanks to my advisor Dr Wondimye A. (PhD) for his unreserved advice, comment, support with help full educational materials and provision of timely and valuable advice for the accomplishment of this research.
References
- United Nations Population Fund East and Southern Africa & International Planned Parenthood Federation Africa Region. Assessment of Adolescents and Youth-Friendly Health Service Delivery in the East and Southern Africa Region. Johannesburg and Nairobi, UNFPA, United Nations Population Fund and IPPF, International Planned Parenthood Federation. 2018.
- United Nations, Department of Economic and Social Affairs, Population Division. (www.Worldometers.info).
- Mental Health Disorder EPHA 28th conference. 2016.
- Magdy K, Training Manual for the Providers of Youth-Friendly Services. www.fhi360.org. 2011.
- Natnael Atnafu. Youth friendly service utilization and associated factors among preparatory school students in sodo town, southern nations, nationalities and people’s region, Ethiopia. 2017.
- World Health Organization Department of Reproductive Health and Research: Global consultation on lessons from sexual and reproductive health programming to catalyze HIV prevention for adolescent girls and young women, Brocher foundation, Hermance, Geneva, Switzerland. 2016; 27-29.
- Pathfinder international, Bringing Youth-Friendly Services to Scale in Ethiopia. 2012. WWW.PATHFINDER.ORG.
- Erulkar, Annabel, Abebaw Ferede, Worku Ambelu, Woldemariam Girma, et al, Ayehualem Tameru, and Messay Teferi. Ethiopia young adult survey: A study in seven regions. Addis Ababa: Population Council. 2016.
- Simegn A, Azale T, Addis A Youth friendly sexual and reproductive health service utilization among high and preparatory school students in Debre Tabor town. 2020.
- Tefera T. Assessment of reproductive health service utilization and associated factors among high school youths in Addis Ababa, Ethiopia. Master’s Thesis, Addis Ababa University. 2015.
- Amerti Fikadu, Elias Teferi, Mulugeta Mekuria, Adamu Birhanu, Tsegaye Benti. Youth Friendly Reproductive Health Service Utilization and Associated Factors among School Youths in Ambo Town, Oromia Regional State, Ethiopia. 2018.
- Abenet Menene Gurara, Admasu Belay Gizaw, Awoke Koyachew Ayalew. Aliye Kediro Adem Reproductive health service utilization and associated factors among adolescents at public school in Adama town east Shewa Ethiopia. 2020.
- Kalayu Kahsay, Semarya Berhe, Mussie Alemayehu utilization of youth friendly services and associated factors in mekelle town, tigray, northern Ethiopia. 2016.
- Tsegaab Temesgen, current utilization of reproductive health Services and the role of peer influence among Undergraduate students of wachamo University, hosanna, SNNPR, Ethiopia. 2017.
- Perez O. determinants of utilization of youth friendly reproductive health services among school and college youth in thika west district, kiambu county, Kenya. Master’s Thesis. Kenyatta University. 2012: 27-44. OD25.