
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Research Article - Open Access, Volume 6
Should carotid body tumors be embolized pre-surgically?: A single university hospital randomized study
Mohammad Ali Nahas1*; Ashraf Mohammed2; Ammar Mohammad2; Bashar Al-Ajjan2; Joudy Elerdy3; Issa Ahmad3; Jaafar Samrah3; Mohamad Ghannam2; Mohamad Ali Ahmad2; Zaher Al Nahhas4
1Head of Division of Vascular and Endovascular Surgery, National University Hospital, Faculty of Medicine, University of Damascus, Syria.
2Vascular Surgeon, National University Hospital, Faculty of Medicine, University of Damascus, Syria.
3Vascular Surgery Resident, Damascus University Hospitals, Faculty of Medicine, University of Damascus, Syria.
4Resident, Department of Radiology, Damascus Hospital, Damascus, Syria.
*Corresponding Author : Mohamad Ali Nahas
Head of Division of Vascular and Endovascular Surgery, National University Hospital, Faculty of Medicine, University of Damascus, Syria.
Email: ali.nahas@damascusuniversity.edu.sy
Received : Jan 29, 2025
Accepted : Feb 20, 2025
Published : Feb 27, 2025
Archived : www.jcimcr.org
Copyright : © Nahas MA (2025).
Abstract
Objective: Carotid body tumors, almost benign, are some of the most challenging cases for Vascular surgeons, because of their close proximity to the neuro-vascular structures of the neck and their hyper-vascularized histological nature. Complete surgical resection is the cornerstone of treatment of these tumors. This study aims to evaluate the role of pre-surgical embolization in the reduction of para-surgical complications of carotid body tumors resection.
Methodology: Between 2010 and 2023, 29 carotid body tumors in 24 patients underwent surgical resection in our center, of which 13 tumors were embolized pre- surgically. Statistical analysis of the differences in para-surgical bleeding, neurological injuries and duration of surgery between the embolized and non-embolized patients was then done.
Results: Statistical analysis showed that the pre-surgical embolization contributed to reduction of para-surgical bleeding and shortening time of surgery, whereas there were no statistically relevant differences regarding the neurological injuries between the two groups which depend, mainly, on the operator experience and classification of the tumor.
Conclusion: When performed by well experienced hands, pre-surgical embolization can reduce para-surgical morbidity and mortality of carotid body tumors resections. It is useful to include the results of this study in meta-analysis and systematic reviews to get results that are more generalizable.
Keywords: Vascular surgery; Carotid body tumors; CBTs; Embolization.
Citation: Nahas MA, Mohammed A, Mohammad A, Al-Ajjan B, Elerdy J, et al. Should carotid body tumors be embolized pre-surgically?: A single university hospital randomized Study. J Clin Images Med Case Rep. 2025; 6(2): 3488.
Introduction
Carotid Body Tumors (CBTs), also known as carotid chemodecatomas, paraganglioams, are rare neoplasms with a very little number of cases described in the literature. These tumors belong to the bigger “paraganglioma” tumor family, which is a family of tumors that originates from the neural crest cells in the whole body [1].
The “carotid body” is the largest mass of chemoreceptor in the body. It is located in the posterior-lateral wall of the carotid sinus within the peri-adventitial tissue and measures about 0.5 cm. It receives arterial supply from branches of the external carotid artery, whereas the venous drainage is carried out through tributaries of the lingual and laryngeo-pharyngeal veins.
Embryonically, the carotid body origins from the third brachial arch, namely from its neuroral crest ectoderm and mesodermal tissue. These neural crest cells immigrate in association with the autonomic ganglion cells and called the type 1 glomus cells, while the mesodermal tissue forms the vascular-rich stroma [2].
These chemoreceptors are stimulated by hypoxia, hypercapnia and acidosis. Stimulating the glomus cell type 1 releases neurotransmitters leading to increase in the respiratory rate and tidal volume, additionally, they cause hypertension as a result of vasoconstriction [3].
Carotid body tumors resemble the normal carotid body both macroscopically and microscopically [4]. They are usually benign neoplasm with a slow growth. In contrast to many other neoplasms of the body, the malignancy of CBTs is determined by clinical behavior rather than histology. The malignant transformation is generally rare [5].
The most common presentation of carotid bod tumors is asymptomatic neck mass below the angle of the mandible, which are usually smooth, lobulated and firm. The most characteristic sign is the horizontal mobility of the vertically fixed mass on clinical examination [6]. Large tumors may cause nonspecific symptoms related to local compression and\or invasion such as tenderness, fullness, numbness, hoarseness, dysphagia and chronic cough. Due to compression, there might be in rare cases signs of compression of 10th, 11th and 12th cranial nerves. Horner’s syndrome is occasionally described in these tumors). In 30-40% there is an auditable bruit over the mass [7,8].
| There is a wide-range differential diagnosis of carotid body tumors, these can be classified based on etiology as the following: Congenital | Congenital malformation, hygromas. Branchial cleft cysts |
|---|---|
| Inflammatory | Reactive lymph adenopathy, chronic lymphadenitis |
| Infections | Viral, bacterial and parasitic |
| Benign tumors | Lipoma, salivary glands, other cervical gangliomas ((glomus jugulare and glomus vagale) |
| neoplastic | Metastatic, lymphoma |
| carotid | Aneurysms, kinks |
Because of this wide range of differential diagnosis, radiological imaging plays an essential role in the evaluation of neck masses [9]. Both Computed tomography angiography CTA and Magnetic resonance Angiography MRA have replaced the Digital subtraction Arteriography as the imaging modality of choice, unless pre-surgical embolization is indicated, these two modalities are non-invasive and provide excellent anatomical and vascular details when duplex ultrasound is insufficient, especially regarding the proximal and distal parts of the tumor [7].
Duplex ultrasound is a safe option, which can provide details about the size, vascularity, vascular encasement and eventual carotid artery atherosclerotic disease. However, this modality is operator dependent, and might be unable to clearly visualize the proximal and distal extension of the tumor [7].
Conventional digital subtraction arteriography was previously the gold standard for the diagnosis of carotid body tumors. It can clearly visualize the size, extent and vascularity of carotid body tumors. Additionally, it provides the opportunity of pre-surgical embolization of the tumor, which seems to play a prophylactic role against complications. On the other hand, DSA is invasive, which can cause hematomas, common femoral artery pseudoaneurysms, dissections and contrast material related complications [10].
Shamblin et al. have set a classification for CBTs, which classifies the tumor size and its adjacent carotid arteries involvement in three tumor groups as the following:
| Group 1 | Small tumors that can usually easily dissected. |
| Group 2 | tumors that partially encases the carotid arteries |
| Group 3 | tumors that completely encases the carotid arteries |
This classification can assist the treatment planning and the prediction of the complications [4].
Prompt surgical resection is the cornerstone of the treatment of carotid body tumors, in the absence of perioperative risk, prohibitive co-morbidities or short life expectancy. CBT patients should undergo surgical resection as soon as the diagnosis is made in order to avoid invasion of nerves, malignant transformation and cranial extension [11].
Pre-operative embolization through selective catheterization of the blood feeding vessels is a controversial option; some studies demonstrated lower blood loss, shorter surgery time, shorter hospital stays and lower perioperative complication. However, other studies mentioned disadvantages including the invasive nature of embolization, the possible inadvertent cerebral embolization and higher costs [10,12]. We support the routine embolization of shambline 2 and 3 tumors using particle and in very selected case coils after selective catheterization of the external carotid artery and the tumor feeding vessels.
Radiation therapy is reserved for unresectable, recurrent CBTs or patients who are deemed poor surgical candidates. Preoperative radiation should not be performed to avoid extensive scarring which might negatively affect the surgical planning [12].
Surgical resection is usually carried out under general anesthesia through a longitidual incision along the median border of the sternal-cleido-mastoid muscle. The tumor is then carefully dissected from the surrounding tissues. It is of utmost importance to recognize and protect the cranial 10th, 12th and sometimes 9th nerves. The tumor is usually dissected starting from the peri- adventitial tissue of the medial aspect of the tumor near the external carotid artery. It might be necessary to ligate the encased external carotid artery and resect it enbloc with the tumor. The internal carotid artery must be protected as much as possible. When it is necessary, the internal carotid artery and the carotid bifurcation can be resected with tumor and reconstructed using either 6-mm ePTFE or saphenous venous interposition graft. Using a vascular shunt in this case might be recommended.

The surgical mortality, reported by literature, is less than 0, 5% [13]. Complications rate is believed to be very rare occurrence including cerebrovascular, cranial nerve and other minor complications when performed by well-experienced surgeons. Other relevant complications include bleeding and neck hematomas. The tumor volume and its proximity to the base of the skull are the most important predictors of post-surgical complications, while the majority of authors depend on the shamblin’s classification [13].
Objectives
A case series study aims to:
- Represent the diagnosis, treatment options, surgical results and complication in our center retrospectively.
- Test the statistical relevance of the differences between surgical resection of CBTs with and without pre-surgical embolization.
Methodology
The patients’ medical records were revised. Relevant data regarding pre-surgical assessment, surgical intervention and post-surgical follow up were collected. The post-surgical complication rate, surgical time, intra-surgical bleeding was compared between the pre-surgical embolization group and the direct surgical resection group. The statistical relevance of the differences between the two groups were then checked.
Results
24 patients with 29 neck masses (19 unilateral and 5 bilateral cases) were referred to our vascular surgery university clinic over 13 years period (2010-2023), 11 females (45.83%) and 13 males (54.16%), aged: 20-71 years old. The family history was positive in 5 patients (20.83%).
The most common symptom was an accidentally discovered asymptomatic neck mass in 11 cases (37.93%), other symptoms included: dysphagia in 6 cases (25.00%), hoarseness in 5 cases (17.24%), dyspnea in 4 cases (13.79%), headaches in 2 cases (6.89%) and vertigo in 3 cases (10.34%). Relevant medical history included 1 case of arterial hypertension and palpitation in another single case, the endocrinology works up, which was done by the endocrinologists, was negative in the both cases. Additionally, two patients underwent previously lymphnodes resections in external clinics before referral to our clinic, the pathology revealed non-specific inflammatory changes in both cases.
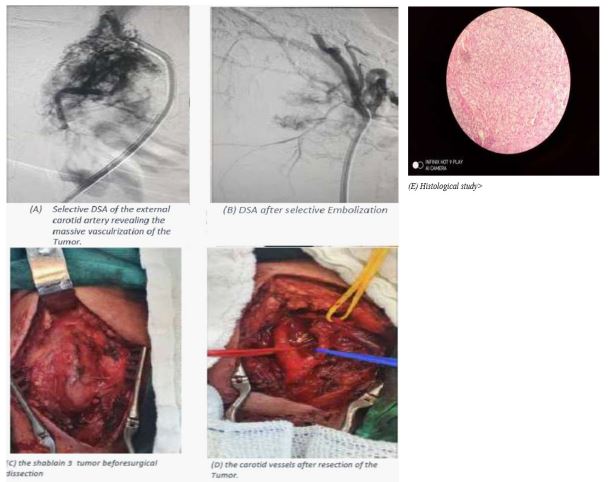
Radiologic assessment included color duplex ultrasonography and contrast multi-slice computed tomography for all cases to confirm the diagnosis of CBT. DSA was carried out in 13 cases, who subsequently underwent pre-surgical embolization. Tumor size ranged between (21-72 mm) on its maximal diameter, with an average tumor size of 3.16 mm. While the Shamblin’s class was class 1 in 2 tumors (6.89%), class 2 in 25 tumors (86.20%), and class 3 in 2 tumors (6.89%). 13 cases out of 29 underwent pre-surgical embolization using (750-1000 micrometer) particles injected through selective catheterization of the tumor feeding vessels and in one patient pushable coils were used because of the great size of the feeding artery originating from the superior thyroid artery.
The surgical approach was through a longitudinal incision along the medial border of the sternocleidomastoid muscle followed by proximal common carotid control far from the tumor, after that a delicate dissection of the external carotid artery and, when possible, of the XII nerve. The dissection of the tumor was hold from the external carotid artery first and then laterally toward the internal carotid dissecting the tumor away from it. Ligation of the external carotid artery in 2 cases (6.89%). In tow case (6.89%) the internal carotid artery was intersected and a saphenous interposition graft was performed. tumor resection was feasible in 28 cases, while in one case the tumor was not totally respectable due to its close proximity to the base of the skull. Radiotherapy was recommended later.
The duration of surgery varied between 40-180 minutes. The median duration was shorter in embolized cases (75 vs 120 minutes). The intra-surgical bleeding was less than 100 ml in all embolized tumors, while in the non-embolized cases the Median intra-surgical bleeding volume was approximately 750 ml (75-3000 ml).
Reoperation was needed in one patient (3.44%) due to a retro bulbar bleeding. Post-operative neurologic defects occurred as following:
2 post-surgical transit cranial nerve injuries (facial and sublingual. Which totally resolved spontaneously, brain imaging revealed no specific findings (1 embolized and 1 non- embolized case.
| Group | Embolization | Surgery |
|---|---|---|
| Mean | 58.85 | 757.81 |
| SD | 21.13 | 746.31 |
| SEN | 5.86 | 186.58 |
| N | 13 | 16 |
| The two-tailed P value equals 0.0023. By conventional criteria, this difference is considered to be very statistically significant. (CI=95%, t=3.3641, df=27, standard error of dif- ference = 207.773). | ||
In one case the vagus nerve was encased by the tumor and injured during dissection, the symptoms were well tolerated, this case was not previously embolized.
| Group | Embolization | Surgery | |
|---|---|---|---|
| Complicated | 1 | 2 | 3 |
| Non-complicated | 12 | 14 | 26 |
| Sum | 13 | 16 | 29 |
| The chi-square statistic is 0.1787. The p-value is .672452. The result is not significant at p<.05. | |||
There was no para-surgical mortality. no cases of recurrence during the follow up period (1-13 years).
| Group | Embolization | Surgery |
|---|---|---|
| Mean | 74.23 | 129.88 |
| SD | 17.64 | 29.68 |
| SEN | 4.89 | 7.42 |
| N | 13 | 16 |
| The two-tailed P value is less than 0.0001 By conventional criteria, this difference is considered to be extremely statistically significant. (CI=95%, t=5.9491, df=27, standard error of difference=9.353). | ||
The results were then statistically analyzed, regarding the bleeding differences between embolized and non-embolized patients using T-test, the results were as following:
Another variable was the incidence of cranial vascular nerve injuries using the chi-square test, the results was as following:
The duration of surgery of these two groups was also compared in minutes, the results was as following:
Based on the statistical analysis of the results, the pre-surgical Embolization lead to significant reduction in the surgical time and intra-surgical bleeding. No statistically significant difference in the incidences of cranial nerve injuries.
Discussion
Carotid body tumors are benign neoplasms that arise in the neck. Malignancy is rare and the malignant transformation is diagnosed upon the clinical behavior rather than pathological findings. Despite the benign nature of these tumors, their surgical resection can cause life-threatening complications due to its close proximity to the respiratory tract, cranial nerves and the carotid artery. One case of a carotid body tumor in our center was non-operable at the time of diagnosis. The tumor was then embolized and transferred to radiation therapy. The patient was excluded from the study because was lost of the follow up.
The distribution of the cases revealed a slight male-predominance. The age distribution was revealed a wide age distribution (20-71 years), these results are with the epidemiological studies, which show that these tumors can be detected at any age. The somehow high age at the time of diagnosis among some patients can be understood on the light of the general situation in Syria, namely the under-functioning health services and the lack of health insurance policy, which should cover all people equally.
Our center covers the vast majority of CBTs surgeries in Syria; therefor this study can give an idea about the prevalence of this disease in Syria. However, the asymptomatic nature and the restricted accessibility to the healthcare system for many patients can mask the exact prevalence of these tumors.
5 of 24 patients (20.83%) presented with bilateral tumors, 3 of these patients were 1st degree relatives, what can indicate the genetic tendency of these tumors. This familiar CBTs makes up to 10% of cases and is usually inherited in autosomal dominant model. However, further genetic workup is necessary to confirm this tendency. Many patients in our study lives in mountainous areas, which is a well-known risk factor for carotid body tumors due to chronic hypoxemia.
The age range was somehow wide (20-71) years. Early diagnosis was related mainly to symptomatic cases and family members screening, therefor it seems useful to perform screening using duplex ultrasonography for first degree relatives of the patients.
The decision to perform pre-surgical embolization depended on tumor size and surgeon’s preferences. Financial aspects played also a role on the light of the missing well established health insurance system.
The duration of surgery among patients who underwent pre-surgical embolization was clearly shorter. There are many factors which could clarify this fact, such as the minimal bleeding, which leads to a clear surgical field, easier dissection and reduced stress. However, these benefits might be challenged by the time needed for the embolization, the side effects of the contrast media and the use of ionizing X-rays.
The most important benefit of pre-surgical embolization of carotid body tumors is the reduction of blood loss, which in turn contributes to the reduction of transfusion therapy, which can help in the avoidance of transfusion’s complications, including acidosis, hypothermia and respiratory complications.
Another important aspect of post-surgical complications of carotid body tumors resection are the nerve injuries. These surgeries are usually performed in a very narrow area, which serves as a pathway for many nerves (7th, 9th, 10th and 12th cranial nerves). The nerve injuries can lead to disability, cosmetic issues and in some cases life-threatening complications. The use of pre- surgical embolization can theoretically minimize the risk of cranial nerves injuries. Our study didn’t show a fundamental drop in nerve injuries after using the embolization. The main reason of these results is the direct encasement of the nerves by the tumor in addition of the small number of cases, which could mathematically mask any statistical relevance of the deference’s between the two patients’ groups.
The Shamblin’s classification is a useful tool to expect post-surgical complications. However, this classification neglects many other important prognostic factors, such as the tumor size, nerve encasement and anatomical characteristics of the patient. It might be beneficial to develop a scoring system, which considers all prognostic aspects, such a system should consider the size and other characteristics of the tumors feeding vessels, in order to simplify the decision, to embolize the tumor.
The surgical skills and experience are also important factors in the decision-making process, as the embolization process itself can end in devastating sequences, when performed by surgeons or interventional radiologists who lack sufficient endovascular skills. Affinity to embolization procedures is also very important. Embolization process should be done selectively with utmost care, to avoid injuries such as carotid dissection and accidental embolization of the internal carotid artery.
Conclusion
Pre-surgical embolization has a protective role against para-surgical complications of carotid body tumors resection, as long as it contributes of reduction in surgical bleeding, duration of surgery and nerve injuries. However, it is of utmost importance to perform the embolization by well-experienced surgeons or interventional radiologists who have a good affinity with embolization’s techniques. It seems reasonable to include the results of this study in systematic reviews and/or meta-analysis in order to generalize the results.
References
- Sevilla Garcia MA, Llorente Pendas JL, Rodrigo Tapia JP, et al. Head and neck paragangliomas: revision of 89 cases in 73 patients. Acta Otorrinolaringol Esp. 2007; 58: 94–100.
- Baysal BE, Myers EN. Etiopathogenesis and clinical presentation of carotid body tumors. Microsc Res Tech. 2002; 59: 256–261.
- Kumar P, Prabhakar NR. Peripheral chemoreceptors: function and plasticity of the carotid body.
- Compr Physiol. 2012; 2: 141–219.
- Shamblin WR, ReMine WH, Sheps SG, et al. Carotid body tumor (chemodectoma). Clinicopathologic analysis of ninety cases. Am J Surg. 1971; 122: 732-739.
- Rinaldo A, Myssiorek D, Devaney KO, et al. Which paragangliomas of the head and neck have a higher rate of malignancy?. Oral Oncol. 2004; 40: 458–460.
- Westerband A, Hunter GC, Cintora I, et al. Current trends in the detection and management of carotid body tumors. J Vasc Surg. 1998; 28: 84-93.
- Amin MF, El Ameen NF. Diagnostic efficiency of multidetector computed tomography versus magnetic resonance imaging in differentiation of head and neck paragangliomas from other mimicking vascular lesions: comparison with histopathologic examination. Eur Arch Otorhinolaryngol. 2013; 270: 1045–1053.
- Stoeckli SJ, Schuknecht B, Alkadhi H, et al. Evaluation of paragangliomas presenting as a cervical mass on color-coded Doppler sonography. Laryngoscope. 2002; 112: 143–146.
- Schwetschenau E, Kelly DJ. The Adult neck mass. Am Fam Physician. 2002; 66: 831-8.
- Kafie FE, Freischlag JA. Carotid body tumors: the role of preoperative embolization. Ann Vasc Surg. 2001; 15: 237–242.
- Hinerman RW, Amdur RJ, Morris CG, et al. Definitive radiotherapy in the management of paragangliomas arising in the head and neck: a 35-year experience. Head Neck. 2008; 30: 1431–1438.
- Power AH, Bower TC, Kasperbauer J, et al. Impact of preoperative embolization on outcomes of carotid body tumor resections. J Vasc Surg. 2012; 56: 979–989.
- Kim GY, Lawrence PF, Moridzadeh RS, et al. New predictors of complications in carotid body tumor resection. J Vasc Surg. 2017; 65: 1673–1679.