
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 6
The use of acoustic myography and multi-frequency bioimpedance to assess muscle function and rehabilitation following ACIF: A case study
Bartels EM1; Harrison AP2
1Department of Neurology, Copenhagen University Hospital, Bispebjerg and Frederiksberg, Denmark.
2Department for Veterinary and Animal Sciences (IVH), Section for Physiology, Faculty of Health & Medical Sciences, University of Copenhagen, PAS, Dyrlægevej 100, 1870 Frederiksberg C, Denmark.
*Corresponding Author : Harrison Adrian Paul
Department for Veterinary and Animal Sciences
(IVH), Section for Physiology, Faculty of Health &
Medical Sciences, University of Copenhagen, PAS,
Dyrlægevej 100, 1870 Frederiksberg C, Denmark.
Email: [email protected]
Received : Feb 08, 2025
Accepted : Mar 05, 2025
Published : Mar 12, 2025
Archived : www.jcimcr.org
Copyright : © Harrison AP (2025).
Abstract
The aim of this case study was to see if multi frequency Bioimpedance and Acoustic Myography, both non-invasive and easily applicable methods, could be used to follow patients with nerve injuries during the long healing process following surgery. A patient suffering from a prolapse at the level of C5-6 on the right side with paresis in the upper right extremity over the shoulder and elbow was followed for a period of 12 months after surgery using the Anterior Cervical Interbody Fusion (ACIF) technique. To avoid a high degree of muscle atrophy during nerve recovery, the affected m. Biceps was electrically stimulated using a TENS unit on a daily basis. The two applied measuring techniques showed great promise as a package to design physiotherapy correctly so that it matches the patients needs, as well as follow recovery both prior to any physical sign of improvement and during visible improvement, including signs of overtraining by the patient.
Keywords: Case report; Disc prolapse; ACIF; Rehabilitation; Acoustic myography; Multi-frequency bioimpedance.
Citation: Bartels EM, Harrison AP. The use of acoustic myography and multi-frequency bioimpedance to assess muscle function and rehabilitation following ACIF: A case study. J Clin Images Med Case Rep. 2025; 6(3): 3506.
Introduction
This case report is the first of its kind to demonstrate feedback concerning muscle function in a prolapse paresis subject following ACIF. It reveals the importance of being able to provide the patient with encouraging progress, especially during the first 6-8 months following surgery, where training is essential for successful rehabilitation. During this time patients most often lack any feeling of functional improvement themselves and are therefore likely not to adhere to their rehabilitation programme.
Case history
A 68 year old male patient presented himself with paresis in the upper right extremity over the shoulder and elbow, complaining of pain and sensory disturbances. An MRI showed a prolapse at the level of C5-6 on the right side. C4-5 also revealed significant changes. The condition was treated with decompression and insertion of a cervical cage in both of the mentioned positions, applying the Anterior Cervical Interbody Fusion (ACIF) technique. Following the operation there was an improvement in radiculopathy after a period of three days and the patient was dismissed from hospital. He was subsequently referred for rehabilitation training at the city council clinic. The expectation of the neurosurgeon was that improvement back to normal use of the right arm would take up to two years, and that the outcome may not be a complete recovery.
During the first month following the operation, an adequate level of rehabilitation was not forthcoming. Subsequently, the decision was made to follow this patient as an individual case study. The aim was to see if it was possible to document the effect of rehabilitation, and especially to identify clear signs of improvement in terms of muscle activity in the affected arm. One of the major concerns was that the muscle (m. Biceps brachii) that had impaired nerve stimulation would continue to deteriorate without some form of intervention, making long-term recovery and full use of the right arm difficult as a consequence (e.g. atrophy) [1,2]. Furthermore, it has recently been shown that muscle contraction plays an essential role in stimulating new growth of motor neurons involving both biochemical and mechanical factors [3]. The solution for this concern was to provide the patient with a TENS stimulator (InTENSity 12; Roscoe Medical Inc. Ohio, USA) in order to deliver field stimulation of m. Biceps. The patient was educated in the use of the TENS device which had been pre-set to P1 (20 mins treatment time, pulse rate 1-10 Hz, pulse width 150-200 microseconds, cycle time 20 sec) and P2 (20 mins treatment time, pulse rate 80-100 Hz, pulse width 100-120 microseconds, cycle time 10 sec). The device was used twice daily on the affected arm only. The patient complied closely with this stimulation protocol, which he was instructed in the use of and followed rigidly. The decision to stimulate was made in order to maintain as much healthy muscle tissue as possible during the initial phase of recovery, when there was little or no nerve stimulation of the involved muscle of the right upper extremity. Compliance and tolerance were discussed with the patient at the start of each new mfBIA and AMG measurement, and no adverse or unanticipated events occurred over the year. Prior to the start of rehabilitation (after the first month following the operation), multi frequency Bioimpedance (mfBIA) and Acoustic Myography (AMG) measurements were carried out on m. Biceps on both upper extremities. These measurements were then repeated on the affected arm at approx. monthly intervals, so as to follow any detectable improvement.
At the first follow-up control visit with the neurosurgeon (approx. 3 months following surgery), the rehabilitation programme provided by the local city council was discussed. The outcome of this control visit was that the patient was sent to a specialized physiotherapist who dealt routinely with neurological cases. A training programme was subsequently designed to meet the patient’s special needs and expectations. The patient followed this training programme closely at home.
Measuring methods
Two non-invasive and easily applicable methods were used, namely mfBIA and AMG. Full ethical approval for the use of these two techniques was gained from Copenhagen University Department of Pathobiological Sciences, Faculty of Health & Medical Sciences (protocol ID 2018-15-0201-01462). The choice of combining these two measuring techniques was due to a wish to obtain a full description of the recovery processes taking place at rest and during movement. It should be noted that mfBIA lends itself to static measurements, whilst AMG records dynamic activity in muscle. Our aim was to follow the rehabilitation process in the right arm starting from a stage with little or no stimulation from the damaged nerve, to one of almost complete recovery. mfBIA gives a description of the condition of the involved muscle [4], in this case the m. Biceps brachii. The parameters measured were impedance Z, resistance R, reactance Xc, phase angle PA, centre frequency fc, membrane capacitance Mc, internal resistance Ri, and external resistance Re. A full set of values for these parameters in a healthy population can be found in Bartels et al. [5]. AMG measures the number and type of muscle fibres involved in producing a defined force/movement, and the ability to switch off these fibres when they are not needed. This is described by the parameters S (spatial summation – how many fibres operate at a given time), T (temporal summation – how often a fibre is triggered over a given time period) and E (efficiency – the period of time that muscle fibres are contracted during any given movement) [6,7].
Results
mfBIA
The results for the mfBIA measurements showed an overall level of significance for m.Biceps for Z, R, PA, fc, Mc and Ri compared with values for the healthy arm (left). The results for PA (ratio of R and Xc) showed an initial set of values that were very close to those of the healthy arm, before worsening and then over time showing an improvement close to that of the healthy arm (P=0.002). The results for Xc showed an initial set of values that was very high compared to those of the healthy arm, before worsening slightly and then over time reversing to become identical with that of the healthy arm (P=0.8). The results for R and Z showed an initial set of values that were very high compared to those of the healthy arm, before settling around and slightly above values for the healthy arm (both P=0.03). The results for fc showed an initial set of values that was very comparable to those of the healthy arm, before increasing over time and remaining elevated compared to the healthy arm (P=0.0006).
The results for Re showed an initial set of values that was very high compared to those of the healthy arm, before settling around values for the healthy arm (NS). The results for Mc and Ri showed an initial change that was very different to those of the healthy arm, before fluctuating with values that were very different from the healthy arm (P< 0.0001 and 0.004, respectively).
AMG
AMG recordings were made from m. Biceps during voluntary movements, where the patient was asked to rotate his forearm slowly and as fast as possible, whilst supporting his forearm on a table. The rotation took the form of a diadochokinesia with the forearm flat on the table, such that m. Biceps was activated but did not take part in the counter gravitational effort of supporting the affected arm. The progression of the AMG S- parameter shown as Volts over time for the patient during the postoperative period is shown in Figure 2.
Compared with the healthy left arm, the T-score for fast voluntary movements, mainly involving fast fibres, was found to change very little. For the slow voluntary movement, mainly involving slow fibres, the T-score was found to decrease (faster firing frequency) compared with the healthy left arm, before finally recovering completely (Figure 3). Of interest are the changes in frequency, since the T-score was measured with a 160 Hz setting, the value of 8.8 for the healthy slow arm movement represents a firing frequency of 19.2 Hz, whilst for the healthy fast arm movement a value of 9.3 represents a firing frequency of 11.2 Hz. During the rehabilitation period the lowest T-score for the fast arm movement was 6.5 representing a firing frequency of 56.0 Hz, and for the slow arm movement a low value of 4.7 was measured, representing a firing frequency of 84.8 Hz.
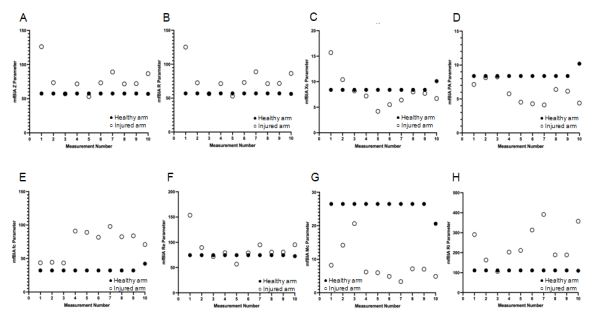
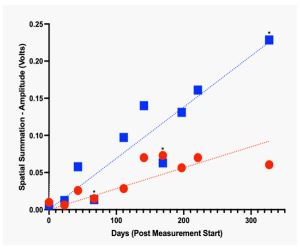
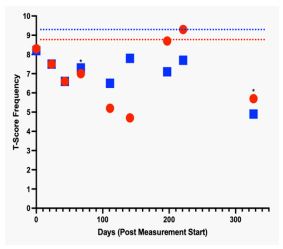
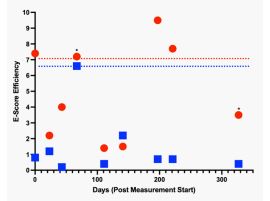
Table 1: The eight mfBIA parameters measured for the healthy arm at the start and finish of the study, as well as the start and finish parameters for the injured arm (m.Biceps). Values were measured at the 50 kHz setting.
| Z (Ω) | R (Ω) | Xc (Ω) | PA (o) | Fc (kHz) | Re (Ω) | Mc (nF) | Ri (Ω) | |
|---|---|---|---|---|---|---|---|---|
| Healthy arm (18th Dec 2023) | 57.6 | 57.0 | 8.4 | 8.4 | 32.2 | 74.7 | 26.5 | 111.3 |
| Healthy arm (25th Nov 2024) | 57.1 | 56.3 | 10.1 | 10.2 | 42.3 | 72.6 | 20.6 | 109.6 |
| Injured arm (18th Dec 2023) | 126.2 | 125.2 | 15.7 | 7.1 | 43.6 | 153.6 | 8.2 | 290.8 |
| Injured arm * (25th Nov2024) | 86.7 | 86.4 | 6.7 | 4.4 | 70.9 | 95.1 | 4.9 | 357.3 |
* denotes that this recording was taken a day after over-training.
In the affected arm, the E-score for fast voluntary movements is very much decreased and remains so throughout the rehabilitation period. This indicates that the fibres associated with fast movement are not being efficiently used and are most likely active for most of the time. The slow arm movement Escores show a higher value than those for the fast arm movement during most of the rehabilitation period and appear to return to normal or better values at or around 200 days. Note that overtraining (day 67) has probably tired out both fast and slow fibres such that a false efficiency score is measured following a bout of over exercise, due to the fact that very few fibres are active at all (see Figure 2).
12 month follow-up
Approximately 12 months after the initial assessment measurements applying mfBIA and AMG, a follow-up measurement was made
mfBIA: For a comparison of the changes in mfBIA parameters for this patient and for the injured as well as the control healthy limb see Table 1. The healthy limb had maintained almost every parameter, apart from PA which had improved. This change is in line with a very physically active patient who had compensated by using the healthy arm for every task required in daily life. The injured arm showed signs of over-exercise (high Ri and lower Mc), but otherwise great improvement. The Z and R parameters were closer to those for the healthy arm and the Re value was greatly reduced, indicating less oedema, which in itself would improve the Z and R values.
AMG: In the healthy control limb, fast and slow rotation gave an S-score of 6.20 and 8.10 at the start of voluntary diadochokinesis (18th Dec 2023) corresponding to a signal amplitude of 0.0467 and 0.0234 Volts, respectively. These values were retained throughout for the healthy limb. Approximately 12 months after the initial assessment, the signal amplitude for the injured arm also gave comparable amplitude values of 0.0403 and 0.0269 Volts for the fast and slow voluntary diadochokinesis, respectively. The AMG (S-score) amplitude values for P1, recorded 12 months after the initial assessment, were found to be 0.0269 and 0.0269 Volts for the injured limb at the start and 20 minutes after TENS stimulation. For P2, however, S-score amplitude values of 0.0403 and 0.0148 Volts were recorded at the start and after 20 minutes of TENS stimulation, respectively. Combined, these results indicate that whilst slow stimulation (P1) was sustainable by the injured muscle, the faster stimulation (P2) resulted in fatigue, even though the starting value was identical to that of the healthy limb.
Feedback from the patient: The patient reported that he was now functionally recovered to the extent that he could easily lift a 1 kg weight and was able to carry out daily living tasks including washing his hair, buttoning up shirts, cooking and light gardening activities. He also added that he would not have been motivated to complete the training of his injured arm without the feedback offered using mfBIA and AMG measurements, where improvement was detectable much earlier than anything he could feel himself.
Discussion/conclusion
The aim of this case study was to find a method to follow improvement of nerve damage during the period of recovery, following an ACIF intervention. Such a recovery period is known to be long and not easy to comprehend for the patient. Furthermore, the recovery period is also important for the medical and therapeutical staff treating the patient since further intervention may be necessary depending on the progress and outcome of the patient over time.
This case report is limited to the fact that only one subject has been measured, the degree of nerve damage was severe but hard to quantify (the patient could not lift his right arm at all at the start). Moreover, the potential effects/benefits of TENS stimulation cannot be assessed with only one subject. However, the patient adhered closely to the TENS stimulation programme as well as additional training/rehabilitation, nearly 100%.
The assessment methods used in this case report have a number of strengths. They are non-invasive, quick and easy to use, pain-free and not susceptible to extraneous noise. In addition, they are objective and give real-time feedback which can be extremely beneficial for patients. Following such an ACIF operation, assessment is typically carried out during control visits with the surgeon or a rehabilitation clinic where a more subjective measure of outcome is used. Under such visits the patient would normally be assessed by the degree of, and extent to which voluntary flexion is possible. With mfBIA and AMG, improvement can be detected and quantified (slow/fast) much earlier than any feeling of recovery by the patient or assessment by the surgeon or therapist. In this case the methods used had the additional psychological effect on the patient of motivating him to adhere to the rehabilitation programme, perhaps accelerating his recovery. However, whilst the effects of TENS stimulation cannot be determined in this case report, the benefits of such treatment are very likely to have speeded up the recovery of the injured nerve [3].
It is known that muscles with minimal or no nervous stimulation suffer from atrophy to a degree that may make full recovery of movement difficult [1,2]. Another reason for the use of field stimulation was to reduce the risk of trans-spinal compensation, affecting the otherwise healthy arm [8,9]. For ethical reasons, we therefore initiated a protocol of field stimulation (TENS) of m. Biceps brachii one month after surgery, since the patient had no visible control of the muscle, and atrophy was a real concern. Despite this lack of visible motor control for the affected muscle, our AMG method revealed a voluntary signal, albeit greatly decreased compared to the healthy arm, and this signal gradually improved over the year of measurement.
Our approach for this study was to use both a static and a dynamic assessment of the affected muscle, as well as the healthy arm by way of a control. We used the first set of measurements (mfBIA & AMG) to make sure that any possible trans-spinal compensation affecting the healthy arm could not influence our further assessments [8,9].
Multi-frequency Bioimpedance (mfBIA)
The mfBIA measurements were always recorded prior to any voluntary or TENS activated movements. This ensured that the movement protocol did not influence the mfBIA parameters and the data represent the optimal state of the affected muscle. The initial high R value is most likely indicative of dehydration/perfusion issues in the injured arm, that quickly became corrected (Figure 1B). The correction of the R value occurs following the start of the field stimulation protocol (TENS), which serves to gently massage the upper arm tissues and facilitate the venous pumps and lymphatic drainage through muscle fibre contractions. The Xc and Z changes (Figure 1A & 1C) support this finding, as does the PA value (Figure 1D) which is a ratio of R/Xc and correlates with overall cellular health [5,6,10]. Values for fc are initially very comparable with the healthy arm, but subsequently show an increase which remains over time and is suggestive of an increased resting tension in the muscle (Figure 1E). The Re values are indicative of dehydration/perfusion issues initially but could also be due to fibre damage (Figure 1F). Mc shows an initial improvement as though the internal cellular environment was restoring itself, before worsening, most likely the effect of the patient starting to be able to exercise and overuse this muscle (Figure 1G). Likewise, Ri which has been closely correlated with cellular oxygen consumption (cellular metabolism) [11,12] showed an initial improvement, before becoming more erratic and raised compared to the healthy arm (Figure 1H).
With over training, particularly in the early stages of recovery (measurement 4), there are changes in the mfBIA parameters that coincide with the over-use of this weak muscle; e.g. especially Mc showing a drop in membrane capacitance representing a higher level of trans-membrane transport, an increase in fc indicative of increased resting tension, and a drop in PA which denotes impaired cellular health. The last measurement also showed signs of over exercise [4], and the patient mentioned that he had been lifting a weight the day before and that that activity had been for a prolonged period.
Acoustic Myography (AMG)
The dynamic assessment of this affected muscle was achieved using acoustic myography. This technique records fibre use in muscle contractions, expressing the recorded signal as both spatial- (number of active fibres at any point in time; S-score) and temporal-summation (firing frequency of active fibres; T-score) as well as the efficiency with which muscle fibres are recruited for any given contraction (E-score).
The spatial summation data (S-score) can be seen in Figure 2, where both slow and fast voluntary rotation movements (diadochokinesis) of the affected arm are plotted over time. There was a clear improvement in the spatial summation parameter both during slow and fast movements, although the improvements were temporarily affected by two initial periods of over exercise (4th and 8th measurements). It should be noted that in this case an improvement in the S-score indicates that fewer fibres were recruited for any given movement.
Of interest is the last measurement, where the patient explained that he had over exercised the day before. This was indeed supported by the mfBIA data, yet interestingly, the AMG data did not show a decrease in signal amplitude (S-score; Figure 2) unlike the two earlier occasions of over exercise. This could be interpreted as indicating that the muscle fibres in the injured arm had recovered to an extent that a mild period of over exercise did not have a detrimental effect on muscle function as assessed by a brief period of voluntary exercise. However, the P2 measurement revealed that 20 minutes of TENS stimulation at a higher frequency (80-100 Hz) resulted in fatigue, which is not observed in the healthy arm. Clearly full recovery of function in the injured arm had not been achieved at 12 months, although the patient had returned to his normal daily activities. Finally, the changes in the T- and E-scores for the AMG measurements support the findings of improvement in this patient.
mfBIA and AMG combined show great potential in assessing patients who have experienced nerve damage with resulting loss of muscle function. Improvement can be followed at a very early stage of rehabilitation, even when the clinical assessors and the patient himself cannot detect any change. This will help the patient to comply with the rehabilitation programme and the therapist to follow any benefits, as well as make any necessary adjustments. The TENS muscle stimulation therapy seems, furthermore, to be advantageous from a physiological point of view, although documentation for this is now needed.
Declarations
Acknowledgements: The authors wish to thank the patient for participating in the study and adhering so well to the protocol. The patient has read and accepted the manuscript.
Competing interests: APH has been involved in developing the CURO and setting up a company to manufacture and sell the units; CURO-Diagnostics ApS, but this has had no influence on the data collection. EMB has no interests to declare and was responsible for the protocol.
References
- Lepley LK, Davi SM, Burland JP, Lepley AS. Muscle Atrophy After ACL Injury: Implications for Clinical Practice. Sports Health. 2020; 12(6): 579-586. DOI: 10.1177/1941738120944256
- Kostrominova TY. Skeletal Muscle Denervation: Past, Present and Future. Int J Mol Sci. 2022; 23(14):7489. DOI: 10.3390/ ijms23147489.
- Bu A, Afghah F, Castro N, Bawa M, Kohli S, Shah K, et al. Actuating extracellular matrices decouple the mechanical and biochemical effects of muscle contraction on motor neurons. Advanced Healthcare Materials. 2024; 2403712.
- Bartels EM, Andersen EL, Olsen JK, Kristensen LE, Bliddal H, Danneskiold-Samsøe B, et al. Muscle assessment using multi-frequency bioimpedance in a healthy Danish population aged 20– 69 years: a powerful non-invasive tool in sports and in the clinic.Physiol Rep. 2019; 7(11): e14109. DOI: 10.14814/phy2.14109 https://doi.org/10.14814/phy2.14109
- Bartels EM, Sorensen ER, Harrison AP. Multi-frequency bioimpedance in human muscle assessment. Physiol. Rep. 2015; 3: e12354.
- Harrison AP. A more precise, repeatable and diagnostic alternative to surface electromyography– an appraisal of the clinical utility of acoustic myography, Clin Physiol Funct Imaging. 2018; 38: 312-325. DOI: 10.1111/cpf.12417
- Bartels EM, Olsen JK, Andersen EL, Danneskiold-Samsøe B, Bliddal H, Kristensen LE, Harrison AP. Muscle function assessed by the non-invasive method acoustic myography (AMG) in a Danish group of healthy adults, Current Research in Physiology. 2020; 2: 22–29 DOI: 10.1016/j.crphys.2020.02.002
- Song Y, Forsgren S, Yu J, Lorentzon R, Stål PS. Effects on Contralateral Muscles after Unilateral Electrical Muscle Stimulation and Exercise. PLOS One. 2012; 7(12): e52230. DOI:10.1371/journal.pone.0052230
- Mastalerz A, Sadowski J. The effect of unilateral training on contralateral limb power in young women and men. Biol Sport. 2020; 37(4): 443-448. DOI: 10.5114/biolsport.2021.102208.
- Ivorra A. Bioimpedance monitoring for physicians: an overview. Centre National de Microelectronica, Barcelona. 2003.
- Stahn A, Strobel G, Terblanche E. VO(2max) prediction from multi-frequency bioelectrical impedance analysis. Physiol. Meas. 2008; 29: 193–203.
- Stahn A, Terblanche E, Grunert S, Strobel G, 2006. Estimation of maximal oxygen uptake by bioelectrical impedance analysis. Eur. J. Appl. Physiol. 96:265–273.