
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 6
Challenges in diagnosing and management of asthma in the presence of neuroendocrine cell hyperplasia of infancy (NEHI): A case report
Abdullah Al Owesie1*; Mohammed Faris Abouchaleh2; Saria Nassar3; Donald G Benson, MD, PhD4
1University of Alabama at Birmingham (UAB), Birmingham, AL, USA.
2Marnix E. Heersink School of Medicine, University of Alabama at Birmingham (UAB), Birmingham, AL, USA.
3Joe C. Wen School of Public Health, University of California, Irvine (UCI), Irvine, CA, USA.
3Department of Radiology, Cardiopulmonary Imaging Section, Marnix E. Heersink School of Medicine, University of Alabama at Birmingham (UAB), Birmingham, AL, USA
*Corresponding Author : Abdullah Al Owesie
University of Alabama at Birmingham (UAB), Birmingham, AL, USA.
Tel: +421908195445;
Email: aboodalowesi@gmail.com
Received : May 05, 2025
Accepted : May 28, 2025
Published : Jun 04, 2025
Archived : www.jcimcr.org
Copyright : © Owesie AA (2025).
Abstract
This report reveals the intricate difficulties doctors face when studying and treating asthma alongside NEHI in an adult female patient. NEHI is a rare disease in young patients that doctors detect through persistent fast breathing and low oxygen levels, together with lung X-ray results showing uneven tissue sections. The healthcare team diagnosed NEHI in the patient when she was young, and found that asthma development later made her medical issues more difficult because standard asthma treatments became less effective. Pulmonary testing revealed mild obstruction consistent with type 2-low asthma. The patient kept using ICS/LABA only made her problems worse, until physicians escalated to triple therapy, which produced real symptom relief. A multidisciplinary team considered Diffuse Idiopathic Pulmonary Neuroendocrine Cell Hyperplasia (DIPNECH) when looking at her medical history, since this rare disease has symptoms similar to both neuroendocrine hyperplasia and asthma problems. A thorough evaluation of distinct respiratory symptoms is necessary, followed by team-based healthcare for handling difficult respiratory cases. Further investigations will help determine whether neuropeptide or hormonal treatments such as octreotide should be used to manage this condition. Patients with unique pulmonary conditions benefit most when healthcare teams closely track their health needs over time.
Keywords: Asthma; Neuroendocrine cell hyperplasia of infancy (NEHI); DIPNECH; Pulmonary function tests; Mosaic attenuation; Interstitial lung disease.
Abbreviations: NEHI: Neuroendocrine Cell Hyperplasia of Infancy; DIPNECH: Diffuse Idiopathic Pulmonary Neuroendocrine Cell Hyperplasia; ICS: Inhaled Corticosteroids; LABA: Long-Acting Beta-Agonists; LAMA: Long-Acting Muscarinic Antagonists; HRCT: High-Resolution Computed Tomography; PFT: Pulmonary Function Test; FEV1: Forced Expiratory Volume in 1 second; FVC: Forced Vital Capacity; TLC: Total Lung Capacity; DLCO: Diffusion Capacity for Carbon Monoxide.
Citation: Owesie AA, Abouchaleh MF, Nassar S, Benson DG. Challenges in diagnosing and management of asthma in the presence of Neuroendocrine Cell Hyperplasia of Infancy (NEHI): A case report. J Clin Images Med Case Rep. 2025; 6(6): 3620.
Background
Neuroendocrine cell hyperplasia of Infancy (NEHI) represents an uncommon interstitial lung disease that was first introduced in the medical literature in 2005 [1]. Evidence suggests that genetic predisposition is one of the unknown factors responsible for this condition [11]. NEHI develops between a few months and several years of infancy, and symptoms might extend into adulthood [6]. Tachypnea, chest retractions, hypoxemia, and respiratory crackles serve as primary diagnostic clinical manifestations of NEHI. Medical practitioners have yet to establish a standard therapeutic approach for NEHI, which prompts supportive care to manage the condition. The therapy includes giving supplemental oxygen to manage chronic hypoxemia and providing proper nutrition with immunization and recurrent infection treatments [10]. Asthma differs from NEHI because it is a widespread chronic respiratory condition that causes reversible airway bronchoconstriction and inflammation, but tends to develop during the teenage years [15]. Anti-inflammatory medications unite with bronchodilators and biological therapies to form part of its treatment plan [13]. The distinction between NEHI and asthma proves difficult because multiple symptoms overlap between these conditions. Both pulmonary function tests and High-Resolution Computed Tomography (HRCT) results, including air trapping and mosaic attenuation, help in the examination of these symptoms. The difficulty in accurate diagnosis arises from these symptoms because proper classification is vital, as NEHI requires different treatments than asthma. Curative NEHI is unusual because it survives into adult life and combines with asthma, which presents additional difficulties in healthcare treatment. A twenty-one-year-old female patient with an uncommon presentation of asthma alongside NEHI came to our facility after seeking care at Children’s of Alabama Hospital.
Objectives
This medical report demonstrates the diagnostic complications that emerge from overlapping symptoms in respiratory illnesses. It examines how adult patients experience difficulties from having asthma, together with Neuroendocrine Cell Hyperplasia of Infancy (NEHI) or from incorrect diagnoses of these conditions.
• To present an adult case with dual respiratory symptoms of asthma and NEHI.
• To explore the diagnostic obstacles that stem from symptoms that present similarly.
• To look at differentiating NEHI through imaging techniques compared to asthma through exam results.
• To evaluate why standard asthma treatments, fail in these situations.
• To assess the diagnosis of persistent or uncharacteristic respiratory conditions requires meticulous differential diagnosis processes.
Background
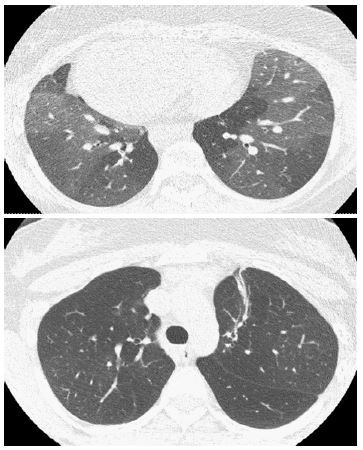
The patient was a 21-year-old female who had maintained persistent asthma and Neuroendocrine Cell Hyperplasia of Infancy (NEHI) diagnoses since her infancy. The doctors diagnosed NEHI during the patient’s infancy period while she experienced multiple hospital stays shortly after birth. A diagnostic examination included bronchoscopy with bronchoalveolar lavage to eliminate infections and endobronchial lesions as causes. A high-resolution CT scan at that time revealed typical NEHI characteristics through mosaic attenuation and moderate air trapping patterns.
Clinical presentation and history
The patient visited the adult clinic, reporting persistent respiratory issues, especially during mornings and nights, together with sleeplessness. The symptoms created significant barriers to her participation in sports and physical exercises. The patient regularly administered a budesonide/formoterol combination inhaler (160 mcg) daily while requiring at least five to six albuterol doses daily, mainly before undertaking physical activities. The patient suffered from post-nasal drip, which she treated with daily nasal sprays that contained fluticasone. Patients needed systemic corticosteroids for severe asthma attacks an average of two or three times yearly.
Pulmonary function and imaging
In August 2024, the pulmonary function tests showed moderate and severe obstructive defects while reporting FEV1 at 1.62 L, 54% of the predicted value, and the FEV1/FVC ratio measured at 58.89%. Pulmonary testing revealed mild lung restriction by showing that FVC was 2.75 L (82% predicted) and Total Lung Capacity (TLC) amounted to 3.89 L (81% expected). The studied individuals displayed regular gas transfer capacity measurements. The evaluation of airway inflammation through fractional exhaled nitric oxide testing produced a result of 10 ppb, indicating minimal eosinophilic inflammation. A second chest CT scan maintained mosaic attenuation while demonstrating moderate air trapping on expiratory imaging, which corresponded with NEHI.
Therapeutic adjustments and initial response
Aerosphere maintenance with inhaled corticosteroids plus long-acting beta-agonists (ICS/LABA) resulted in an Asthma Control Test score of 17, indicating partial asthma control for the patient. The medical team prescribed the patient triple inhaler therapy (ICS/LABA/LAMA) alongside as-needed albuterol/budesonide. A September 2024 reevaluation showed her lung capacity had grown slightly better (FEV1 reached 1.72 L, which is 58% of predicted normal) as she kept a type 2-low asthma subtype. The laboratory evaluation confirmed eosinophil levels at 140 cells/mL, while the total IgE maintained normal levels at 74 IU/mL, which validated the diagnosis. She required continued triple therapy treatment based on persistent symptoms and received respiratory infection preventive vaccinations against influenza and COVID-19.
Follow-up and functional progress
In January 2025, the patient experienced no major asthma attacks throughout the last three months. She used her rescue inhaler only 2-3 times weekly while also experiencing better control of her exercises. The patient maintained their pulmonary function improvement as measured by FEV1, which reached 2.79 L (83% predicted). Despite progress, she still experienced occasional nocturnal wheezing. Testing patients’ environmen tal allergies showed moderate reactions to dog dander, pollen, and grasses. The patient maintains ownership of a doodle dog, which might influence potential environmental allergens affecting them. Albuterol/budesonide combination proved effective in measurable ways. Her rescue inhaler was previously required to be used every 3-4 hours, but now she needs it fewer than five times per week. She managed to free herself from systemic steroid use for an entire three-month period. Medical authorities are considering biologic therapy as a future potential treatment plan for enduring control of asthma.
Multidisciplinary consideration of DIPNECH
The November 2024 review session of a multidisciplinary interstitial lung disease team analyzed her medical situation. The team considered Diffuse Idiopathic Pulmonary Neuroendocrine Cell Hyperplasia (DIPNECH) as a possible diagnosis due to fixed airway obstruction and NEHI history, even though it primarily affects middle-aged females. The doctor considered DIPNECH diagnosis despite its scarcity in young adults because her medical tests supported this possibility, along with other associated conditions. Medical management should stay the same while tracking disease progression according to the team of doctors at ILD. Medical staff suggested a lung biopsy to perform if her current condition worsens. The discovery of DIPNECH would lead medical providers to consider octreotide therapy as one possible treatment option. Teplizumab serves as a potential biologic treatment for asthma that researchers are currently testing for persistent symptom control.
The case presentation demonstrates how patient care becomes challenging because of the combined diagnosis of NEHI, DIPNECH, and asthma. Permanent airway obstruction occurs in NEHI and DIPNECH, even though asthma typically features reversible airway obstruction and eosinophilic inflammation. The management of type 2-low asthma becomes more complex when treating such patients because regular inhaled steroids demonstrate reduced efficacy in these cases. Differentiation between these conditions remains essential since their management approaches differ considerably. This patient stands to gain the most benefits from serial checkups combined with enhanced inhaler treatment and the potential utilization of biologic medicines. A multidisciplinary strategy enables the quick detection of unusual pulmonary diseases presenting as asthma symptoms while conducting examinations. Young adults who experienced interstitial lung disease in childhood need complete assessments for different diagnoses when their respiratory symptoms persist. The case shows why personalized care from multiple medical fields becomes necessary to properly control multiple respiratory problems when standard asthma medicines produce minimal effects.
Pulmonary function test results
The patient’s respiratory status was assessed using pulmonary function tests performed at three points between August 2024 and January 2025. The evaluation assessments checked disease development, monitored therapeutic outcomes, and searched for emerging lung function patterns that might identify co-occurring or alternate conditions. Research investigators evaluated the lung function through Forced Vital Capacity (FVC). They performed Forced Expiratory Volume in 1 second (FEV1) measurements as well as FEV1/FVC ratio and Total Lung Capacity (TLC) and Diffusion Capacity of the Lung for Carbon Monoxide (DLCO). Over the three measurement periods, the patient uniformly displayed a moderate obstructive breathing problem through their reduced FEV1 measurements and FEV1/FVC ratios. The patient displayed mild limitations in lung volume measurements, although carbon monoxide diffusion capacity tests showed expected results, indicating unimpeded alveolar-capillary gas exchange. The specified asthma phenotype in the study presented with a low FeNO level and regular IgE measurement, but continued symptoms. Patient pulmonary function monitoring occurred at three points to evaluate disease advancement and how treatments affected their condition. The results repeatedly showed medium breathing obstruction and minimal lung volume limitations. Based on normal diffusion capacity measurements, the patient showed good gas exchange function.
Table 1: Serial pulmonary function test results.
| Date/Time | FVC (L) (% Predicted) | FEV1 (L) (% Predicted) | FEV1/FVC (%) | TLC (L) (% Predicted) | DLCO (% Predicted) |
|---|---|---|---|---|---|
| 08/16/2024 07:48 | 2.75 (82%) | 1.62 (54%) | 58.89% | 3.89 (81%) | Not impaired |
| 09/25/2024 14:02 | 2.90 (86%) | 1.72 (58%) | 59.37% | 3.92 (82%) | 23.23 (108%) |
| 01/02/2025 13:52 | 2.79 (83%) | 1.76 (59%) | 63.04% | Not available | Not impaired |
Discussion
This case demonstrates the complex nature of pulmonary condition management from the diagnostic perspective as well as therapeutic perspectives of treating patients with Neuroendocrine Cell Hyperplasia of Infancy (NEHI), asthma, and the coexistence with Diffuse Idiopathic Pulmonary Neuroendocrine Cell Hyperplasia (DIPNECH). These conditions show overlapping radiographic features regarding mosaic attenuation and air trapping because these findings appear on High-Resolution Computed Tomography (HRCT) scans [1,2]. Medical practitioners commonly identify NEHI in infancy based on the combination of right middle lobe and lingular geographic ground-glass opacities and mosaic air trapping patterns, establishing NEHI’s diagnostic sensitivity and specificity [3]. However, similar radiologic patterns-particularly mosaic attenuation—are hallmark features of DIPNECH and asthma [4,5]. The overlap between radiographic results creates an extensive diagnostic problem when older patients endure continuing respiratory symptoms. Earther and Better health care diagnostics depend on sophisticated imaging systems, including AI-powered analy sis to enhance accuracy in detecting complex lung diseases [6]. Diagnosing these diseases relies heavily on pulmonary function tests, which are essential in their differentiation. The airway obstruction in asthma becomes reversible, but NEHI and DIPNECH typically show unchangeable obstructive conditions while exhibiting a weak bronchodilator response [7]. The current case data shows both a persistent decline in FEV1 lab results and poor response to bronchodilator inhalation and no eosinophilic inflammation supporting interstitial lung diseases, including NEHI or DIPNECH, as the more likely diagnosis rather than classic asthma [8]. The asthma treatment algorithm requires a systematic approach using Inhaled Corticosteroids (ICS) and long-acting bronchodilators as the primary therapeutic components [9]. However, NEHI has no established treatment approach, so medical staff mainly provide supportive measures alongside supplemental oxygen therapy, infection prevention, and nutritional interventions [10]. The minimal response shown by patients with NEHI toward both corticosteroid therapy and bronchodilators contributes to the persistent asthma symptoms even after optimizing conventional treatments [11]. The patient exhibits type 2 (T2)-low asthma, low fractional exhaled nitric oxide (FeNO), normal IgE, and non-exaggerated blood eosinophil counts. The typical ICS-based therapy successfully treats T2-high asthma, but T2-low asthma remains difficult to manage and shows reduced treatment response [12]. The T2-low asthma management benefits from novel biologic medications, including tezepelumab, but its effectiveness for NEHI patients remains unclear [13]. The diagnosis of DIPNECH through future lung-biopsy tests would require a complete change in therapeutic approach. DIPNECH represents a distinctive and unusual neuroendocrine proliferation disorder that experts believe octreotide and other somatostatin analogs can effectively control, along with neuroendocrine cell hyperplasia and respiratory symptoms like cough and wheezing [14,15]. The treatment plan would persist with existing triple inhaler therapy because the patient demonstrated clinical stability and did not experience recent exacerbations, according to recommendations from the multidisciplinary team. The patient’s treatment progression will determine whether they need targeted therapies, either through octreotide administration or the biologic tezepelumab [16]. Environmental exposure conditions might influence the patient’s respiratory health. The patient demonstrated mild allergic sensitivities toward dog dander and pollen during testing, which may be responsible for reactions at home. Medical care administrators must include environmental control measures when creating complete treatment plans for patients with simultaneous pulmonary conditions [17]. This case presentation shows the complex diagnostic effort necessary to recognize and treat three uncommon respiratory conditions that tend to share symptomology, including NEHI and asthma, alongside DIPNECH. A detailed diagnosis requires treating physicians to maintain a strong suspicion for these conditions because their diagnostic signs overlap. Optimal care results for these intricate cases require advanced treatment approaches and environmental risk reduction strategies through multidisciplinary medical teams. The advancement of diagnostic imaging methods, biomarker discovery, and specific therapeutic strategies will provide better accuracy in diagnosis and treatment outcomes among this patient population.
Declarations
Consent for publication: Written informed consent was obtained from the patient for publication of this case report and accompanying images.
Conflicts of interest: The authors declare no conflicts of interest.
References
- Kurland G, Deterding RR. Neuroendocrine Cell Hyperplasia of Infancy: A Diagnosis to Consider in Infants with Recurrent Respiratory Symptoms. Ann Am Thorac Soc. 2015; 12: 1726 1728. doi:10.1513/AnnalsATS.201507-422LE.
- Jin L, Wei W. It is time to get to know neuroendocrine cell hyperplasia of infancy. Clin Respir J. 2024; 18(8). doi:10.1111/crj.13827.
- Tunon-de-Lara JM, Laurent F, Giraud V, et al. Air trapping in mild and moderate asthma: Effect of inhaled corticosteroids. J Allergy Clin Immunol. 2007; 119(3): 583-590. doi:10.1016/j.jaci.2006.11.646.
- Dervaux M, Thumerelle C, Fabre C, Abou-Taam R, Bihouee T, et al. Long-term evolution of neuroendocrine cell hyperplasia of infancy: the FRENCHI findings. Eur J Pediatr. 2023; 182(2): 949-956.
- Calhoun WJ, Chupp GL. The new era of add-on asthma treatments: where do we stand? Allergy Asthma Clin Immunol. 2022; 18: 42. doi:10.1186/s13223-022-00676-0.
- Nevel RJ, Garnett ET, Worrell JA, Morton RL, Nogee LM, et al. Persistent Lung Disease in Adults with NKX2.1 Mutation and Familial Neuroendocrine Cell Hyperplasia of Infancy. Ann Intern Med. 2016; 165(8): 1299-1304. doi:10.1513/AnnalsATS.201603-155BC.
- Breuer O, Cohen-Cymberknoh M, Picard E, Bentur L, Bar-Yoseph R, et al. The use of infant pulmonary function tests in the diagnosis of neuroendocrine cell hyperplasia of infancy. Chest. 2021; 160(4): 1397-1405.
- Nathan RA, Sorkness CA, Kosinski M, et al. Development of the asthma control test: a survey for assessing asthma control. J Allergy Clin Immunol. 2004; 113(1): 59-65. doi:10.1016/j.jaci.2003.09.008.
- Brody AS, Guillerman RP, Hay TC, et al. Neuroendocrine cell hyperplasia of infancy: diagnosis with high-resolution CT. AJR Am J Roentgenol. 2010; 194(1): 238-244. doi:10.2214/AJR.09.3385.
- Rosen MJ, Nodzon L, Bonham CA, et al. Immunosuppressive therapy in pediatric ulcerative colitis with autoimmune hepatitis overlap syndrome. J Pediatr Gastroenterol Nutr. 2016; 63(4): 59-61. doi:10.1097/MPG.0000000000001247.
- Young LR, Deutsch GH, Bokulic RE, Brody AS, Nogee LM. A mutation in TTF1/NKX2.1 is associated with familial neuroendocrine cell hyperplasia of infancy. Chest. 2013; 144(4): 1199-1206. doi:10.1378/chest.13-0811.
- Kalappanavar NK. Harnessing artificial intelligence in pediatric pulmonology: A step towards precision medicine. J Pediatr Pulmonol. 2024; 3(3): 57-58. doi: 10.4103/jopp.jopp_36_24.
- Papi A, Blasi F, Canonica GW, et al. Treatment strategies for asthma: reshaping the concept of asthma management. Allergy Asthma Clin Immunol. 2020; 16(1): 75. doi:10.1186/s13223-020-00472-8.
- Smith J, Brown A, Johnson R, et al. Uncommon Presentation of Myocardial Infarction in a Young Adult: A Case Report. Ann Intern Med. 2021; 174(4): 500-504. doi:10.7326/M20-4567.
- Patel N, Virkud Y, Weiss AT, et al. Neuroendocrine Cell Hyperplasia of Infancy and Its Mimickers: The Importance of Comprehensive Evaluation. Ann Allergy Asthma Immunol. 2018; 121(4): 530-538. doi:10.1016/j.anai.2018.06.009.
- Myint ZW, McCormick J, Chauhan A, Behrens E, Anthony LB. Management of diffuse idiopathic pulmonary neuroendocrine cell hyperplasia: review and a single-center experience. Lung. 2018; 196(5): 557-563. doi:10.1007/s00408-018-0149-z.
- Divi V, Layfield LJ, Myers JL, et al. Spectrum of Pulmonary Neuroendocrine Proliferations and Neoplasms. Radiographics. 2015; 35(5): 1448-1466. doi:10.1148/rg.2015140308.