
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 6
Effect of photobiomodulation on joint regeneration in patient with temporomandibular joint disorder: Case report
Mayra Costanti Vilela Campos1*; Patrícia de Viveiros Tavares Alves1; Marianna Delle Serre Tanganeli2; Lara Jansiski Motta1; João Paulo Colesanti Tanganeli3
1Department of Biophotonics Medicine, Universidade Nove de Julho (UNINOVE), São Paulo, State of São Paulo, Brazil.
2Universidade Estadual Paulista (UNESP), São José dos Campos, State of São Paulo, Brazil.
3APCD School of Dentistry, São Paulo, State of São Paulo, Brazil.
*Corresponding Author : Mayra Costanti Vilela Campos
Avenida Presidente Vargas, 40 Sala 05 – Centro, Campo Limpo Paulista - São Paulo CEP 13230-100, Brazil.,
Email: mayra.vilela@uni9.edu.br
ORCID ID: 0000-0002-6301-4667
Received : May 15, 2025
Accepted : Jun 09, 2025
Published : Jun 16, 2025
Archived : www.jcimcr.org
Copyright : © Campos MCV (2025).
Abstract
Introduction: Degenerative processes affecting the temporomandibular joint (TMJ) are common in the elderly but can occur at different ages, frequently causing pain. Conventional and minimally invasive treatments are often considered palliative, as they aim at pain control and functional restoration. In some cases, joint replacement with prosthetics may be necessary, an expensive procedure with patient impact and no guaranteed success.
Objective: To report the clinical evolution of a patient and the qualitative imaging aspects of a degenerating TMJ before and after treatment with photobiomodulation and nutraceutical supplementation.
Methods: Supplementation with 500 mg Glucosamine Sulfate, 400 mg Chondroitin Sulfate, 300 mg PEAFLAN®, 40 mg B2 Cool Galena® for 60 days. Application of an 808 nm laser to four periarticular points for 10 weeks, once a week. Cone beam CT before and after treatment, digital caliper for measuring mouth opening, and a visual analog scale for pain assessment at the beginning and end of treatment. Results: The final CT scan showed qualitative differences in the uniformity of the mandibular head contour. The right TMJ, initially with severe erosion, demonstrated only flattening in the same region. There was an increase in mouth opening, and pain reached the minimum score on the scale in the final session. Conclusion: Photobiomodulation demonstrated analgesic and anti-inflammatory effects and shows regenerative potential for TMJ, requiring randomized clinical trials to confirm its effectiveness.
Keywords: Temporomandibular disorders; Orofacial pain; Photobiomodulation; Temporomandibular joint osteoarthritis; Low-intensity laser therapy.
Abbreviations: TMJ: Temporomandibular Joint; TMD: Temporomandibular Disorders; NSAIDs: Non-Steroidal Anti-Inflammatory Drugs; PBM: Photobiomodulation; DC/TMD: Diagnostic Criteria for Temporomandibular Disorders; VAS: Visual Analog Scale; CT: Computed Tomography; LED: Light Emitting Diode; LASER: Light Amplification by Stimulated Emission of Radiation; MIC: Maximum Intercuspation.
Citation: Campos MCV, Alves PVT, Tanganeli MDS, Motta LJ, Tanganeli JPC. Effect of photobiomodulation on joint regeneration in patient with temporomandibular joint disorder: Case report. J Clin Images Med Case Rep. 2025; 6(6): 3636
Introduction
Temporomandibular disorder (TMD) is defined as a set of signs and symptoms, involving the masticatory muscles, TMJ, and associated structures. It is estimated that TMD affects approximately 5% to 15% of the adult population, with symptoms found in 50% of adults, making it a public health issue as it is the primary cause of non-dental pain and the second most common musculoskeletal disorder after lower back pain [1-3].
According to the 4th edition of the American Academy of Orofacial Pain (AAOP) manual, TMD diagnosis and classification are divided into two main groups: muscular TMD and articular TMD, each with respective subdivisions. Articular dysfunctions include condyle-disc disorders, structural incompatibilities of the articular surfaces, and inflammatory disorders such as arthritis, osteoarthritis, osteoarthrosis, and polyarthritis. Osteoarthritis is a degenerative disease involving cartilage degradation, subchondral bone remodeling, synovitis, and chronic pain. TMJ degeneration affects both hard and soft tissues, leading to pain, dysfunction, and reduced quality of life. Studies indicate that TMJ degeneration begins as early as age 14, increasing with age, suggesting that individuals over 65 with TMD exhibit the degenerative form of the disease [1,4-7].
In cases of TMJ degeneration, the treatment goal is to control and prevent cartilage and subchondral bone destruction while restoring function and reducing joint pain. Treatment approaches include conservative measures such as physiotherapy and NSAIDs, minimally invasive techniques such as arthrocentesis, and, in advanced clinical stages, joint replacement [6,8].
Among conventional treatments, nutraceuticals and photobiomodulation are noteworthy. Nutraceuticals are bioactive food-derived components scientifically proven effective. The most common supplements for osteoarthritis treatment are glucosamine and chondroitin sulfate, which relieve symptoms and improve tissue structure. Photobiomodulation therapy is increasingly used as a therapeutic procedure for various medical conditions, including edema control, chronic joint disorders, pain management, and wound healing. This therapy activates cellular structures, converting light energy into photochemical energy, triggering biophysical and biochemical reactions that influence cellular metabolism [9-12].
Thus, this study aims to report the qualitative imaging aspects of degenerating TMJ before and after laser therapy combined with nutraceutical supplementation and describe the patient’s clinical evolution during the rehabilitation process.
Experimental section: This study is an observational, descriptive case report. The study design follows international case study recommendations outlined in the STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) statement.
The study adhered to research regulations for human subjects as per the Research Ethics Committee guidelines. The participant provided informed consent in accordance with Resolution 466/12 of the National Health Council.
Collected variables: Sociodemographic information was collected, including age, self-reported skin color, education level, occupation, weight, height, and physical activity habits. In adaddition to sociodemographic data, clinical information was gathered, such as the history of systemic diseases, personal and family health history, past and current treatments, and medications used.
Visual Analogue Scale (VAS) for pain: A unidimensional tool used to assess pain intensity. It consists of a line numbered from 0 to 10, where one end represents “no pain” and the other “worst pain imaginable.” The patient is asked to rate their pain along this line. VAS was applied at the beginning and end of each session.
Digital caliper: A digital caliper was used to assess mouth opening by measuring from the incisal edge of the upper central incisor to the incisal edge of the lower central incisor. Mouth opening measurements were taken during the first and last consultations.
Computed Tomography (CT): Used to obtain images of the cortical bone of the temporomandibular joint. Two CT scans were performed: one before treatment and another 90 days after the start of treatment.
Additionally, a medication record was kept to monitor the need for medication adjustments or the introduction of new medications beyond those initially prescribed.
Therapeutic intervention: The treatment lasted 10 weeks (two and a half months) and included 10 sessions (one session per week), each lasting approximately 30 minutes. After completing the 10-week treatment, a new evaluation was performed. The participant received an application of a GaAIAs and InGaALP semiconductor laser, infrared diode, with a wavelength of 808 nm, power of 100 mW, properly calibrated, and energy of 2J per point (20 seconds) at four periarticular points, as represented in Table 1.
Sessions were conducted in a private room attached to the outpatient clinic, free from sound interference. During the application, only the treated volunteer and the researcher responsible for the treatment were present, both wearing specific protective eyewear. The active laser tip was covered with a disposable transparent plastic (PVC) to avoid cross-contamination and ensure hygiene, and the irradiated area was pre-cleaned with 70% alcohol.
The patient remained seated during applications, with the Frankfurt plane parallel to the ground. Four laser applications were performed at four specific TMJ points: three points in front and one behind the tragus, as shown in Figure 1, for 10 weeks, with a frequency of once per week. Figure 2 represents the treatment flowchart.
At the beginning of treatment, the patient was prescribed nutraceutical supplementation. PEAFLAN 300 mg (Palmitoylethanolamide), B2 Cool Galena 40 mg, and Glucosamine Sulfate 500 mg combined with Chondroitin Sulfate 400 mg were prescribed. The supplementation lasted 60 days.
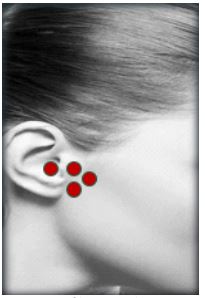

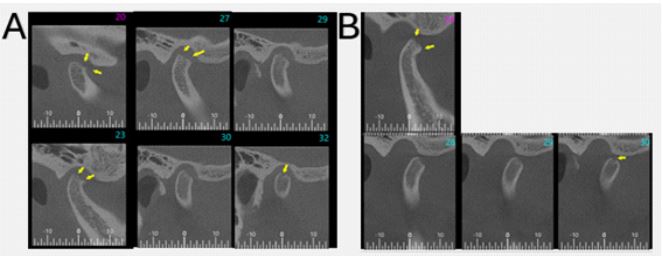
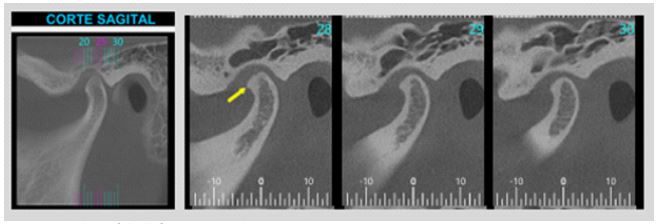
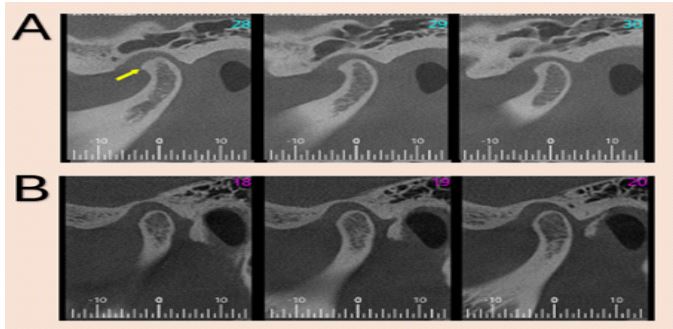
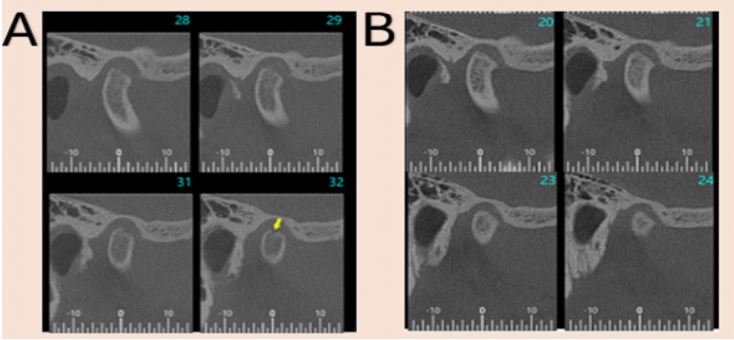
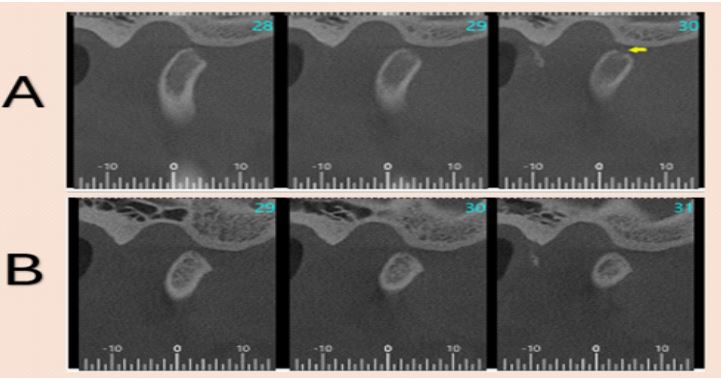
Table 1: Dosimetric parameters for photobiomodulation application.
| Parameters | Infrared laser |
|---|---|
| Wavelength [nm] | 808 |
| Operating mode | Continuous |
| Power [mW] | 100 |
| Aperture diameter [cm] | 0.354 (Beamdiameter with spacer) |
| Beam area[cm²] | 0.0984 (Withspacer) |
| Exposure time[s] | 20 secondsper point |
| Fluence [J/cm²] | 20 |
| Energy [J] | 2Jper point |
| Number of irradiated points | 4 |
| Application technique | Contact |
| Number of sessions | 10 |
| Treatment frequency | Once per week |
| Total irradiated energy [J] | 96J |
The patient underwent dental arch molding for the fabrication of a stabilizing night guard and received instructions on its use.
Results
The patient included in this study, a 45-year-old female, was evaluated on April 3, 2024. Palpation of the masticatory and accessory muscles identified trigger points in the masseter muscle, temporalis, and sternocleidomastoid insertion.
Using a stethoscope, we performed joint auscultation during mouth opening and closing movements and identified sounds recognized as crepitus in both joints. A digital caliper was used to measure the patient’s mouth opening capacity, initially limited to a maximum of 30 mm with pain. Using the visual analog scale (VAS), where 0 represents no pain and 10 the worst pain imaginable, the patient reported an initial pain score of 7, impacting her ability to eat and engage in social interactions. Cone beam CT performed in July 2023 with the mouth open and closed, obtaining coronal, sagittal, and axial slices of 1 mm thickness, showed degenerative changes in the TMJs, more pronounced on the right side.
A qualitative analysis of the right TMJ CT images revealed severe erosion in the anterosuperior pole of the mandibular head, with irregular cortical compromise and the presence of an irregular subcortical cyst (Figure 3). The same tomographic analysis of the left TMJ showed thickening of the anterolateral cortical region of the mandibular head, with early osteophyte formation (Figure 4). In both joints, the articular fossa appeared normal. The patient showed positive clinical progression during treatment. As sessions progressed, pain complaints diminished, with a final VAS score of 0 during palpation and joint function in the last session. Mouth opening also improved, reaching 38 mm without pain.
New CT images were taken one month after treatment completion at the same diagnostic center, using the same CT scanner as in 2023 and analyzed by the same professional, unaware of the treatment performed. Post-treatment CT images showed qualitative differences in the right and left TMJs compared to initial exams. Tomographic cuts revealed a more uniform mandibular head contour in both joints, with osteophyte reduction in the left TMJ (Figure 5). The right TMJ, initially more compromised by degeneration, displayed increased cortical density compared to initial images. The anterosuperior region of the right condyle, initially showing severe erosion, exhibited only flattening in the final CT scan (Figures 6 and 7).
Discussion
Degenerative joint diseases are common as individuals age. Regarding the temporomandibular joint, internal derangement and osteoarthritis are the most prevalent degenerative diseases, associated with pain, functional impairment, and reduced quality of life [9,13]. Treatments that improve joint tissue and patient quality of life. The patient in this study underwent a non-invasive, painless, and accessible treatment using low-power laser therapy combined with nutraceutical supplementation, resulting in pain relief, functional improvement, and favorable changes in the uniformity of the mandibular head contour. Furthermore, the flattening observed in the previously eroded region suggests a potential regenerative effect of the therapy.
Currently, the recommended treatments for temporomandibular disorders include conservative procedures, starting with patient education on their role in treatment, self-monitoring of parafunctional habits, and their correction. The use of a stabilizing night guard is recommended to reduce muscle activity, distribute tension evenly, and protect the temporomandibular joint from dysfunctional stresses. Physiotherapy includes exercises to restore muscle balance and strengthen the musculature, thermal treatment for pain relief in inflammatory situations, and resources such as transcutaneous electrical nerve stimulation (TENS), ultrasound, iontophoresis, and laser therapy [14]. All these treatments aim to relieve pain and improve function, but they do not address the primary cause of symptoms, which is the degenerative joint process.
The patient who received the proposed treatment showed regeneration of the areas affected by the degenerative process in the TMJ. We believe that these changes occurred due to the unique characteristics of the temporomandibular joint, which, although classified as a synovial joint like others, has its condylar cartilage covered by a connective tissue membrane identified as the perichondrium and a powerful niche of mesenchymal stem cells capable of differentiation [15]. In addition to these characteristics, low-level laser therapy was used, which plays an important role in stimulating the production of collagen and proteoglycans, both of which are regenerative agents [16].
The classic signs and symptoms of TMDs include orofacial pain, joint clicking, and limited mouth opening, all of which were present in the patient during the initial evaluation. However, in addition to the joint regeneration demonstrated by cone-beam computed tomography (CBCT) images taken before and after treatment, the patient also showed a clinical improvement, with increased mouth opening and minimal pain scores at the end of treatment. This finding aligns with the literature on photobiomodulation and its anti-inflammatory and analgesic potential, which works by rebalancing the sodium-potassium pump in the peripheral nerve endings of nociceptors, preventing the nerve conduction threshold from being reached and ensuring patient adherence to treatment [16,17].
With the improvement in symptoms and function observed and reported by the patient, the progression of clinical interventions was avoided. This prevented the need to advance from conventional therapies to minimally invasive procedures such as arthrocentesis, which involves intra-articular lavage to remove inflammatory mediators and stimulate the production of new synovial fluid. This is particularly relevant because an inflammatory network sustains the degenerative process, giving it a progressive nature by promoting the production and release of inflammatory cytokines, which exacerbate the degenerative and painful condition and may lead to modifications in bone structures and the articular disc. This technique can be followed by viscosupplementation with hyaluronic acid [13,17,18].
Total TMJ replacement is the next step in the treatment process. However, this procedure involves high costs for the patient, as well as the risk of acute infections (5/8 cases) and late infections (3/8 cases), which may require prosthesis replacement. Additionally, the natural wear of the prosthesis necessitates future replacements. Invasive surgical treatment not only carries significant risks for the patient but also does not always achieve effective management of TMJ degenerative lesions [15,19].
The presented case report demonstrated that joint regeneration was achieved through a non-invasive approach, without risks to the patient, at a low cost, and with high patient adherence by using low-level laser therapy. This technology enhances cellular metabolism, stimulating the synthesis of proteins and enzymes and promoting cell proliferation—one of the five key mechanisms of tissue regeneration. In the case of cartilaginous tissue, this phase is crucial for the formation of chondrocytes, which are responsible for secreting collagen, glycoproteins, and proteoglycans, and originate from chondroblasts in the perichondrium.
In addition to its regenerative capacity, low-level laser therapy also acts as an inflammatory modulator, blocking pro-inflammatory mediators involved in the degenerative process. Chondrogenesis is triggered by bone morphogenetic proteins and growth factors such as TGF-β, whereas cytokines like IL-1β and TNF-α act as suppressors of this process [16,20,21].
The results demonstrated in this case report should encourage clinical trials to explore regenerative tools for the temporomandibular joint, ultimately leading to pain relief and functional recovery. The literature has already highlighted the unique histological characteristics of this joint, including its adaptive and regenerative capacity, as well as the effects of photobiomodulation (PBM) as a tissue-regenerating agent.
Conclusion
Photobiomodulation, in addition to its documented analgesic and anti-inflammatory effects, demonstrated regenerative potential for TMJ. This clinical case, which would have progressed to minimally invasive procedures with limited resolution, pain involvement, and high costs, exhibited condylar bone cortical regeneration with low-power laser therapy. As an accessible, user-friendly device with high patient adherence, further randomized clinical trials are necessary to confirm its effectiveness in similar clinical conditions.
Declarations
Acknowledgments: The authors would like to thank FAOA – Faculdade de Odontologia da APCD, located at Rua Voluntários da Pátria 547, Santana, São Paulo, Brazil.
Author contributions: M.C.V.C. and J.P.C.T. participated in the conception, design, and data collection of the study. M.C.V.C., P.V.T.A and M.D.S.T. drafted the manuscript. J.P.C.T. and L.J.M critically reviewed the manuscript for intellectual content and coordinated the study. All authors read and approved the final manuscript.
Conflict of interest: The authors declare no financial or commercial conflict of interest.
Data availability statement: The data that support the findings of this study are available from the corresponding author upon reasonable request.
References
- Carrara SV, Conti PCR, Barbosa JS. Terms of the 1st Consensus on Temporomandibular Dysfunction and Orofacial Pain. Dental Press J Orthod. 2010; 15: 114-20.
- Lekaviciute R, Kriauciunas A. Relationship between occlusal factors and temporomandibular disorders: A systematic literature review. Cureus. 2024; 16: e54130.
- Ortiz-Culca F, Stupinaro-Capristan P, Alcedo-Moncada D, Pineda-Mejia M, Watanabe-Velazquez R. Association between painful temporomandibular disorders and psychosocial factors in dental students. Brazilian Dental Science. 2024; 27(4): e4413.
- Leeuw R. Orofacial pain: assessment, diagnosis, and treatment guide. 4th ed. São Paulo: Quintessence; 2010.
- Okeson JP. Management of Temporomandibular Disorders and Occlusion. 8th ed. Rio de Janeiro: Editora Guanabara Koogan Ltda; 2020.
- Cui D, Li H, Xu X, Ye L, Zhou X, Zheng L, Zhou Y. Mesenchymal stem cells for cartilage regeneration of TMJ osteoarthritis. Stem Cells Int. 2017; 11: 5979741.
- Yadav S, Yang Y, Dutra EH, Robinson JL, Wadhwa S. Temporomandibular joint disorders in older adults. J Am Geriatr Soc. 2018; 66: 1213-7.
- Albagieh H, Alomran I, Binakresh A, Alhatarisha N, Almeteb M, Khalafb Y, Alqublan A, Alqahatany M. Occlusal splints—types and effectiveness in temporomandibular disorder management. Saudi Dent J. 2023; 35: 70-9.
- D’Adamo S, Cetrullo S, Panichi V, Mariani E, Flamigni F, Borzì RM. Nutraceutical activity in osteoarthritis biology: A focus on the nutrigenomic role. Cells. 2020; 9: 1232.
- Meneguzzo DT, Lopes LA, Pallota R, Soares-Ferreira L, Lopes-Martins RA, Ribeiro MS. Prevention and treatment of mice paw edema by near-infrared low-level laser therapy on lymph nodes. Lasers Med Sci. 2013; 28(3): 973-80.
- Alghadir A, Omar MT, Al-Askar AB, Al-Muteri NK. Effect of low-level laser therapy in patients with chronic knee osteoarthritis: a single-blinded randomized clinical study. Lasers Med Sci. 2014; 29: 749-55.
- Silva MG, Bento VAA, Castillo DB. Efficiency of myofascial release in patients with tension-type headaches: an integrative review. Br J Pain. 2021; 4: 374-8.
- Sembronio S, Tel A, Tremolada C, Lazzarotto A, Isol M, Robiony M. Temporomandibular joint arthrocentesis and microfragmented adipose tissue injection for the treatment of internal derangement and osteoarthritis: A randomized clinical trial. J Oral Maxillofac Surg. 2021; 79: 1447-56.
- Wieckiewicz M, Boening K, Wiland P, Shiau Y, Paradowska-Stolarz A. Reported concepts for the treatment modalities and pain management of temporomandibular disorders. J Headache Pain. 2015; 16: 1-12.
- De Souza Tesch R, Takamori ER, Menezes K, Carias RBV, Dutra CLM, De Freitas Aguiar M, et al. Temporomandibular joint regeneration: Proposal of a novel treatment for condylar resorption after orthognathic surgery using transplantation of autologous nasal septum chondrocytes, and the first human case report. Stem Cell Res Ther. 2018; 9: 1-12.
- De Oliveira MF, Johnson DS, Demchak T, Tomazoni SS, Leal-Junior EC. Low-intensity LASER and LED (photobiomodulation therapy) for pain control of the most common musculoskeletal conditions. Eur J Phys Rehabil Med. 2022; 58: 282-9.
- Ahmad SA, Hasan S, Saeed S, Khan A, Khan M. Low-level laser therapy in temporomandibular joint disorders: a systematic review. J Med Life. 2021; 14: 148-64.
- Bavaresco CS, Grossmann TK, Rehm DS, Grossmann E. Effect of mesenchymal stem cells on the regeneration of structures associated with the temporomandibular joint: a narrative review. Braz J Pain. 2020; 3: 275-9.
- Lypka M, Shah K, Jones J. Prosthetic temporomandibular joint reconstruction in a cohort of adolescent females with juvenile idiopathic arthritis. Pediatr Rheumatol. 2020; 18: 1-7.
- Cruz IBM, Severo AL, Azzolin VF, Garcia LFM, Kuhn A, Lech O. Regenerative potential of cartilage tissue through mesenchymal stem cells: updates, limitations, and challenges. Rev Bras Ortop. 2017; 52: 2-10.
- Magri AMP, Parisi JR, de Andrade ALM, Rennó ACM. Bone substitutes and photobiomodulation in bone regeneration: A systematic review in animal experimental studies. J Biomed Mater Res A. 2021; 109: 1765-75.