
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
The Sinewy Swirls- Angioleiomyoma
Anubha Bajaj*
Histopathologist in A.B. Diagnostics, New Delhi, India
*Corresponding Author : Anubha Bajaj
Histopathologist in A.B. Diagnostics, New Delhi, India
Email: anubha.bajaj@gmail.com
Received : Dec 02, 2020
Accepted : Dec 22, 2020
Published : Dec 27, 2020
Archived : www.jcimcr.org
Copyright : © Bajaj A (2020).
Abstract
Angioleiomyoma is an exceptional, benign, solitary neoplasm originating from tunica media of vascular smooth muscle. The neoplasm commonly represents as a uniform, well defined, solitary, soft, nodular, gradually progressive, bluish or purple lesion commonly beneath <2 centimetres magnitude with an absence of accompanying inflammation. Tumefaction is composed of thickened smooth muscle fibres and vascular channels with circumscribing attenuated fibrous tissue capsule. Additionally, the lesion may denominate organizing thrombus, mature adipose tissue cell aggregates and lymphocytic infiltrate. The neoplasm is immune reactive to desmin, myosin, α-smooth muscle actin, HHF35, calponin and h-caldesmon. Angioleiomyoma necessitates a segregation from angiomyolipoma, leiomyoma with bizarre nuclei, glioblastoma multiforme, arteriovenous malformation, cavernous haemangioma, angiofibroma, primary intracranial myopericytoma, glomus tumour, traumatic neuroma, eccrine spiradenoma, angiolipoma, ganglion cyst, neuroma, fibroma, lipoma, neurofibroma, neurilemmoma, salivary gland neoplasms as mucocoele, pleomorphic adenoma, vascular neoplasms as lymphangioma, haemangioma, pyogenic granuloma or dermoid cyst. Comprehensive surgical excision of the lesion with a tumour -free perimeter is an optimal treatment strategy.
Keywords: Angioleiomyoma, Neoplasm.
Citation: Bajaj A. The Sinewy Swirls- Angioleiomyoma. J Clin Images Med Case Rep. 2020; 1(1): 1003.
Short commentary
Leiomyoma is subdivided into pertinent categories designated as angioleiomyoma and leiomyoma arising from deep-seated soft tissue. Angioleiomyoma is an exceptional, benign, solitary neoplasm which originates from tunica media of vascular smooth muscle. Tumefaction is composed of vascular articulations with thickened smooth muscle fibres and is devoid of elastic tissue. The essentially benign, painful, subcutaneous or deep-seated, dermal neoplasm comprised of vascular configurations and smooth muscle emerges as a morphological continuum to myopericytoma and myofibroma [1]. Angioleiomyoma is additionally designated as an “angiomyoma” or a “vascular leiomyoma”. The neoplasm is usually detected and appropriately categorized upon comprehensive surgical excision [1].
Disease characteristics: As estimated by World Health Organization, angioleiomyoma is a frequently discerned variant of leiomyoma with an incidence of around 74%. Nearly 55.9% instances of the vascular neoplasm appear reddish, bluish or purple whereas roughly 44.1% tumours are grey, white or mucosa-tinged [1,2]. Angioleiomyoma is generally situated within the lower and upper extremities, face or oral cavity although no site of tumour emergence is exempt.
The neoplasm is commonly discerned within middle aged individuals between 30 years to 60 years. Males are incriminated at a median age of 53 years whereas females are implicated at a median age of 38 years [2,3].
Majority of tumefaction are miniature with a tumour diameter below <2.0 centimetres although neoplasms vary from 0.5 centimetres to 2.0 centimetres in magnitude with median dimension of 1.0 centimetre. Symptomatic individuals depict a median tumour magnitude of 1.0 centimetre whereas asymptomatic tumefaction demonstrates a median tumour diameter of 0.7 centimetres [2,3]. Angioleiomyoma is associated with a female predominance, is commonly discerned within lower extremities of female subjects and head and neck or upper extremities in male subjects [2,3]. Malignant metamorphoses is exceptional, emerges as a primary, vascular leiomyosarcoma or malignant tumour reoccurrence of a pre-existing angioleiomyoma and accounts for around 7% of soft tissue sarcomas [2,3].
Clinical elucidation: Angioleiomyoma is a uniform, well defined, solitary, soft, nodular, gradually progressive, bluish or purple lesion commonly beneath <2 centimetres magnitude with an absence of accompanying inflammation. Tumefaction is mobile, tender and demonstrates an elevated superimposed layer of stratified squamous epithelium. Alternatively, an exophytic, nodular, reddish-purple, well circumscribed lesion of varying magnitude with unremarkable superimposed mucosa can be ] discerned [3,5]. The neoplasm manifests as a painful or painless nodule. Concurrent pain is described as paroxysmal, drilling or radiating. Certain centric lesions of oral angioleiomyoma may be painful. Neoplasms confined to the facial region or head are commonly painless [3].
The classic clinical symptom of angioleiomyoma is a painful nodule occurring in association with or absence of tenderness which is discerned in an estimated 45% to 70% individuals. Pain appears on account of stretching of nerves entrapped within the tumour parenchyma or tumour capsule or originates due to efflux of mast cell mediators.
Pain can be paroxysmal and is precipitated by fleeting touch, exposure to wind, cold, menses, variations in extraneous pressure or imperceptible stimuli [3,5]. Morimoto in 1973 categorized angioleiomyoma into three distinctive subtypes denominated as
• solid or capillary subtype which is painful, appears in
an estimated 66% neoplasms and arises within lower
extremities, generally within female subjects [4].
• venous subtype which is painless and is discerned within
males wherein around 23% lesions commonly arise within
the head and neck [4].
• cavernous subtype is exhibited in roughly 11% instances
where in tumours are common within the upper
extremity or head [4]. Angioleiomyoma can delineate an
amalgamation of solid, venous or cavernous subcategories.
Nevertheless, the subtypes are devoid of pertinent clinical
significance. Also, clinical categories do not appear to be
concordant with histological subtypes [4].Angioleiomyoma
confined to the hand is minimally painful and of venous
or cavernous subtype. Pain is engendered due to localized
tissue ischemia arising from contraction of blood vessels
feeding the neoplasm or mediated through nerve fibres
traversing tumour parenchyma. Miniature nerves fibres
are observed entrapped within the tumour capsule or
tumour stroma [5].
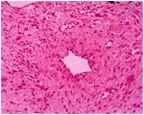
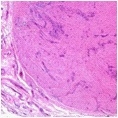
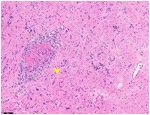
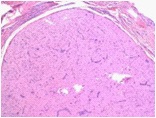
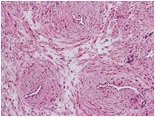
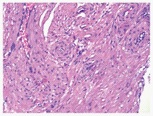
Histological elucidation: Macroscopically, the neoplasm is irregular, lobulated, smooth, spherical, pearly grey and well encapsulated. Tumefaction can emerge as a well demarcated, homogenous nodule confined to deep-seated dermis or arise as a firm, sharply circumscribed, grey/white or brown nodule of magnitude below <2 centimetres. Cut surface is glistening, grey/ white or reddish brown on account of enlarged number of blood vessels [5,6]. On fine needle aspiration cytology, moderate or sparsely cellular smears are composed of uniform, spindle-shaped cells admixed with variable proportion of smooth muscle cells and fragments of collagenous tissue. Macrophages, mature adipose tissue cells or enlarged, ganglion-like cells are occasionally discerned [5,6]. On microscopy, tumour nodule is comprised of thickened smooth muscle fibres and vascular channels circumscribed by an attenuated fibrous tissue capsule. Although constituted by vascular configurations of varying magnitude admixed with smooth muscle fascicles, lesions may denominate organizing thrombus, mature adipose tissue cell aggregates and lymphocytic infiltrate. Miniature foci of hyaline or myxoid alterations are observed [5,6]. The neoplasm exhibits enlarged, vascular channels of diverging calibre encompassed with thickened walls along with irregular dissemination of spindle-shaped cells. Spindle-shaped tumour cells are imbued with elongated, blunt- ended nuclei and eosinophilic cytoplasm. Thereby, smooth muscle bundles are configured which are admixed with interlacing collagen fibres and distended, slit-like vascular articulations.
Smooth muscle fibres configure whorled fascicles adherent to the vessel wall. Atypical mitosis and cellular or nuclear pleomorphism are absent. Well circumscribed fascicles of mature smooth muscle cells are encompassed with vascular lumen layered with normal endothelium and an absence of elastic lamina [5,6].
• solid subtype is composed of compact, closely aggregated
fascicles of smooth muscle.
• venous subtype is comprised of vascular articulations
with thick, muscular walls which intermingle with smooth
muscle bundles.
• cavernous subtype is constituted by distended vascular
channels with minimal quantities of smooth muscle which
commingle with adjacent smooth muscle fascicles [4].
The neoplasm may exhibit foci of cartilaginous or adipose tissue metaplasia or demonstrate bizarre, degenerative
cells recapitulating a symplasmic uterine leiomyoma.
Prominent tumour calcification within acral sites is
exceptional. Scattered epithelioid cells or epithelioid cell
granuloma is infrequently observed. Tumour necrosis,
haemorrhage, mitotic activity, features of vasculitis or
fibromuscular dysplasia are absent [5,6].
Immune histochemical elucidation: Smooth muscle cells are immune reactive to α- smooth muscle actin (α-SMA) in around 90% tumefaction. The neoplasm is immune reactive to desmin, myosin, HHF35, calponin and h-caldesmon. Tumour cells can be highlighted with trichrome stains. Miniature nerve fibres are immune reactive to vimentin, type IV collagen and S100 protein. Endothelial cells are immune reactive to CD34. Nasal lesions are variably immune reactive to progesterone receptors. Proliferative index Ki67 or MIB-1 is minimal [2,3]. The neoplasm is immune non reactive to human melanoma black 45 (HMB-45) antigen, oestrogen receptors or glial fibrillary acidic protein(GFAP) [6,8].
Differential Diagnosis: Angioleiomyoma necessitates a segregation from angiomyolipoma or leiomyoma with bizarre nuclei which can be differentiated as
• angiomyolipoma demonstrates a prominent component
of mature adipose tissue and is immune reactive to human
melanoma black 45 (HMB45) antigen [7].
• leiomyoma with bizarre nuclei is devoid of a prominent
vascular component [7]. Intracranial angioleiomyoma
requires demarcation from diverse entities such
as glioblastoma multiforme (GBM), arteriovenous
malformation (AV), cavernous haemangioma,
angiofibroma (AFM) and myopericytoma(MPC) [8].
• glioblastoma multiforme is an infiltrating, high grade
neoplasm which is a cystic lesion associated with tumour
necrosis, enhanced tumour metabolism, prominent
mitosis and capacity for proliferation. Diffuse vascular
articulations are absent. The neoplasm is immune reactive
to glial fibrillary acidic protein (GFAP) [8].
• arteriovenous malformation (AVM) is an anomaly
comprised of tangled clusters of tortuous arteries, veins
and atypical, interconnected vascular channels [8].
• cavernous haemangioma is composed of peripheral
vascular channels or an enlarged blood filled sinus [8].
• angiofibroma is frequently denominated as a juvenile
nasopharyngeal angiofibroma with accompanying
intracranial extension. The neoplasm is commonly
discerned within teenage males. Juvenile nasal
angiofibroma demonstrates an abundant vascular
component in the absence of smooth muscle component.
The neoplasm is immune reactive to CD34 and is immune non reactive to smooth muscle actin (SMA) [8].
• primary intracranial myopericytoma (MPC) is an
exceptional neoplasm which morphologically recapitulates
angioleiomyoma as the dual conditions are constituted by
myoid- appearing cellular component with diffuse vascular
articulations. However, myopericytoma depicts elliptical
to spindle- shaped cells which concentrically circumscribe
perivascular zones. The neoplasm is immune non reactive
to desmin [8].
Angioleiomyoma emerging as a painful nodule requires segregation from glomus tumour, traumatic neuroma, eccrine spiradenoma or angiolipoma. Tumours confined to the extremity mandate distinction from a ganglion cyst, neuroma, fibroma, lipoma, neurofibroma, neurilemmoma or an inclusion cyst [7,9]. Angioleiomyoma requires a clinical demarcation from mesenchymal neoplasms such as leiomyosarcoma, salivary gland neoplasms as the mucocoele or pleomorphic adenoma, vascular neoplasms as lymphangioma, haemangioma or pyogenic granuloma along with soft tissue cysts as dermoid cyst [7,9]. Angioleiomyoma situated within the hard palate or lesions adjacent to the teeth necessitate distinction from a periodontal lesion [7,9].
Investigative assay: Ultrasonography depicts a well defined, minimally echoic, hyper-vascular tumour nodule with a distinctive tumour perimeter and homogenous intrinsic architecture, indicative of a benign neoplasm.Magnetic resonance imaging (MRI) features are non specific. T2 weighted imaging delineates a mass with mixed foci of hyper-intense and iso- intense regions in concordance with skeletal muscle with a hypo-intense tumour periphery [7,9]. Tumour discernment is adequately achieved with surgical excision and a cogent histological examination [10].
Therapeutic options comprehensive surgical excision of the lesion is an optimal treatment strategy. Tumour associated morbidity is minimal. Oral angioleiomyoma is preferably subjected to surgical excision. Despite an extensive vascular component, profuse surgical haemorrhage is exceptionally encountered [9,10]. Comprehensive surgical extermination with a tumour -free perimeter is recommended in order to circumvent tumour reoccurrence. Localized tumour reoccurrence is exceptional and attributed to incomplete surgical resection or encountered in deep-seated lesions [9,10].


References
- Duhig JT, Ayer JP, et al. Vascular leiomyoma – A study of sixty one cases. Arch Pathol. 1959: 68; 424-30.
- Hachisuga T, Hashimoto H, et al. Angiolieomyoma – A clinicopathologic reappraisal of 562 cases. Cancer. 1984: 54; 126- 130.
- Woo KS, Kim SH, et al. Clinical experience with the treatment of angioleiomyoma. Arch Plast Surg. 2014: 41; 374-378.
- Morimoto N. Angiomyoma (vascular leiomyoma) - A clinicopathologic study. Med J Kagoshima Univ. 1973: 24; 663- 683.
- Chen F, Yuehai P, et al. Primary intracranial angioleiomyoma - a case report and literature review. World Neurosurg. 2020: 138; 145-152.
- Damlar I, Kisa HI, et al. Oral angioleiomyoma of the lower lip - a case report. J Clin Anal Med. 2013: 4 (suppl 5); 494-6.
- Aitken-Saavedra J, da Silva KD et al. Clinicopathologic and immunohistochemical characterization of 14 cases of angioleimyomasin oral cavity. Med Oral Patol Oral Cir Bucal. 2018: 23; e564-8.
- Sun L, Zhu Y, et al. Angioleiomyoma, a rare intracranial tumour – three case report and a literature review. World J Surg Oncol. 2014: 12; 216.
- Mehta PD, Desai N, et al. Angioleiomyoma of the lower lip. Ann Maxillofac Surg. 2020: 10(1); 251-253.
- Figure 1 Courtesy: science direct
- Figure 2 Courtesy: aoms.org.tw
- Figure 3 Courtesy: basic medical key
- Figure 4 Courtesy: pathology outlines
- Figure 5 Courtesy: dermnet.nz.com
- Figure 6 Courtesy: Wikipedia.com
- Figure 7 Courtesy: spandidospublications.com
- Figure 8 Courtesy: hindawi.com