
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
Pleomorphic rhabdomyosarcoma in adult: A very uncommon occipital location
Bouchra Dani*; Zahra Sayad; Malik Boulaadas
Department of Maxillofacial Surgery and Stomatology, IBN SINA University Hospital, Rabat, Morocco
*Corresponding Author : Bouchra Dani
Department of Maxillofacial Surgery and Stomatology,
IBN SINA University Hospital, Rabat, Morocco
Email: bouchradani89@gmail.com
Received : Jan 25, 2021
Accepted : Feb 18, 2021
Published : Feb 20, 2021
Archived : www.jcimcr.org
Copyright : © Dani B (2021).
Abstract
Rhabdomyosarcomeis a commun tumor in children with all its types (pleomorphic, embryonal,alveolarand spindle cell rhabdomyosarcoma). However, it is a very rare tumor in adults, the commun type isthe pleomorphicrhabdomyosarcoma but it is very rare in the head and neck region. The diagnosis of the pleomorphic RMS is made by the histopathologic study, this shows the interest of a biopsy before the surgicalprocedure. The treatment of patients with malignant mesenchymal tumors of the head and neck region is multidisciplinary (radical surgery with postoperative radiotherapy and or chemotherapy) with poor prognosis.
Keywords: Pleomorphic rhabdomyosarcoma, Adult, Occipital Region
Citation: Dani B, Sayad Z, Boulaadas M. Pleomorphic rhabdomyosarcoma in adult: A very uncommon occipital location. J Clin Images Med Case Rep. 2021; 2(1): 1013.
Background
Rhabdomyosarcomais one of the most common tumors of childhood and adolescence, (more than 50% of soft tissue sarcomas) [1]. However, it is a very rare tumor in adults (less than 3% of adult soft tissue sarcomas) [2]. There are four major categories of rhabdomyosarcoma, which include pleomorphic, embryonal, alveolar and spindle cell rhabdomyosarcoma [3]. The pleomorphic form is the most frequent in adults but the neck localisation is the rarest. To our knowledge, there are no previous case reports of adult pleomorphicrhabdomyosarcoma occurring in the occipital region in the literature. In this article we will report an uncommon case of pleomorphicrhabdomyosarcomaoccurring in the occipital region.
Case Report
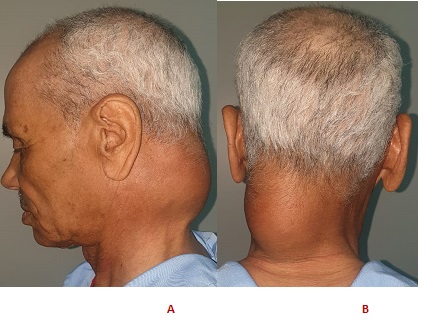
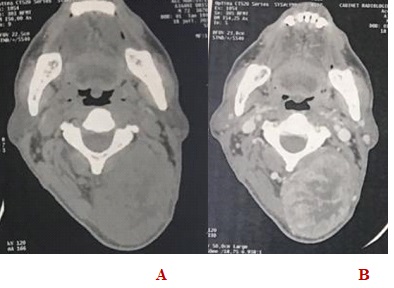
A 72-year-old male patient with no medical history of surgery or trauma, was referred to our department for a huge occipital mass evolving over 10 months and gradually increasing in volume (Figure 1). The clinical examination found an occipital swelling overflowing on the neck without any inflammatory signs in the skin, the tumorwasfirm on palpation, painless, welllimited, about 8 cm major axis. Examination of cervical lymph nodes showed no palpable lymphadenopathy. The rest of the maxillofacial, neurological and somaticexaminationwerewithoutparticularities. A cranio-facial CT scan, the presence of a left-sided, heterogeneous occipital tissue over flowing on the nucal region (Figure 2), containing areas of central necrosis, measuring 59 mm X 73 mm X 92 mm, that enhaced after contrast injection. The mass was interposed between the spinous muscle and the levators capulae muscle. The tumor does not infiltrate the skin from which it is separated by subcutaneous fat. The CT scan showed no lymphadenopathy associated.

Under general anesthesia, we started within tra-operative frozen section that showed pleomorphic cells with enlarged hyperchromaticnuclei and eosinophiliccytoplasm. The surgery was completed by a large excision of the tumor limited by the cervical spine.
A histopathological examination of the surgical specimen showed pleomorphiccells with enlarged hyperchromatic nuclei and eosinophilic cytoplasm. Immunohistochemical testing detected neoplastic cells expressing desmin, myogenin, CK AE1/AE 3, EMA, AML, H-caldesmone, CD 34, CD 31, KI67, and not expressing the HMB45, Melan A and the PS100 ; confirming the diagnosis of pléomorphic rhabdomyosarcoma.
Computerized tomography (CT) examinations of the abdomen and thorax revealed no metastases, and no lymphadenopathy was detected in the neck.
The follow-ups were simple, the patient underwent adjunctive chemotherapy to eradicate any residual tumours.
The oncologists decided to go for 20 sessions of chemotherapy that associeted ifosfamide, Mesna and Doxorubicin.
The patient has continued monthly follow-up visits and has remained disease-free for 1 years after the surgery.
Discussion
Rhabdomyosarcome is a commun tumor in children with all its types. About the opposite for adults where the head and neck sarcoma are presented only 1% of all head and neck cancers [4]. The commun type in adults is the pleomorphic rhabdomyosarcoma but it is very rare in the head and neck region. In addition, this tumor has a higher rate of recurrence and metastasis in adults [3]. The clinical presentation of the head and neck rhabdomyosarcoma depends on its location, the patients usually presents a rapidly growing, painlless, swelling [4,5]. The radiological examination that can be used to identify the extension of the tumor in this region are the cranio-facial CT scan or an MRI.
The diagnosis of the pleomorphic RMS is made by the histopathologic study, that usually shows a large, a typical pleomorphic tumor cells with abundant eosinophilic cytoplasm which can be irregular and hyperchromic, they also can have large or multiple nuclei. The diagnosis is confirmed by the immunohistochemical tests, the tumor cells express desmin, actin, myogenin, Myoglobin, Vimentin and MyoD1 [3,4,5].
Differential diagnosis of a head and neck mass should always be considered to avoid any misdiagnosis and mistreatment of the patients. Other malignant tumors with rhabdomyosarcomatous differentiation need to beconsidered on the differentialdiagnosis. Such as neuroblastoma, lymphoma, melanoma, fibrosarcoma, granular cellmyoblastoma, rhabdomyoma, Ewing’s sarcoma, chordocarcinoma and sarcomatoid carcinoma etc [4].
For our patient, the immunohistochemistry test confirmed the diagnosis by the presence of desmin, actin and myogenin, which are highly sensitive and specific markers for RMSs.
RMSs are locally aggressive and they can spread regionally, or distantly by both lymphatic and hematological routes. The commonest sites of metastatic spread are lung, liver, lymphnode and bone [6]. Therefore, during followup, Computerized tomography (CT) examinations of the abdomen and thorax are essential to searchany metastases or lymphadenopathy in the neck.
Several prognostic indicator are used to evaluate the prognosis of the RMS, which include, age, tumor location, size, histologic subtype, and the presence or absence of regional nodes or distant metastases [17,23]. The age seems to be the most important prognosis factor, studies showed that Children treated for RMS had a significantly better outcome than adults regardless the subtype of the RMS [6].
The treatment of patients with malignant mesenchymal tumors of the head and neck region is multidisciplinary and multimodal includes radical surgery with postoperative radiotherapy and or chemotherapy.
The surgical execison of the tumors should be radical to prevent any local reccurence. The analysis of the specimen and the assessment of the extent of the tumor allow to establish the stage of the tumor according to the Intergroup Rhabdomyosarcoma Study (IRS) [7].
Chemotherapy contributes to improved survival and reduced frequency of recurrence, also reduces the indications of extensive surgical excisions. It often associate Vincristine, Actinomycin, Cyclophosphamide, Ifosfamide, Doxorubicin.
Radiotherapy is also an integral part of the treatment. The irradiation targets the tumor and the lymphnodes. It is not systematic, it is used as adjuvant therapy for small volume residual disease after surgery [8].
However, in high-risk metastatic forms, the treatment approach can be more conservative, partial surgical excision or non surgical therapies such as chemotherapy and/or radiotherapy [8].
In our case, the clinical and radiological présentation of the tumor didn’t give us a diagnosis orientation. That is why we proceeded by an intra-operative frozen section that showed the présence of signs of malignancy. So we proceeded by the resection of the tumor with wide margins.
The histological test of the surgical specimen confirmed the diagnosis of pleomorphic rhabdomyosarcoma and the total excision of the tumor was performed. However, considering the malignancy, the metastatic potential of this tumor and the age of the patient, he was referred to the oncology center for a complement of chemotherapy.
References
- Sultan I, Qaddoumi I, Yaser S, Rodriguez-Galindo C, Ferrari A. Comparing adult and pediatric rhabdomyosarcoma in the surveillance, epidemiology and end results program, 1973 to 2005: an analysis of 2,600 patients. J Clin Oncol. 2009; 27(20): 3391-7.
- Fletcher CDM, Unni KK, Mertens F: WHO classification of tumours: pathology and genetics of tumours of soft tissue and bone. 3rd ed. Skeletal muscle tumors. Lyon: IARC Press. 2006; 141-154.
- Eleanor Chen, Robert Ricciotti, Neal Futran, Dolphine Oda. Head and neck rhabdomyosarcoma: Clinical and pathologic characterization of seven cases. Head and Neck Pathol. 2017; 11: 321-326.
- Zhou DN, Yang QQ, Li ZL, Pan ZY, Deng YF. Head and neck rhabdomyosarcoma: Follow-up results of four cases and review of the literature. Int J Clin Exp Pathol. 2015; 8(5): 4277-83.
- Furlong MA, Mentzel T, Fanburg-Smith JC. Pleomorphic rhabdomyosarcoma in adults: A clinicopathologic study of 38 cases with emphasis on morphologic variants and recent skeletal muscle-specific markers. Mod Pathol. 2001; 14(6): 595-603.
- B Pittore, G Fancello, P Cossu Rocca, G P Ledda and G Tore. Rhabdomyosarcoma: A rare laryngeal eneoplastic entity: A case report. Acta Otorhinolaryngologica Italica. 2010; 30: 52-57.
- Parham DM, Barr FG. Classification of rhabdomyosarcoma and its molecular basis. Adv Anat Pathol 2013; 20: 387-97.
- Sevdegül Mungan, Selçuk Arslan, Eda Küçüktülü, Fafak Ersöz, and Bengü ÇobanoLlu. Pleomorphic rhabdomyosarcoma arising from true vocal fold of larynx: Report of a rare case and literature review. Case Rep Otolaryngol. 2016; 2016: 81359-67.