
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
Cross-leg flap after posttraumatic osteomyelitis defect: A last resource for limb salvage
Eva Campos Pereira1*; Sara Diniz2; Filipe Rodrigues2; Alexandre Pereira2; Ricardo Sousa2#
1Orthopaedics Department, Hospital Central do Funchal, Funchal, Portugal.
2Orthopaedics Department, Centro Hospitalar e Universitário do Porto, Porto, Portugal.
*Corresponding Author : Eva Campos Pereira
Orthopaedics Department, Hospital Central do
Funchal, Funchal, Portugal.
Email: eva.campos.pereira@gmail.com
Received : Jan 26, 2021
Accepted : Feb 19, 2021
Published : Feb 22, 2021
Archived : www.jcimcr.org
Copyright : © Pereira EC (2021).
Abstract
We report the case of a patient with a tibial shaft fracture occurring through a chronic posttraumatic osteomyelitis site with significant soft tissue defect. The bone and soft tissue reconstruction procedures are described with a cross-leg fasciocutaneous flap performed as a last resource after previous rotated muscle flap partial failure. Pre-operative CT angiography, to rule outaxial vessel damage and peripherical vessel diseases, and adequate stabilization of both legs are key for a successful limb salvage.
Keywords: Osteomyelitis, Soft tissue defect, Muscle flap, Cross-leg flap.
Citation: Pereira EC, Diniz S, Rodrigues F, Pereira A, Sousa R. Cross-leg flap after posttraumatic osteomyelitis defect: A last resource for limb salvage. J Clin Images Med Case Rep. 2021; 2(1): 1014.
Background
Cross-leg flap is an ultimate flap option when other coverage solutions fail. It was formally described in 1854 by Hamilton and it had been successfully used in reconstruction of soft tissue defects of the lower limbs [1,2]. However, it has been outdated by the development of microsurgery techniques and skin substitutes [1,3]. Extensive traumatic defects may present a compromised circulatory system which make it impossible to perform microsurgical free flaps [2,4]. The authors describe the reconstructive techniques used to cover a posttraumatic osteomyelitis defect, which culminated with a cross-leg fasciocutaneous flap for definitive soft tissue coverage.
Case Presentation
A 78-year-old man with long standing type II diabetes mellitus entered our emergency room after a low-impact trauma with subsequent right tibial shaft fracture that occurred at the site of a chronic posttraumatic osteomyelitis. The patient had an history of high-energy trauma to his right leg with open fracture more than 30 years ago that was treated elsewhere and ultimately developed chronic posttraumatic osteomyelitis with significant bone exposure that had been treated conservatively for the past few years.
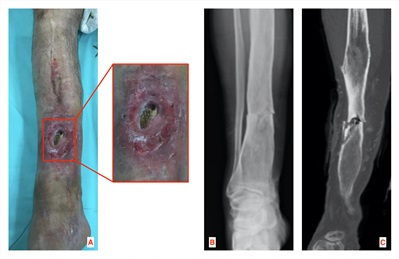
At initial observation he presented an antero-medial tibial cutaneous ulcer with bone exposure of his right leg (Figure 1A). The initial conventional radiographs and computerized tomography (CT) revealed a previously Cierny-Mader type III osteomyelitis that turned type IV by the pathologic fracture (Figure 1B-C). The patient was studied pre-operatively with an Angio-CT that revealed perfusion through all major leg arteries.
On his first surgery an aggressive debridement of all soft tissues anddead bone was performed (Figure 2A-B). Samples were sent for microbiology and absorbable antibiotic impregnated bone substitute - Cerament® (20 mL of vancomycin and 10 mL of gentamicin) - was used to manage dead space, provide local antibiotic(s) and bone support. External fixator was placed to stabilize the fracture in compression (Figure 2C). In the same surgical procedure, an inverted hemisoleus muscle flap and a rotated medial gastrocnemius muscle flap were harvested to cover cutaneous losses in the distal and proximal parts of the lower leg defect, respectively (Figure 2D). Post-operative conventional radiographs revealed good stabilization of the fracture and complete filling of the bone cavity with the bone substitute (Figure 2E-F). Broad-spectrum antibiotics (vancomycin and piperacillin/tazobactam) were started after surgery and subsequentially changed to a targeted antimicrobial therapy (piperacillin/tazobactam) after identification of Proteus mirabilis, Escherichia coli and Streptococcus dysgalactiae ssp equisimilis for a total six weeks duration. After two weeks, flaps were covered with partial-thickness skingraft from the homolateral thigh (Figure 3). Two weeks later (one month after original surgery) full depth necrosis of the flap in the distal part of the wound became evident.


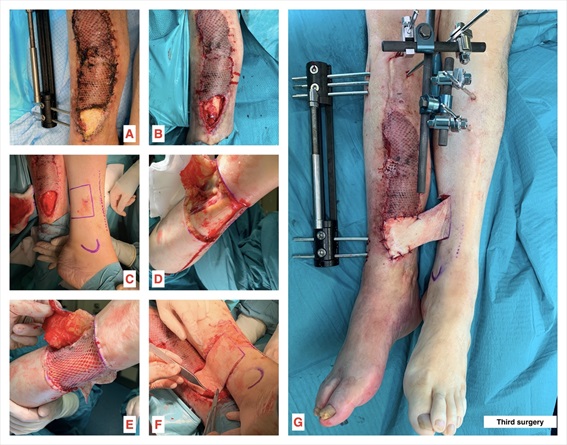
Six weeks after the first surgery, a new surgery was performed for debridement of the necrotic tissues resulting in a large circular defect (Figure 4A-B). Respecting the skin markings, planned according to the exposed area, a fasciocutaneous flap from the posteromedial part of the distal contralateral leg was done (Figure 4C-D). The donor site was covered with partial-thickness skingraft from the right thigh and the flap was partially sutured to the wound borders (Figure 4E-F). Both legs were stabilized together with a second external fixator (Figure 4G). Three weeks later, the cross-leg flap was separated from the donor site and the second external fixator removed.
Fourteen weeks after admission, patient was ultimately discharged home maintaining partial weight bearing walk with external fixator still on. External fixator was kept for eight months after progressive weight bearing, dynamization and radiographic signs of bone consolidation.
One year after his first surgery, conventional radiographs demonstrate a good consolidation of the tibial fracture and there are no signs of recurrent infection (Figure 5A-B). The patient walks autonomously, is painfree and satisfied with the cosmetic result (Figure 5C).

Conclusion
Coverage of extensive posttraumatic lower limbs defects can be challenging. The best wound closure must be considered accordingly the patient local conditions, always having as main goal the limb salvage [5]. Cross-leg flap, that has suffered some modification over the past decades, is an alternative option when other coverage techniques are not viable because of the unsuitable vessels [2,3]. A pre-operative CT angiography is important to rule outaxial vessel damage and peripherical vessel diseases. After running out two muscular rotated flaps options the authors opted to perform a fasciocutaneous cross-leg flap. A free muscle flap could be considered but the poor local conditions, the patient’s comorbidities and old age should prompt other simpler and most successful possibilities. A stable fixation of both legs is mandatory to avoid flap failure. Cross-leg flap does not require microsurgical skills and has the advantage of taking blood supply from the contralateral non-traumatized arterial system. The discomfort inherent to a three weeks period of both legs stabilized together was well tolerated by our patient, without any thromboembolic complication of the long immobilization period. Therefore, the authors recommend the cross-leg flap as good option when other coverage procedures cannot be considered.
References
- Shoeib MA. Cross-Leg Flap: Its Reliability and Outcome. Modern Plast Surg. 2013; 3: 9-14.
- Mahajan R, Srinivasan K, Ghildiyal H, et al. Review of Cross-Leg Flaps in Reconstruction of Posttraumatic Lower Extremity Wounds in a Microsurgical Unit. Indian J Plast Surg. 2019; 52: 117-124.
- Lu L, Liu A, Zhu L, et al. Cross-Leg Flaps: Our Preferred Alternative to Free Flaps in the Treatment of Complex Traumatic Lower Extremity Wounds. J Am Coll Surg. 2013; 217(3): 461-471.
- Contedini F, Negosanti L, Fabbri E, et al. Cross-Leg as a Salvage Procedure after Free Flaps Transfer Failure: A Case Report. Case Rep Orthop. 2012.
- Topalan M, Ermis I. Cross-Leg Free Flap for Emergency Extremity Salvage: Case Report. J ReconstrMicrosurg Open. 2001; 3(17): 157- 161.