
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
Urinoma: Saviour of beleaguered kidney
Manjeet Kumar1*; Mehar Chand2; Sanjeev Chauhan3 ; Sunil Kumar4; Kirti Rana3
1 Assistant Professor, Department of Urology, IGMC, Shimla HP, India.
2 Senior Resident, Department of Radiology, IGMC, Shimla, India.
3 Junior Resident, Department of Surgery, IGMC Shimla, HP, India.
4 Senior resident, Department of Urology, IGMC Shimla HP, India.
*Corresponding Author : Manjeet Kumar
Assistant Professor, Department of Urology, IGMC,
Shimla HP, India.
Email: manjeetkumar.1014@gmail.com
Received : Jan 30, 2021
Accepted : Feb 23, 2021
Published : Feb 25, 2021
Archived : www.jcimcr.org
Copyright : © Kumar M (2021).
Abstract
Introduction: Spontaneous extravasation of urine due to High Pressure Chronic Retention is a rare entity. Most cases of urinoma are secondary to ureteric calculi. We present a case of left spontaneous perinephric urinoma with right hydroureteronephrosis with high pressure chronic retentiondue to benign enlargement of prostate.
Summary: A 70 years male, with no comorbid illness, presented with left flank pain with overflow incontinence. On radiological evaluation, he was found to have distended urinary bladder, with right hydrouretronephrosis and left perinephric collection. Renal function tests were deranged. Patient was managed with per urethral catheter placement, antibiotics and ultrasound guided aspiration. Retention volume was more than one litre. Creatinine content of aspirated fluid was ten times higher to serum creatinine. Transurethral resection of prostate was done. The patient voided well after surgery. The urinoma resolved completely in 2 weeks. Follow up Contrast study revealed preserved left renal function; however the right hydroureteronephrotic kidney shrank in size.
Conclusion: Spontaneous perinephric urinoma formation due to High pressure chronic retention was a blessing in disguise for the patient. It saved the affected kidney from getting knocked out. The other side hydroureternephrotic kidney suffered anatomical and functional loss.
Keywords: Urinoma, Hydronephrosis, Bladder outlet obstruction
Citation: Kumar M, CHand M, Chauhan S, Kumar S, Rana K. Urinoma: Saviour of beleaguered kidney. J Clin Images Med Case Rep. 2021; 2(1): 1017.
Introduction
Spontaneous extravasation of urine is a rare entity. It comprises 0.08% - 1% of urograms. Most of the cases occur on unilateral side. Mostly it is self-limiting and resolves with conservative treatment [3]. It results when urine extravasation occurs from the urinary tract. This extravasation can occur from kidney, ureter, bladder, or urethra. Urinoma can unilateral or bilateral depending on etiology. It can be symptomatic or asymptomatic. It can present as an encapsulated collection or free fluid mimicking ascites [1].
In urinoma, there is urine collection in retroperitoneum, causing a local inflammatory reaction on perirenal fat. It leads to lipolysis causing encapsulation of urine which is called urinoma [2].
Case presentation
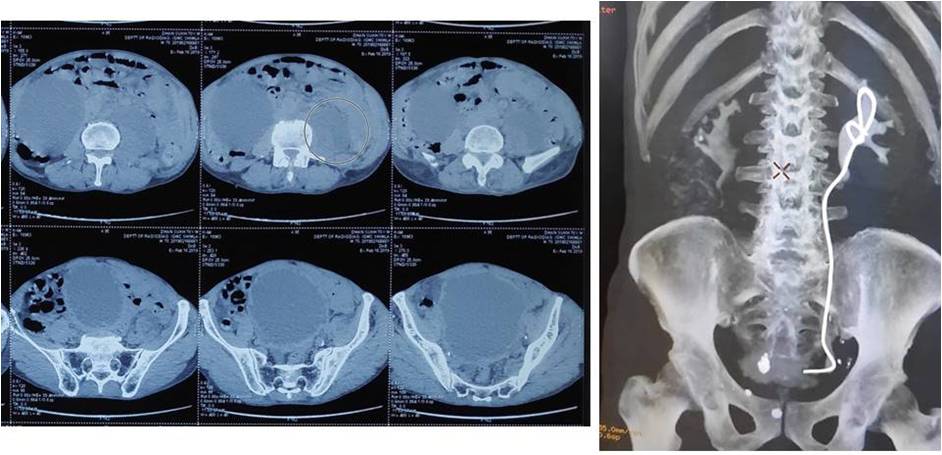
A 70 years male, with no comorbid illness, presented with left flank pain with overflow incontinence. On examination patient had palpable urinary bladder and tender left renal angle. On radiological evaluation, he was found to have distended urinary bladder, with right hydrouretronephrosis and left perinephric collection. Initial NCCT KUB suggests right hydronephrosis and hydroureter (12 X 5.7 cm Kidney size) till urinary bladder. Left Kidney measure 11 X 4.9 cm with mild hydronephrosis with perinephric collection 12 X 7 X 4.5 cm. The urinary bladder is over-distended and 5.5 mm thick.
Renal function tests were deranged (Urea 40/2.5 mg/dl). He was managed with per urethral catheter placement, antibiotics, left DJ stenting and ultrasound guided aspiration. Retention volume was more than one litre. Creatinine content of aspirated fluid was ten times higher to serum creatinine. He had decrease in creatinine (nadir 0.9 mg/dl) and resolution of perinephric collection. Cystoscopy showed grade II trabeculations and median lobe grade II with grade III lateral lobes. He was planned for transurethral resection of prostate. He voided well after surgery. Follow up Contrast study revealed preserved left renal function; however the right hydroureteronephrotic kidney shrank in size.




Discussion
Urinoma or spontaneous extravasation of urine is a rare condition caused by extravasation of from urinary tract. Clinically patients can be asymptomatic or symptomatic. The patient can present as an acute abdomen i.e.; flank pain decreased urine output or deranged renal function tests. However, in a patient with large urinoma and patients with symptoms of pain, fever, and urosepsis, urgent interventions are required. Treatment involves empiric antibiotic and drainage catheter placed into urinoma [2].
Causes of urinoma can be broadly divided into two categories:
Obstructive
Ureteric calculus
BPH
Post-radiation scarring
Retroperitoneal fibrosis
Pelvic abscess
Pregnancy
Non-obstructive Gynecological
External trauma to the urinary system
Genitourinary surgery
Pelvic
Retroperitoneal
Among all these, traumas is the most common cause [1].
Urine leak can occur between kidney and capsule, which is called subcapsular urinoma, and it can also occur between Gerota’s fascia and capsule. The most common urine leak occurs between the kidney and Gerota’s fascia. Mostly asymptomatic and symptoms consist of nausea, vomiting, flank pain, fever, ileus, etc. Evaluation of patient with suspected urinoma include, ultrasonography followed by NCCT KUB, NCCT is the gold standard. Management of urinoma is mostly conservative, but if the size of urinoma does not decrease, percutaneous catheter under ultrasound guide can be placed in urinoma. Urinoma, if diagnosed in time, can prove fatal, causing serious complications requiring immediate intervention. A complication of urinoma includes hydronephrosis, abscess formation, sepsis, and paralytic ileus [1].
Our patient had right hydronephrosis and left perinephric fluid collection i.e. urinoma secondary to overdistended urinary bladder as a result of prostatic obstruction. Right Kidney had thin parenchyma compared to left kidney at presentation. This was mainly as a result formation of left urinoma venting off increased pressure in left pelvicalyceal system. The release of urine from left renal pelvis leads to preservation of parenchyma as well leading to symptoms.
Conclusion
Spontaneous perinephric urinoma formation due to high pressure chronic retention was a blessing in disguise for the patient. It saved the affected kidney from getting knocked out. The other side hydroureternephrotic kidney suffered anatomical and functional loss.
References
- Gautam R, Shaikh T, Attarde N, Gupta S, Wani J, Ghosalkar M, Ansari S, Murali S. Urinoma: A rare complication of ureteral calculi. International Journal of Research in Medical Sciences, 2015; 3(9): 2440-2442.
- Goldwasser J, Wahdat R, Espinosa J, Lcerna A. Urinoma: Prompt Diagnosis and Treatment Can Prevent Abscess Formation, Hydronephrosis, and a Progressive Loss of Renal Function. A case report in Emergency Medicine. 2018.
- Pang H, Dang X, Yao Z, Feng X, Wu G. Bilateral spontaneous urinary extravasation shown by computed tomography urography in a patient with benign prostatic hyperplasia. Elsevier. 2015; 10(1): 53-55.