
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
Total thumb reconstruction by an original groin pocket flap-graft design
Elise Lupon, MD, MSc1,2*; Alexandre Gaston Lellouch, MD, MSc2,3; Paul Girard, MD, MSc4; Pierre Mansat, MD, PhD5; Jean Louis Grolleau, MD, PhD1; Jérôme Laloze, MD, MSc6,7; Samuel Riot, MD1
1 Department of Plastic surgery, University Toulouse III Paul Sabatier, HôpitalRangueil, Toulouse, France.
2 Vascularized Composite Allotransplantation Laboratory, Center for Transplantation Sciences, Massachusetts General Hospital, Harvard Medical School, Boston, MA, USA.
3 Department of Plastic Surgery, European George Pompidou Hospital, University of Paris, Paris, France.
4 Department of Plastic, Reconstructive and AestheticSurgery, Hospital Sud, University of Rennes 1, Rennes, France.
5Department of Orthopedic and Traumatologic surgery, University Toulouse III Paul Sabatier, Hospital Purpan, Toulouse, France.
6 Department of Faculties of Medicine and Pharmacy, University of Limoges, Myelin Maintenance and Peripheral Neuropathies (EA 6309), Limoges, France.
7 Department of Maxillo-Facial and Reconstructive Surgery and Stomatology, University Hospital Dupuytren, Limoges, France
*Corresponding Author : Lupon Elise
Department of Plastic surgery, University Toulouse III
Paul Sabatier, HôpitalRangueil, Toulouse, France.
Email: elupon@mgh.harvard.edu
Received : Feb 02, 2021
Accepted : Feb 26, 2021
Published : Mar 02, 2021
Archived : www.jcimcr.org
Copyright : © Elise L (2021).
Abstract
Background: The thumb plays a key role in hand function for precise dexterity. The surgical treatment of full avulsions of the digital skin sheath by tearing (ring syndrome) is complex and the management of these lesions is challenging for the reconstructive surgeon. When replantation is not possible, other alternatives are available if the covering tissue is thin and flexible.
Case presentation: A 30-year-old male, tobacco addict, had a thumbsequelae similar to a stage III ring finger. Revascularization attempt failed and the skin envelope necrosed secondarily. A groin pocket flapgraft allowed a conservation of his thumb with a satisfactory aesthetic and functional result.
Conclusions: We described a thumb coverage by a groin flapgraft using an original pocket design. This simple and safe procedure, in the carefully selected patient can successfully address functional and aesthetic concerns simultaneously, with minimal sequelae at the donor site. This technique can be used to treat a cutaneous tearing of the other fingers.
Keywords: Flap-graft, Thumb reconstruction, Ring-finger, Inguinal flap, Digital reconstruction, Digital cutaneous tearing
Citation: Lupon E, Lellouch AG, Girard P, Mansat P, Grolleau JL, et al. Total thumb reconstruction by an original groin pocket flap-graft design. J Clin Images Med Case Rep. 2021; 2(2): 1018.
Introduction
Hand traumatism may result in soft tissue defects, which cause functional loss [1]. The thumb is crucial in hand function. Daily activities such as holding, gripping, opposition, circumduction, and motions involving the manipulation of the hand are possible because of the unique anatomical properties of the thumb. Thus, damage to the thumb results in greater loss of function compared to the other fingers [2].
When thumb loss occurs due to trauma, replantation is the best method to restore full function. When replantation is not possible, thumb reconstruction using autologous tissue is necessary [3].
In addition, the surgical treatment of full avulsions of the digital skin sheath by tearing is complex and the long-term results are sometimes disappointing both aesthetically and functionally. The management of these lesions is challenging for the reconstructive surgeon.
Herein, we present a case report describing a thumb reconstruction by a groin flap-graftin a young man’s non-dominant hand, re-sensitized by a Litter-like procedure.
Case presentation
Patient and operative indication
A 30 years-old man was admitted in the emergency room (ER) for severe trauma of the first ray of his non-dominant left hand.
The patient is originally from India, a computer scientist, had no major past medical history. He is an active smoker. He had fallen while climbing a tree, and had skewered his thumb with a wooden branch.
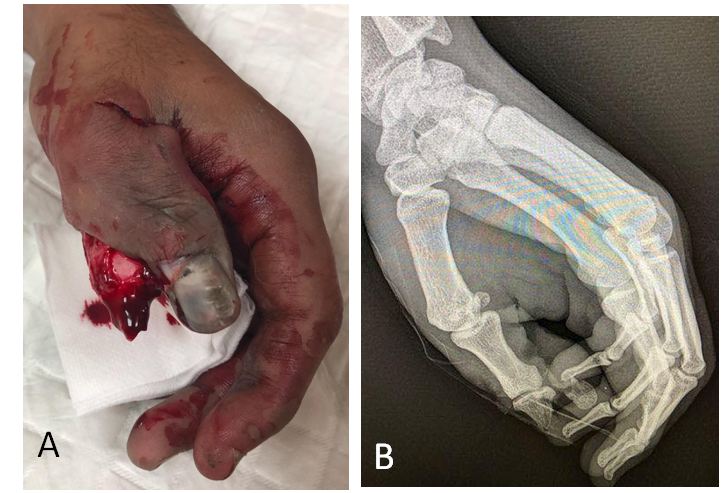
It had an appearance similar to a ring-finger stage III classification of the thumb (Figure 1). On clinical examination, the skin envelope of the thumb was complete. The X-ray showed a transverse diaphyseal fracture of the distal phalanx.
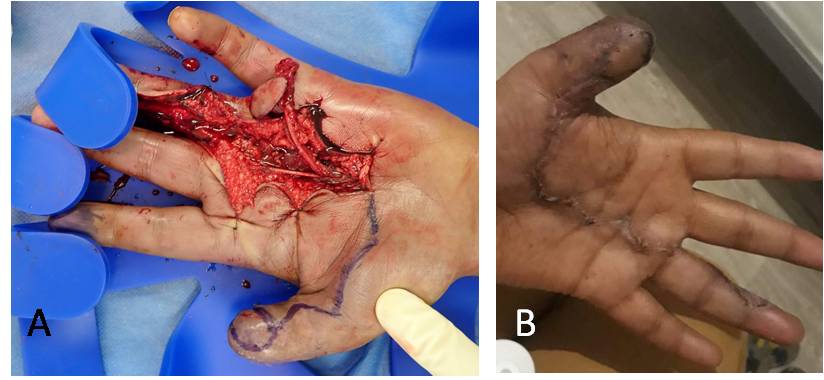
This patient, hemodynamically stable and with no other lesions, was rushed to the operating room. The arteries and collateral nerves were stripped, but the long thumb flexor tendon and the extensor tendon was intact. Osteosynthesis by interphalangeal broaching was performed and a revascularization with arterial bypass by venous grafting was attempted (Figure 2). Revascularization was initially successful butan arterial thrombosis with cutaneous necrosis complicated the procedure on post-operative day (POD) 3.

The different surgical alternatives for thumb reconstruction were discussed in the setting of an active smoker patient. We were looking for a reliable technique in terms of vascularization. Therefore, our team was not favorable to a microsurgery (free flap) technique. Thus, a reconstruction by free toes transfer was not considered as the best option for our patient and an attempt at reconstruction by a groin flap-graft was proposed and accepted by the patient. This technique was, according to us, the more reliable and functional option/alternative, in face of the impossibility of a free flap.
Surgical technique
The procedure was performed under general anesthesia. The patient is positioned supine on the operating table with both arms supported on arm boards, abducted to 90°. A pneumatic tourniquet was placed at the root of the limb.
The first step was the pre-operative drawing. A template for drawing the inguinal flap can be made using an operating sterile glove and allows determining the necessary skin coverage area. The design is adapted in a spindle, in order to facilitate skin closure.
Second step consists of a debridement of necrotic tissue. This step must be performed with the tourniquet deflated in order to evaluate properly viable tissues. A sterile glove used as a template allows, by drawing transparently over the area to be covered, to define the minimum skin area required. In our case, we needed to shorten the thumb.
Third step is to create subcutaneous pocket for the thumb introduction. This step is facilitated by the inflation of the pneumatic tourniquet, at 250 mmHG. The inguinal flap is harvested in a subdermal plane, with an upper hinge. The ends of the spindle are de-epidermized. The dermal pedicle flap, thus obtained, is plastered and sutured on itself in order to obtain a pocket for the area to be covered with the thumb. The finger is inserted into the pocket and the edge of the healthy skin edge on the thumb is sutured to the skin edges forming the open area of the pocket on the flap. At the end of this step, the patient’s upper limb is strictly immobilized for 3 weeks.
Once the theoretical vascular autonomy of the flap is restored, the last step is for the flap to be weaned. Superficial skin sloughing off is common. These damaged area must be removed sparingly.
Post-operative care and results
The patient was hospitalized for six weeks. Complete healing of the thumb and inguinal sampling site was achieved at 3 weeks (Figure 3). At 1 month post-operatively, the patient had found a solid thumb-index pinch movements and a Kapanji score at 9/10. The patient was very satisfied with the aesthetic result. Physiotherapy was started over the following week. At 12 weeks from weaning, a Littler’s like island heterodigital flap by transferring the radial collateral pedicle of the 4th ray, optimized thumb reconstruction by resensitizing the tip of the reconstructed thumb pulp. (Figure 4).

Discussion
The groin pocket flap-graft technique described here gives the surgeon an opportunity to achieve the coverage of the thumbexposed with the best aesthetic results.
The success of a digital reimplantation depends mainly on the mechanism of the traumatism. The tearing lesion with skin avulsion lead to a poor prognosis. This reconstruction takes all its importance for the 1st digitation, the thumb being a key element of the hand’s function. The technique chosen must allow the finger to be mobilized rapidly. The tissue used must therefore be fine and flexible. Reconstruction should allow sensitivity to be recovered, if possible.
Several surgical techniques for thumb reconstructionare possible. The main advantage of local flaps is that they provide tissue similar to avulsed tissue but make it possible to cover limited skin defect and their removal induces significant sequelae on adjacent fingers [4]. Locoregional flaps based on radial or ulna vessels are questionable when they require the sacrifice of one of the two major axes of hand vascularization. In addition, their removal imposes an unsightly scar on the forearm and skin thickness is generally greater and less suitable for distal thumb coverage [5].
We could have considered a partial toe transfer using the wraparound technique. However, the patient refuses the aesthetic morbidity of such a surgery. Otherwise, this smoker patient was at risk of vascular complications and these two reasons led us not to consider microsurgery as a first-line treatment. Indeed, aesthetic sequelae at the donor site and functional sequelae with pain type can be a reason for the patient to refuse this reconstruction [6].
The free flaps (temporal fascia flap, antero-lateral thigh flap and superficial circumplex iliac artery flap) were rejected because of the vascular risks associated with the patient’s active smoking. In addition, the free flaps would have given thick and not very functional reconstructions, except for the free fascia temporalis flap but which involves an additional grafting sequelae.
McGregor’s inguinal flap has a thickness not very suitable for finger reconstruction, with poor functional and aesthetic results for mobility [7].
The thumb cover by a groin flap-graft is a fast and simple procedure for patients with skin defect of the thumb.
The flap-graft technique, initially described by Colson, and taken at the inguinal region, is an interesting alternative because of its reliability and finesse. It is a flap degreased from the outset, fed by its pedicle, and later fed by its deep face in the manner of a graft [8]. Colson proposed a donor area located on the anterolateral side of the contralateral arm. Inguinal sampling reduces patient discomfort and scarring sequelae. We describe a technical variant in the modeling of this flap, which folds on itself, following a pre-operative drawing designed on the basis of a template. This allows a custom digital pocketing. The creation of this pocket, designed to contain the injured finger, allows an optimization of the final result in terms of fineness and adjustment of the flap on the surface to be covered. This technique is also possible to treat skin tears from other fingers [9].
We recommend this technique, when a toe transfer isn’t possible, in the mechanisms of skin avulsion because it gives very satisfactory results in a compliant patient. Aesthetically, it provides a thin and homogeneous thumb, as it would have been obtained with a total skin graft. However, it should be noted that the scars in this type IV Fitzpatrick patient, are dyschromic and have a hypertrophic tendency. Nevertheless, the recovery of an index-thumb clamp, which is functionally correct, is early after weaning.
This procedure must be completed by secondary surgeries. Indeed, the thumb plays a very important role in hand function, so it is important to take any kind of measure to restore the mobility, stability, length and sensory properties of the thumb after hand trauma. The Littler heterodigital neurovascular flap is a methodwhich can be used to achieve this purpose by flawlessly restores sensory function after a Colson flap-graft [10]. Our procedure was not the original Littler procedure as we didn’t use the ulnar pulp of the ring finger, innervated by the ulnar nerve, to re-sensitize a thumb that is why we called it “a Littler’s like island heterodigital flap”.
The main disadvantage of this technique is related to its constraining character related to the long period of immobilization. This can cause pain, maceration and stiffness. This makes it a surgery reserved for patients who are motivated by surgery and have understood it well. However, in a compliant patient surrounded by relatives, the immobilization time from flap making to flap weaning would probably be achievable at home, which would drastically reduce the length of hospitalization to a few days and improve the patient’s experience. On the other hand, a superficial suffering of this random flap is possible, requiring a compromise between the importance of degreasing the sampled flap, so therefore the thickness of the future thumb, and that of the correct vascularization of the flap. These controlled healing but can extend the recovery time. It should also be highlighted that this flap is not sensitive, in contrast to a free toe transfer. Finally, the flap may be a little dyschromic and keeps any hair from the donor area.
Conclusions
The groin pocket flap-graft is a good option in thumb reconstruction, as a first-line treatment for patients who refuse the morbidity of a toe transfer donor site or patient at high risk of microsurgical failure, or in areas where microsurgical methods are difficult to implement, in finger covers having undergone skin avusions in patients able of withstanding constraining immobilization. It allows an optimal aesthetic and functional result at the price of a very discreet scar at the donor site but requests a secondary sensitization procedure.
References
- Qin JZ, Wang PJ. Fingertip reconstruction with a flap based on the dorsal branch of the digital artery at the middle phalanx: A simple and reliable flap. Ann Plast Surg. 2012; 69(5): 526-8.
- Muzaffar AD, Chao JJ, Freidrich JB. Posttraumatic thumb reconstruction. Plast Reconstr Surg. 2005; 116(5): 103-22.
- Friedrich JB, Vedder NB. Thumb reconstruction. Clin Plast Surg. 2011; 38(4): 697-712.
- Martin DL, Kaplan IB, Kleinert JM. Use of a reverse cross-finger flap as a vascularized vein graft carrier in ring avulsion injuries. J Hand Surg. 1990; 15(1): 155-9.
- Noaman HH. Salvage of complete degloved digits with reversed vascularized pedicled forearm flap: A new technique. J Hand Surg 2012; 37(4): 832-6.
- Murphy AD, Tham SK. Second-toe wrap-around flap for reconstruction of a ring avulsion injury. J Hand Surg Eur Vol. 2017; 42(8): 857-858.
- Lister GD, McGregor IA, Jackson IT. The groin flap in hand injuries. Injury. 1973; 4(3): 229-39.
- Colson P, Houot R, Gangolphe M, de Mourgues A, Laurent J, Biron G, et al. Use of thinned flaps (flap-grafts) in reparative hand surgery. Ann Chir Plast. 1967; 12(4): 298-310.
- Dast S, Dessena L, Assaf N, David E, Herlin C, Sinna R. Reconstruction d’un arrachement digital par lambeau-greffe de Colson [Ring finger reconstruction by Colson’s flap]. Ann Chir Plast Esthet. 2017; 62(1): 104-108.
- Adani R, Squarzina PB, Castagnetti C, Lagana A, Pancaldi G, Caroli A. A comparative study of the heterodigital neurovascular island flap in thumb reconstruction, with and without nerve reconnection. J Hand Surg Br. 1994; 19(5): 552-9.