
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
Successfully stented aortoiliac occlusive disease that has multi-level crossing channels in occluded terminal aorta
Hiroaki Yamamoto, MD*; Minato Hayashi, MD; Ryosuke Sakaguchi, MD; Chieko Itamoto, MD; Tsunesuke Kohno, MD
Department of Cardiology, Nagano Chuo Hospital, Japan
*Corresponding Author : Hiroaki Yamamoto, MD
Department of Cardiology, Nagano Chuo Hospital,
Japan.
Email: h-yamamoto@healthcoop-nagano.or.jp
Received : Feb 11, 2021
Accepted : Mar 08, 2021
Published : Mar 10, 2021
Archived : www.jcimcr.org
Copyright : © Yamamoto H (2021).
Abstract
Aortoiliac occlusive disease (AOID) usually occurs as atherothrombotic stenosis or occlusion extending from the terminal aorta to the level of bilateral common iliac arteries. We experienced a young male case who had a history of five years of claudication with a tiny toe ulcer. The angiogram showed severely stenotic terminal aorta with two intraplaque collaterals in a multilevel crossing fashion that runs horizontally and vertically. With the careful endovascular procedure, we successfully implanted two stents in the lesion. As there are few reports that described such interesting channels, we presented the case in this article.
Keywords: Aortoiliac occlusive disease, Multilevel crossing channel, Endovascular treatment
Citation: Yamamoto H, Hayashi M, Sakaguchi R, Itamoto C, Kohno T. Successfully stented aortoiliac occlusive disease that has multi-level crossing channels in occluded terminal aorta. J Clin Images Med Case Rep. 2021; 2(2): 1022.
Introduction
Aortoiliac occlusive disease(AOID) usually occurs as atherothrombotic stenosis or occlusion extending from the terminal aorta to the level of bilateral common iliac arteries. Anatomies of AIOD are widely variables depending on the extent of the atherothrombotic burden and collateral channels that come from internal thoracic arteries, lumbar arteries and internal iliac arteries. We experienced a young male case that had very interesting and challenging intraplaque channels that were treated by endovascular treatment.
Case presentation
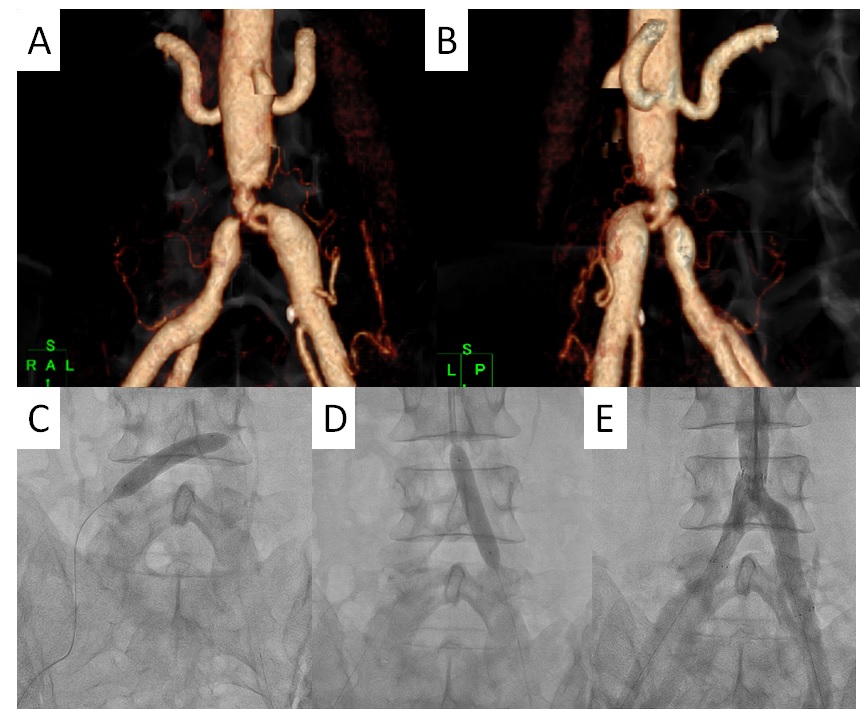
We present the case of a 45-year-old man. His risk factor was only smoking. Approximately 5 years ago, he began experiencing intermittent claudication that gradually worsened to rest pain in the left leg. One week before admission, he noticed a painful small ulcer on his big toe and came to our hospital. The ankle-brachial index was 0.80 on both the right and left. Computed tomography (CT) performed at the initial visit revealed that the terminal aorta was tapered and almost occluded; however, after careful review of the CT image, the right common iliac artery (CIA) was connected to the left CIA with a small channel located anteriorly, and the aorta was connected to left CIA with a small channel posteriorly (Figure 1a,b). The former channel ran horizontally, whereas the latter ran almost perpendicularly, like a multi-level crossing. However, the aorta and right CIA were not connected.
We intended to perform double-barrel stent implantation at the terminal aorta. We inserted a sheath into the right femoral artery and a long sheath from the left brachial artery to the aorta. GW easily passed from the right CIA to the left CIA via the true lumen. It was difficult to pass GW from the right CIA to the aorta even with hard GW. Therefore, we initially opened the right to left CIA-horizontal channel with a 2 mm balloon graduated up to 8 mm balloon (Figure 1c). Then we tried to again pass GW from the right CIA to the aorta, but it failed. Therefore, we crossed GW from the aorta to the left CIA and opened the perpendicular channel initially with 2 mm balloon graduated up to 8 mm, making cracks on the aorta-right CIA-total occlusion site (Figure 1d ), after which we were able to pass GW from the aorta to the right CIA. We placed a Zilver518 8/40 mm stent on the right CIA and a Zilver518 10/60 mm stent on the left CIA. We finished the procedure as initially planned (Figure 1).
Discussion
Occluded aortoiliac arteries are occasionally recanalized into intra-arterial channels; however, the number of channels is usually one [1]. Our patient had multi-crossing channels in the terminal aorta. One hypothesis that explains how such complex channels were created is that firstly, plaque deposition at the terminal aorta occluded right CIA remaining small channel to left CIA, then oxygen demand made perforating channel from left to right CIA by mechanical force and chemical mechanism such as thrombolytic reaction. Many aortoiliac occlusive disease cases are nowadays safely treated by endovascular treatment [2]. A technically important point is how to dilate the channels that show this special configuration of horizontal and vertical directions.With careful procedures, it was a safe and effective strategy to dilatesuchhorizontally running small channels with the preparation ofthe use of covered balloon-expandable stents [3].
Conclusion
Aortoiliac occlusive disease that has multi-level crossing channels in the terminal aorta was safely stented even that run horizontally from right to left common iliac arteries.
References
- Takigawa M, Akutsu K, Kasai S, Tamori Y, Yoshimuta T, Higashi M, et al. Angiographic documentation of aortoiliac occlusion in Leriche’s syndrome. Can J Cardiol. 2008; 24: 568.
- Neisen MJ. Endovascular management of aortoiliac occlusive disease. Semin Intervent Radiol. 2009; 26: 296-302
- Mwipatayi BP, Ouril K, Anwari T, Wong J, Ducasse E, Panneton JM, de Vries JPM, Dave R. A systematic review of covered balloonexpandable stents for treating aortoiliac occlusive disease. J Vasc Surg. 2020; 72: 1473-86.