
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
Abdominal emergency - Acute promyelocytic leukaemia presenting as a corpus luteal cyst
Brinderjeet Kaur*; S Fayyaz
Department of Obstetrics and Gynecology, Santokba Durlabhji Memorial Hospital and Research Center, Jaipur, India.
*Corresponding Author : Brinderjeet Kaur
Department of Obstetrics and Gynecology, Santokba
Durlabhji Memorial Hospital and Research Center,
Jaipur, India.
Email: dr.bjkaur@gmail.com
Received : Feb 04, 2021
Accepted : Mar 12, 2021
Published : Mar 16, 2021
Archived : www.jcimcr.org
Copyright : © Kaur B (2021).
Abstract
Acute promyelocytic leukaemia (APML) is known to present with disseminated intravascular coagulopathy (DIC) but as a Corpus luteal cyst hemorrhage however, it is rarely seen at presentation. This case is the first to describe a patient with APML who presented with ruptured corpus luteum without ovarian tissue infiltration with blasts, leading to hemoperitoneum posing as life threatening acute abdominal emergency in a woman belonging to child bearing age. The case is a singular case where APL has presented in such a rare manner.
Keywords: Corpus luteal cyst hemorrhage, Acute abdomen, Leukemia.
Citation: Kaur B, Fayyaz S. Abdominal emergency - Acute promyelocytic leukaemia presenting as a corpus luteal cyst. J Clin Images Med Case Rep. 2021; 2(2): 1027.
Short report
Acute promyelocytic leukaemia (APL) is known to present with disseminated intravascular coagulopathy (DIC) but as a Corpus luteal cyst hemorrhage however, it is rarely seen at presentation. [1]. A 27 year old female patient was admitted to the hospital with complaints of dizziness, palpitations as an acute abdominal emergency with unstable vitals (Blood pressure 90/58 mm of Hg, pulse rate 128/minute and a febrile). The initial investigations showed hemoglobin level of 8.1 g/dl, total leucocytes count 65,390/mm3 , with Blasts+ Promyelocytes- 61%, Myelocytes-12%, Metamyelocytes-11%, Neutrophils- 08%, Lymphocytes-06%, Monocytes-02% and platelet count- 30,000/mm3 . Prothrombin time (PT) was 20.2 seconds and INR-1.75. The peripheral blood smear examination was suggestive of acute leukemia (Promyelocytic) and was confirmed on flow cytometry.
The leukemic infiltration of female genital tract was earliest reported in 1933 by Mc Donald and Waugh [2]. Leukemias presenting as spontaneous hemoperitoneum is a rare event and generally involves leukemic cell infiltration of female genital tract [3]. There are few case reports where Acute lymphoblastic leukemia (ALL), Chronic myelogenous leukemia (CML) and other lymphomas have involved female genital tract but there is paucity of literature pertaining to leukemia result in corpus luteal cyst rupture leading to hemoperitoneum without histopathological involvement of female genital tract with leukemic blast cells [4,5]. Our case is a rarest of rare event where APL has presented as bleeding corpus luteal and bleeding ovary.
Corpus luteum cyst is the designation used for a cystic corpus luteum that is more than 3 cm in diameter. Corpus luteum is a thick walled cystic structure that is prone to internal hemorrhage and sometimes with intra abdominal hemorrhage. Occasionally these follicles may bleed into ovary causing cortical stretching, pain, rupture and rarely hemoperitoneum.
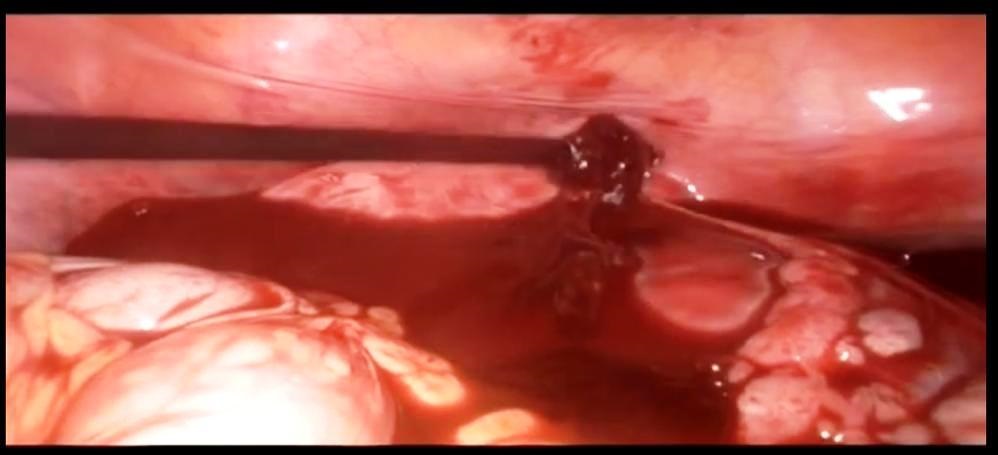
The patient presenting with acute abdominal pain and unstable vitals, she was administered 2 units of Packed red cell (PRC), one single donor platelet (SDP) and 1 Fresh frozen plasma (FFP) prior to diagnostic laproscopy which revealed ovary as source of bleed harboring hemorrhagic corpus luteum cyst which was managed by unilateral oopherectomy and tubectomy. The hemoorhagic corpus leuteal cyst is shown in the figures 1 to 3.
This case is the first to describe a patient with APML who presented with ruptured corpus luteum, leading to hemoperitoneum posing as life threatening acute abdominal emergency in a woman belonging to child bearing age.


References
- Habek D, Cerkez Habek J, Galic J, Goll-Barie S. Acute abdomen as a first symptom of acute leukemia. Arch Gynecol Obstet 2004; 270: 122–3.
- Cepicky P, Feyereislova A. Hemoperitoneum due to rupture of an ovarian endometrioid cyst as a first symptom of acute leukemia. Acta Clin Belg. 1991; 46: 28–9.
- Padmanabhan V, Shahin MM, Abdallah K. Chronic myeloid leukaemia manifesting as a gynecological emergency in a young woman. Int J Reprod Contracept Obstet Gynecol. 2017; 6: 3655-6.
- Chaudhary V, Sachdeva P, Karanth P, Arora R. Spontaneous hemoperitoneum in chronic myeloid leukemia: An unusual etiology. J Hematol. 2013; 2(1): 40-1.
- Successful management of a ruptured endometrial cyst in acute leukemia Taguchi, Ayumi et al. Fertility and Sterility. 95(1): 292; e1 - 292.e3.