
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
A COVID-19 extensive bilateral pneumonia, variants ischemic heart disease, and Movable-weaning phenomenon of hypocalcemia or Yasser’s phenomenon; dramatic reversal at home management
Yasser Mohammed Hassanain Elsayed
Critical Care Unit, Fraskour Central Hospital, Damietta Health Affairs, Egyptian Ministry of Health (MOH), Damietta, Egypt.
*Corresponding Author : Elsayed YMH
Critical Care Unit, Fraskour Central Hospital, Damietta
Health Affairs, Egyptian Ministry of Health (MOH),
Damietta, Egypt.
Email: dryaser24@yahoo.com
Received : Feb 11, 2021
Accepted : Mar 26, 2021
Published : Mar 28, 2021
Archived : www.jcimcr.org
Copyright : © Elsayed YMH (2021).
Abstract
Rationale: A COVID-19 is a recently infectious pandemic disease caused by a newly detected coronavirus. It is mostly presented with mild, moderate, or severe pneumonia. Interestingly, the presentation of COVID-19 infection with a newly ischemic heart disease have a risk impact on both morbidity and mortality of COVID-19 patients. The Movable-weaning phenomenon or Yasser’s phenomenon is a novel electrocardiographic phenomenon in hypocalcemia. Movable-weaning off an electrocardiographic phenomenon is a guide for both Wavy triple or double electrocardiographic signs. Patient concerns: An elderly female COVID-19 patient presented to physician outpatient clinic with extensive bilateral pneumonia and evidence of ischemic heart disease and Movable-weaning phenomenon of hypocalcemia (Yasser’s phenomenon). Diagnosis: COVID-19 pneumonia with variants ischemic heart disease and the Movable phenomenon of hypocalcemia or Yasser’s phenomenon. Interventions: Electrocardiography, chest CT scan, echocardiography, and oxygenation. Outcomes: Gradual dramatic clinical, electrocardiographic, and radiological improvement had happened. Lessons: It signifies the role of the anti-infective drugs, anticoagulants, antiplatelet, and steroids in COVID-19 with extensive pneumonia and ischemic heart disease patients are effective therapies. The presence of variant types of electrocardiographic ST-segment depressions in a COVID-19 patient is an indicator for severe specific ischemic myocardial insult. The dramatic reversal of variant types in ST-segment depressions in ECG may be interpreted as a coronary artery spasm. The presence of changeable Wavy triple ECG sign as a hallmark for the existence of the Movable-weaning phenomenon of hypocalcemia is recommended for further wide-study.
Keywords: COVID-19, Coronavirus, Extensive bilateral pneumonia, Movable-weaning off an electrocardiographic phenomenon, Yasser’s phenomenon, Wavy triple electrocardiographic sign At home distinct management.
Citation: Elsayed YMH. A COVID-19 extensive bilateral pneumonia, variants ischemic heart disease, and Movable-weaning phenomenon of hypocalcemia or Yasser’s phenomenon; dramatic reversal at home management. J Clin Images Med Case Rep. 2021; 2(2): 1035.
Introduction
The initial reports of a novel Coronavirus-2 (COVID-19) that is causing severe acute respiratory syndrome had emerged from Wuhan, China in December 2019 [1]. The clinical presentations of COVID-19 infection are highly variable which ranging from asymptomatic carrier to respiratory failure and acute respiratory distress syndrome (ARDS) [2,3]. An unusually high prevalence of hypercoagulability and pulmonary embolism has become prominent [4]. The cardiovascular system is widely influenced by severe acute respiratory syndrome (SARS) COVID-19 infection. The suggested mechanisms for COVID-19 sequels are either by a direct viral infection and indirect injury due to inflammation, endothelial stimulation, and microvascular thrombosis. The main pathophysiology underlying cardiovascular injury is the interaction between virus binding to the angiotensin-converting enzyme-2 receptors and the impact this action has on the renin-angiotensin system (RAAS), the body’s innate immune response, and the vascular response to cytokine production [5]. The most common clear cause of ST-segment depression (STD) is ischemic heart disease (IHD). ST-segment depression can be either up-sloping, down-sloping, or horizontal. Horizontal or down-sloping ST-segment depression ≥ 0.5 mm at the J-point in ≥2 contiguous leads is a signal for IHD. Up-sloping ST-segment depression in the precordial leads with prominent De-Winter sign is highly specific for obstructed anterior descending artery (LAD). ST-segment depression due to nonST-segment elevation ischemia is usually happening in a variable number of leads and with variable morphology [6,7]. However, STD that is occurring by IHD is mostly diffuse. It may be located in both anterior and inferior leads but unnecessarily localizing [7]. Wide-spectral opinions in cardiac stress testing reveal that the actual configuration of the STD affects the specificity of this abnormality but with a down-sloping STD segment more specific for the diagnosis of IHD than horizontal STD depression [7,8]. A depressed but up-sloping ST-segment carries low specificity for IHD [7]. The Movable-weaning phenomenon or Yasser’s phenomenon is a novel ECG phenomenon in hypocalcemia [9]. Movableweaning off an ECG phenomenon is a guide for both Wavy triple or double electrocardiographic signs [9,10].
Case description
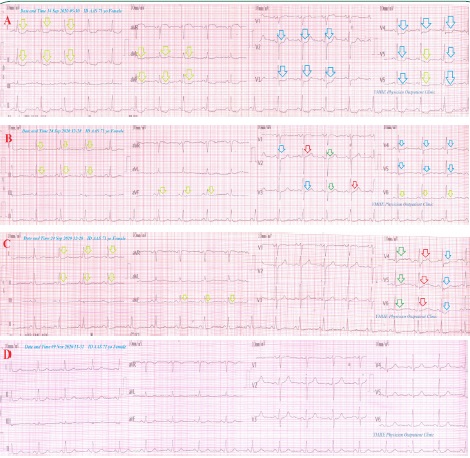
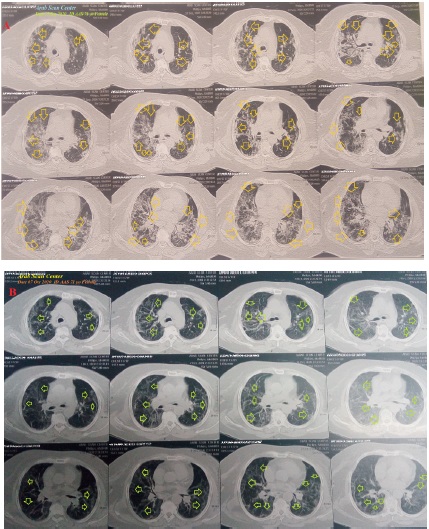
A 71-year-old married housewife Egyptian female patient presented to the physician outpatient clinic (POC) with acute tachypnea, fever, and dry cough. Fatigue, loss of appetite, and generalized body pain were accompanied symptoms. She gave a history of fever for 7 days. Recently, she had a history of contact with a neighbor who confirmed a COVID-19 patient in the past 10 days. Upon general physical examination; generally, the patient was tachypneic, distressed, with a regular pulse rate of 83 bpm, blood pressure (BP) of 90/70 mmHg, respiratory rate of 44 bpm, the temperature of 39.2°C, and pulse oximeter of oxygen (O2 ) saturation of 89%. She showed moderate obesity. No more relevant clinical data were noted during the clinical examination. She had managed at home as COVID-19 pneumonia with IHD and electro cardiographic Movable-weaning phenomenon of hypocalcemia (Yasser’s phenomenon). Initially, the patient was treated with O2 inhalation by O2 cylinder (100%, by nasal cannula, 5 L/min). The patient was maintain treated with cefotaxime; (1000 mg IV every 8 hours), azithromycin (500 mg PO single daily dose), oseltamivir (75 mg PO twice daily only for 5 days), and paracetamol (500 mg IV every 8 hours as needed). SC enoxaparin 80 mg twice daily), aspirin tablet (75 mg, once daily), clopidogrel tablet (75 mg, once daily), and hydrocortisone sodium succinate (100 mg IV every 8 hours) were added. The patient was daily monitored for temperature, pulse, blood pressure, and O2 saturation. The initial ECG on presentation showing normal sinus rhythm (of VR of 83) with down-sloping ST-segment depressions in inferior leads (II and aVF), in anterior leads (I and AVL), horizontal ST-segment depressions in V2-4, leads, and mixed ST-segment depressions in V5 and V6 (Figure 1A). The initial complete blood count (CBC); Hb was 10 g/dl, RBCs; 3.3*103/mm3 , WBCs; 14*103/mm3 (Neutrophils; 60%, Lymphocytes: 35%, Monocytes; 3%, Eosinophils; 2% and Basophils 0%), Platelets; 380*103/mm3 . S. Ferritin was high; 230.3 ng/ ml. D-dimer was high (2100 ng/ml). CRP was high; 96 g/dl. LDH was high; 228 U/L. SGPT was high; 75 U/L, SGOT was high; 53 U/L. Serum creatinine showed mild elevation; 1.5 mg/dl and blood urea; showed mild elevation; 54 mg/dl was high. RBS was; 214 mg/dl. Ionized calcium was mildly low; 0.65 mmol/L. The troponin test was positive. After 24 days of management; RBS was normal; 102 mg/dl. CBC; Hb was 10.3 g/dl, RBCs; 3.6*103 /mm3 , WBCs; 6.8*103 /mm3 (Neutrophils; 60 %, Lymphocytes: 34%, Monocytes; 4%, Eosinophils; 2% and Basophils 0%), Platelets; 280*103 /mm3 . S. ferritin was normal; 98.4 ng/ml. D-dimer was normal (160 ng/ ml). CRP was negative (˂6 g/dl). LDH was still high; 542 U/L. SGPT was normal; 41 U/L, SGOT was normal; 32 U/L. Serum creatinine; 1.1 mg/dl and blood urea ; 33 mg/dl were normal. Ionized calcium was normal; 1.01 mmol/L. The troponin test had become negative. The first chest CT scan was done on presentation showing extensive bilateral ground-glass pulmonary consolidations (Figure 2A). Serial ECG tracings were done. ECG tracing was taken within 14 days of treatment showing down-sloping ST-segment depressions in inferior leads (II and aVF), and in anterior leads (I and 6) and horizontal ST-segment depressions in V4 and V5 leads with normal sinus rhythm (NSR of VR of 83) There is a Wavy triple sign of hypocalcemia or Yasser’s sign-in V2 and V3 leads (Figure 1B). ECG tracing was taken within the same minute of the previous tracing and after 14 days of treatment showing down-sloping ST-segment depressions in inferior leads (II and aVF), and in only anterior aVL lead (NSR of VR of 82). There was a Wavy triple sign of hypocalcemia or Yasser’s sign-in V4-6 leads (Figure 1C). The last chest CT scan was done within 25 days of the presentation showing nearly dramatic healing of the above ground-glass consolidations but with still remnants of vague and reticular opacities (Figure 2B). Echocardiography showed no detected abnormality. A COVID-19 extensive bilateral pneumonia, variants ischemic heart disease, and the Movable-weaning phenomenon of hypocalcemia (Yasser’s phenomenon) was the most probable diagnosis. ECG tracing was taken within 35 days of the presentation showing normalization of above ST-segment depressions and Wavy triple sign with NSR of VR 73 (Figure 1D). Within 24 days of the above management, the patient finally showed nearly complete clinical, radiological, and laboratory improvement. The patient was continued on aspirin tablet (75 mg, once daily) and Oral calcium and vitamin-D preparation for 30 days with further recommended cardiac and chest follow up.
Discussion
• Overview
• An elderly female COVID-19 patient presented to physician outpatient clinic (POC) with extensive bilateral pneumonia and evidence IHD with superadded Movable-weaning ECG phenomenon of hypocalcemia (Yasser’s phenomenon).
• The objective primary for my case study was the presence of COVID-19 pneumonia and evidence of IHD with superadded Movable-weaning ECG phenomenon of hypocalcemia in POC.
• The secondary objective for my case study was the question of; How did you manage the case?
• There was a history of direct contact to confirmed the COVID-19 case.
• The presence of direct contact to confirmed the COVID19 case, and extensive bilateral ground-glass consolidation on top of acute tachypnea, fever, and dry cough will strengthen the COVID-19 diagnosis.
• The tachypnea, hypoxia, consolidation, and elevated ddimer are highly suggestive of associated pulmonary embolism.
• An associated marked elevated d-dimer, IHD, and hypocalcemia in the COVID-19 case presentation may carry a bad prognostic outcome and is indicating a high-risk condition.
• There were down-sloping ST-segment depressions, horizontal ST-segment depressions, and mixed ST-segment depressions.
• The presence of variant types in ST-segment depressions in ECG may be interpreted as accompanied by severe specific ischemic myocardial insult.
• The dramatic reversal of variant types in ST-segment depressions in ECG may be interpreted as a coronary artery spasm. Hypoxia and suspected pulmonary embolism were possible mechanisms.
• The presence of normal heart rate despite fever was interesting but there was an unknown clear etiology. The patient had evidence of both ischemic myocardial insult being physically fit that was suggested. Among healthy people, a slow heart rate may be due to being physically fit, drugs e.g., propranolol, sleep, IHD, sick sinus syndrome (SSS), certain infections e.g., Lyme disease or typhoid fever, hyperkalemia, and hypothyroidism [11].
• The presence of changeable Wavy triple electrocardiographic sign from ECG V1-2 leads to V4-6 leads is a hallmark for the existence of the Movable-weaning phenomenon of hypocalcemia. Tachypnea was a possible cause of hypocalcemia and subsequent Wavy triple electrocardiographic and Movable-weaning phenomenon of hypocalcemia [9,10].
• A nearly complete clinical, radiological, and laboratory improvement that occurred after the management with anti-infective drugs, anticoagulants, steroids, and antiplatelet strongly implies their effects.
• The normal lymphocytic count does not exclude COVID19 infection. But it carries a good prognosis.
• Blood pressure, respiratory rate, pulse, and O2 saturation are a strong guide for clinical follow-up in COVID-19 patients.
• A gradual decreasing the level of elevated CRP, d-dimer, and s. ferritin may be used as another good laboratory guide for follow-up for COVID-19 pneumonic patients.
• The serial change of radiological changes from normal chest CT to abnormal to normal at the end will strengthen the effectiveness of used drugs in this management.
• I can’t compare the current case with similar conditions. There are no similar or known cases with the same management for near comparison.
• The only limitation of the current study was the unavailable coronary angiography.
Conclusion and recommendations
• It signifies the role of the anti-infective drugs, anticoagulants, antiplatelet, and steroids in COVID-19 patients with extensive pneumonia and ischemic heart disease patients are effective therapies.
• The presence of variant types of ECG ST-segment depressions in a COVID-19 patient may be interpreted as a severe specific ischemic myocardial insult. The dramatic reversal of variant types in ST-segment depressions in ECG may be interpreted as a coronary artery spasm.
• The presence of changeable Wavy triple ECG sign as a hallmark for the existence of the Movable-weaning phenomenon of hypocalcemia is recommended for further wide-study.
Conflicts of interest: There are no conflicts of interest.
Acknowledgment: I wish to thanks my wife to save time and improving the conditions for helping me.
References
- Zhu N, Zhang D, Wang W, et al. A novel coronavirus from patients with pneumonia in China. 2019. N Engl J Med. 2020; 382: 727-33.
- Guan W-jie, Ni Z-yi, Hu Y, et al. Clinical characteristics of coronavirus disease 2019 in China. N Engl J Med Overseas Ed. 2020; 382: 1708- 20.
- Yang X, Yu Y, Xu J, et al. Clinical course and outcomes of critically ill patients with SARS-CoV-2 pneumonia in Wuhan, China: A singlecentered, retrospective, observational study. Lancet Respir Med. 2020; 8: 475–81.
- Middeldorp S, Coppens M, van Haaps TF, et al. Incidence of venous thromboembolism in hospitalized patients with COVID-19. J Thromb Haemost. 2020.
- Giustino G, Pinney SP, Lala A, Reddy VY, Johnston-Cox HA, Mechanick JI, Halperin JL, Fuster V. Coronavirus and Cardiovascular Disease, Myocardial Injury, and Arrhythmia: JACC Focus Seminar. J Am Coll Cardiol. 2020; 76(17): 2011-2023.
- Burns Ed. The ST Segment. Available online: https://litfl.com/stsegment-ecg-library/ (Accessed: Feb 4, 2021).
- Pollehn T, Brady WJ, Perron AD, Morris F. The electrocardiographic differential diagnosis of ST segment depression. Emerg Med J. 2002; 19(2): 129-35.
- Goldschlager N, Selzer A, Cohn K. Treadmill stress tests as indicators of presence and severity of coronary artery disease. Ann Intern Med. 1976; 85(3): 277-86.
- Elsayed YMH. Movable-Weaning off an Electrocardiographic Phenomenon in Hypocalcemia (Changeable Phenomenon or Yasser’s Phenomenon of Hypocalcemia)-RetrospectiveObservational Study. CPQ Medicine. 2021; 11(1): 01-35.
- Elsayed YMH. Wavy Triple an Electrocardiographic Sign (Yasser Sign) in Hypocalcemia. A Novel Diagnostic Sign; Retrospective Observational Study. EC Emergency Medicine and Critical Care (ECEC). 2019; 3(2): 1-2.
- Shmerling RH. How’s your heart rate and why it matters? Available online: https://www.health.harvard.edu/heart-health/hows-yourheart-rate-and-why-it-matters (Accessed: March 25, 2020).