
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
A benign rare intraabdominal lesion: Primary giant mesenteric hydatid cyst
Yigit Duzkoylu1*; Ali Imran Kucuk2
1Department of Gastroentrological Surgery, Balikesir Ataturk City Hospital, Turkey.
2Department of Oncological Surgery, Balikesir Ataturk City Hospital, Turkey.
*Corresponding Author : Yigit Duzkoylu
Department of Gastroentrological Surgery, Balikesir
Ataturk City Hospital, Turkey
Email: dryigit@gmail.com
Received : Feb 25, 2021
Accepted : Mar 29, 2021
Published : Mar 31, 2021
Archived : www.jcimcr.org
Copyright : © Duzkoylu Y (2021).
Abstract
Hydatid disease, mostly caused by Echinococcus granulosus, is a common parasitic infestation of the liver. In this type of infectious disease, humans are an intermediate host. Although most common sites are liver (70%) and lungs (25%), this parasitic tapeworm can be seen at any region of the body. Intraperitoneal cysts are usually secondary to the rupture of primary cysts, but primary hydatid cysts of the mesentery are very rare (%2). Herein, we aimed to report a giant primary hydatid cyst in a male patient, treated surgically without any complications.
Keywords: Hydatid Disease, Primary Mesenteric Cyst, Giant Hydatid Cyst.
Citation: Duzkoylu Y, Kucuk AI. A benign rare intraabdominal lesion: Primary giant mesenteric hydatid cyst. J Clin Images Med Case Rep. 2021; 2(2): 1040.
Introduction
Hydatid disease which is also named as hydatidosis, is a parasitic infection caused by tapeworms of the Echinococcus cestode [1,2]. Echinococcus granulosus is the most common form encountered in humans. The disease still has a wide distribution worldwide and endemic in some countries including South Africa, Australia, South America and Eastern Europe involving Turkey [2]. In this disease, humans are known as an intermediate host during the life cycle of the parasite. It is located primarily in the liver (70%) and lungs (25%) and starts to produce daughter cysts [1]. Secondary cysts can be seen at any anatomical site including every solid organ, vertebra, mesentery and soft tissues [3]. Intraperitoneal hydatid cysts are commonly secondary to the rupture of a primary liver cyst and primary mesenteric hydatid cyst is very rarely encountered [1-3]. In this case report, we aimed to report a giant primary mesenteric cyst in a male patient who was treated surgically and diagnosed as hydatid disease following histopathological evaluation.
Case presentation
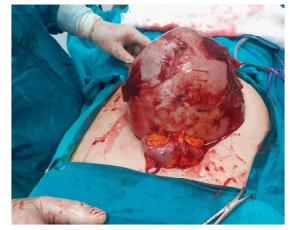
A 62-year-old male patient admitted to hospital with abdominal distention and intermittant abdominal pain lasting for 5 years. On the physical examination, his abdomen was diffusely tense without defense or rebound findings. He had no any other comorbidities or history of surgical procedure. Laboratory findings including liver function tests and tumor markers. Ultrasound examination revealed cholelithiasis and 18 X 16 cm cystic lesion located between supraumblical region to pelvis and sonographic evaluation was consistent with mesenteric cyst with the advice of contrasted computerized tomography for further evaluation. Contrasted tomography was performed and showed 19 X 15 cm cystic lesion which was thought to be originated from 3rd segment of duodenum and reported with differential diagnosis as dublication cyst or mesenteric cyst. Additionally, there was a 13 X 11 mm lesion on the 4th segment of the liver consistent with hemangioma. Neither laboratory test, nor antiparasitic therapy specific to hydatid disease were started because of those radiological findings which were not suspicious for the disease. Following preoperative assessment, midline laparatomy was performed under general anesthesia. Initial exploration revealed a giant cystic lesion originating from the mesentery of proximal small intestine and extending from the level of Treitz ligament to the pelvic inlet (Figure 1). The liver, spleen, pancreas, and both kidneys appeared to be normal and there were not any free fluid. Cyst was removed totally without any dehiscence or spillage (Figure 2). Histopathological examination revealed a 23 X 16 X 17 cm cystic material with 3150 g weight. Cystic wall was found to be 2 mm in thickness, consistent with acellular cuticle membrane without any solid or papillary lesions. Cystic fluid involved numerous scolex formations. The patient was dischaged on the day without any complications with albendazole 800 mg/day treatment. The duration of the treatment was planned to be 3 months and he was called to outpatient clinic for the control of liver function tests once a month.

Discussion
Hydatid disease or Echinococcosis is a parasitic disease caused by the cestode of Echinococcus granulosus in which humans are an intermediate host [4]. It is still considered to be endemic in some parts of the world including Middle East, South America and Mediterranean regions involving Turkey [5]. Mainly four different species can cause active infection in humans, which are Echinococcus granulosus (cystic hydatid disease), Echinococcus multilocularis, Echinococcus vogeli and Echinococcus oligarthus, considering the last two as very rare [6]. Humans are intermediate hosts during the life cycle of the cestode and infected following a contact with a definitive host such as dog or sheep, or by the ingestion of infected vegetables or water [7]. Although any anatomical region may be infected in the body, the most frequent site is the liver (upto 75%), followed by lungs (25-27%) [8,9]. Peritoneal and mesenteric hydatid cysts are more commonly secondary due to a primary liver cyst. They are usually caused by the rupture of this primary cyst [10]. Either primary or secondary, these cysts are considered as a significant manifestation of the disease (13%) [3]. Primary mesenteric cysts of Echinococcus granulosus account for 2% of all abdominal hydatidosis [11]. As it is seen in primary liver cysts, symptoms and complications are related with the location and size of the cyst. Mesenteric hydatid cysts may be completely asymptomatic with regard to their small size, or they can be diagnosed as a non-specific abdominal mass, causing pain due to larger size and pressure effect on the mesentery [1]. Imaging and serology are the main diagnostic tools. Ultrasound is usually effective in diagnosing hydatid cysts in the abdomen. Contrasted computerized tomography (CT) may be considered as the second line radiological tool when needed, showing the size, location and morphology of the cyst in detail.
In our case, the patient was a 62-year old male, with complaints of abdominal distention and intermittent abdominal pain. He did not have any comorbidities or history of surgery. Historyrevealed a long-term animal contact with sheeps during childhood. In our case, ultrasound and CT examinations were consistent with a giant primary mesenteric cyst, which led the physicians to have a lacking record of history and laboratory study such as indirect hemagglutination test for hydatid disease. Following a successful surgery without the rupture of the cyst, the exact diagnosis was reported as mesenteric hydatid cyst with histopathological examination. The cyst was considered was primary mesenteric hiydatid cyst because the CT examination did not show any other abnormal findings in other anatomical parts in neither abdomen, nor thorax. The patient was discharged from the hospital without any complications and kept on medical therapy with albendazole 800 mg per day and called to outpatient clinic once a month.
Conclusion
In endemic countries, hydatid cystic disease should always be kept in mind for the differential diagnosis in a patient with a cystic mass lesion at any anatomical region whatever the age of the patient, even if initial radiological studies do not reveal any suspicion as we had in our patient. Surgery is still accepted as the gold standard treatment in symptomatic cases.
References
- Kushwaha JK, Gupta R, Mohanti S, Kumar S. Primary mesenteric hydatid cyst. BMJ Case Rep. 2012.
- Velioglu M, Diktas H, Kabalak B, Tufekci H, Cermik H, Akar I, Yalcin B, Cosar A. Giant isolated mesenteric hydatid cyst case report without organ involvement. Turkiye Parazitol Derg. 2014; 38(3): 194-6.
- Abdelmaksoud MM, Jamjoom A, Hafez MT. Simultaneous Huge Splenic and Mesenteric Hydatid Cyst. Case Rep Surg. 2020; 7050174.
- Sielaff TD, Curley SA. Liver. In: Brunicardi FC, Andersen DK, Billiar TR, et al editors. Schwartz’s principles of surgery, 8th edition. New York: McGraw-Hill. 2005: 1163.
- Sozuer EM, Ok E, Arslan M. The perforation problem in hydatid disease. Am J Trop Med Hyg 2002; 66: 575-7.
- Khuroo MS. Hydatid disease: Current status and recent advances. Ann Saudi Med. 2002; 22: 56–64.
- Pedrosa I, S aíz A, Arrazola J, et al. Hydatid disease: radiologic and pathologic features and complications. Radiographics 2000; 20: 795–817.
- Kusaslan R, Sahin DA, Belli AK, Dilek ON. Rupture of a mesenteric hydatid cyst: a rare cause of acute abdomen. Can J Surg. 2007; 50(5): E3-4.
- Obradovic Z, Zerem E, Beslagic Z, Susic A. Echinococcosis in Bosnia and Herzegovina. Medicinski Arhiv. 2006; 60(4): 259-62.
- Yuksel M, Demirpolat G, Sever A, Bakaris S, Bulbuloglu E, Elmas N. Hydatid disease involving some rare locations in the body: a pictorial essay. Korean Journal of Radiology. 2007; 8(6): 531-40.
- Singh RK. A case of disseminated abdominal hydatidosis. J Assoc Physicians, India. 2008; 56: 55.